I
Name
:
______________________________
Class
:
_______________________________
"Pharmacology
NSAIDS (1)
Lecture
د
.
احمد الزهيري
NSAIDS (1
)
Mahmood Saied ® 2011
Page 2
Inflammation is triggered by the release of chemical mediators from
injured tissues and migrating cells. The specific mediators vary with the
type of inflammation. They include:
1. Amines (Histamine, 5HT)
2. Lipids (PGs)
3. Small peptides (bradykinin).
4. Large peptides (IL-1)
Drags that act on certain mediators will not affect the inflammation
process
involving other mediators.
Many NSAIDs act by inhibiting the synthesis of PGs. PGs and
related
eicosanoids are released in minute amounts by all tissues except RBCs,
they
are synthesized and inactivated in and same place so the circulating
level is
very small (i.e. PGs don't circulate in blood in significant level).
NSAIDs are group of dissimilar agents, they differ in the following
activities:
1. Antipyretic effect.
2. Analgesic effect.
3. Anti-inflammatory effect.
NSAIDs act by inhibiting the enzyme cyclo-oxygenase (COX), the
prototype of this group is
Aspirin
, the most commonly used and the
drug to which all other anti-inflammatory agents are compared. 15% of
patient show intolerance to aspirin, they may benefit from other NSAIDs.
Some of the newer NSAIDs are better than Aspirin in certain patients
either because of less gastric irritation of standard anti-inflammatory action or
can be taken less frequently, but they are still more expensive than Aspirin
and some are more toxic.
Aspirin and Salicylates

NSAIDS (1
)
Mahmood Saied ® 2011
Page 3
Aspirin is a weak organic acid
irreversibly
acetylate (inactivate) Cox
,mainly COX-1, while other NSAIDs, including salicylates are
reversible
inhibitors for COX enzyme.
Aspirin is rapidly deacetylated by Esterase to produce salicylates with
are still active (have anti-inflammatory, Antipyretic and Analgesic effects).
Kinetics:
Salicylates are rapidly absorbed from the stomach and upper part
of the small intestine yielding a peak plasma conc. within 1-2 hrs.
The acidic medium in the stomach (PH= 1.5) keeps large fraction of
salicylates in non-ionized from (lipid soluble) so it diffuses easily
and absorption is promoted.
when high conc. of salicylates enter the mucosal cells, the drug may
damage the mucosal barrier and result in gastric ulcer.
If gastric PH is raised by suitable buffer to 3.5 or higher gastric
irritation will be minimized (less absorption → less irritation).
After absorption of aspirin it is hydrolyzed into acetic acid and
salicylates, salicylate binds to albumin but as serum conc. of
salicylates increases, a greater fraction remain unbound and available to
tissue.
Ingested salicylates and that generated by hydrolysis of aspirin may
excreted unchanged, but most is converted to water soluble
conjugates that are rapidly cleared by the kidney. When this
pathway becomes saturated, a small increase in aspirin dose result
in large increase in plasma level.*
Urine alkalinization will prevent reabsorption of salicylates.
When aspirin is used in low doses (less than 600 mg) then it will
follow the 1
st
order kinetics (t
1/2
3-5 hrs), while at higher doses it
will follow zero order kinetics (t½= 15 hrs).
The t
1/2
also depends on the status of the kidney and liver. The ↑ in
t
1/2
(at high aspirin doses) → occurs about after week (till the
saturation of the hepatic enzymes) that will lead to the formation of
NSAIDS (1
)
Mahmood Saied ® 2011
Page 4
calicyluric conversion compounds salicyl phenylglucuronide and
salicyluric acid.
* see the diagram in the next page.
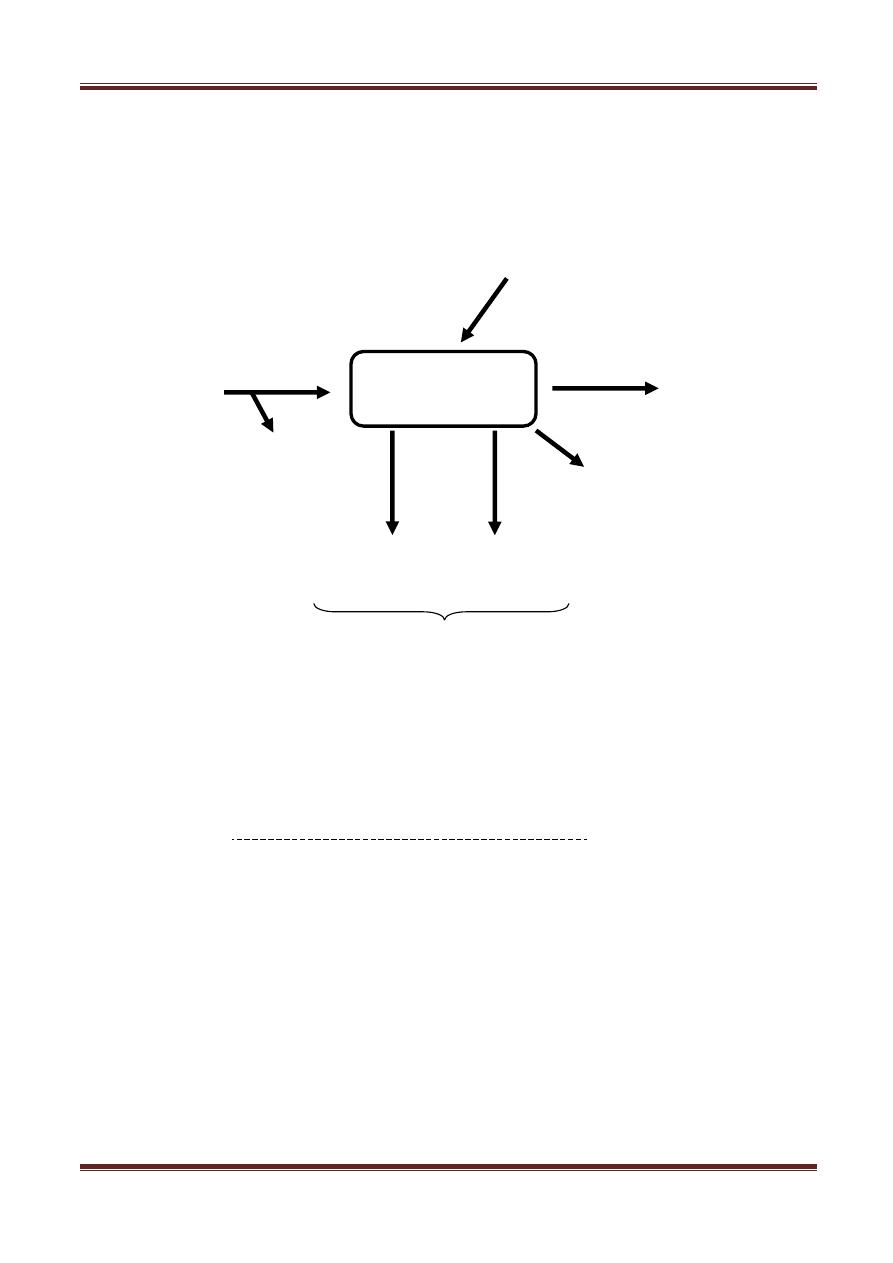
Metabolism of Aspirin:
These are the major 2 pathways in the aspirin metabolism
Dynamics "Action of Aspirin & salicylates"
1) Anti-inflammatory effect:
The effectiveness of Aspirin is largely due to its capacity to inhibit PGs
synthesis. It irreversibly blocks enzyme COX which catalyze the
reaction of AA to cyclic endoperoxide compounds.
In high doses, Aspirin ↓ the formation of PGs and TXs (TXA
2
).
It also interferes with chemical mediators of Kallikrein synthesis.
It inhibits granulocytes adherence to damaged vasculature and
stabilizes
lysosomes and inhibits migration of polymorphonentrophlils
(PMN)
WBCs
& macrophages to site of inflammation.
Na salicylate
Oxidation
hydrolysis
Aspirin
Gentectic acid
1%
Salicylate
gl
u
cu
ro
n
id
e
Co
n
ju
ga
ti
o
n
Co
n
ju
ga
ti
o
n
G
ly
ci
n
e
Free salicylate
Salicyluric
acid
Ester & ether
glucuronide
Acetic acid
NSAIDS (1
)
Mahmood Saied ® 2011
Page 5
2) Analgesic effect:
Aspirin is the most effective in reducing pain of mild to
moderate
intensity
(not severe pain).
It alleviates pain of varying causes: muscular, dental post parum,
arthritis and bursitis. But it is not useful for visceral pain.
Aspirin acts
peripherally
through its effect on inflammation but
probably also depresses pain stimulation at a subcortical level site.
By ↓ PGE
2
synthesis, Aspirin and other NSAIDs depress sensation of
pain.
NSAIDs are superior to opioids is the management of pain due to
inflammation. (have max. efficacy more than that of opioids).
NSAIDs are combined with opioids in treating pain in malignancy.
3) Anti-pyretic effect:
Aspirin decreases (↓) elevated temperature
in case of fever
whereas normal body temperature is only slightly affected.
The fall in temperature is related to increased dissipation of heat
caused by vasodilation of the superficial blood vessels. Anti-pyresis
may be combined sweating.
The fever associated with infection is through to result from 2 action:
a) from production of PG in the CNS in response to bacterial pyogens.
b) through the effect of IL-1 on hypothalamus (IL-1 is produced
during inflammation by macrophages to activate lymphocytes but ↑
temp).
Aspirin blocks the CNS response to IL-1, so it may reset the temp.
control
in hypothalamus thereby facilitating heat dissipation by
vasodilation.

NSAIDS (1
)
Mahmood Saied ® 2011
Page 6
4) Anti-platelet effect:
Aspirin affects hemostasis, single dose aspirin produces a slightly
prolonged bleeding time which doubles if administration is
continued for a week.
This change is explained by inhibition of platelets aggregation,
secondarily to inhibition of TXA
2
synthesis (TXA
2
accelerates platelet
aggregation).
Aspirin inhibits platelet aggregation up to 8 days till the formation
of new platelet.*
Aspirin has long duration of action when compared with other
agents used to inhibit platelet aggregation such as: clofibrate,
phenylbutazone, dipyridamole.
* platelet life span 8 days, thus continuous anti-platelet effect is readily achieved with low doses.
5) Respiratory Effect:
Therapeutic does ↑ alveolar ventilation, higher does acts directly on
respiratory centre (in medulla) causing hyperventilation and respiratory
alkalosis, toxic dose cause central respiratory paralysis and metabolic
acidosis, due to continuous CO2 production.
6) GIT effects:
PGI
2
inhibits gastric secretion, PGE
2
stimulates synthesis of
protective mucosa in the stomach and intestine.
In presence of Aspirin, both PGI
2
and PGE
2
are not formed and this
will
lead to ↑ gastric acid secretion and ↓ mucous production → so this may
cause: epigastric distress, ulceration and hemorrhage.
With ordinary doses of Aspirin, 3-8 ml of blood may be lost with feces
every

NSAIDS (1
)
Mahmood Saied ® 2011
Page 7
day.
Buffered and Enteric coated Aspirin preparations, that delay
absorption of
aspirin to the upper small intestine, are only partially helpful and more
expensive.
Misoprostol (PGE derivative) is used for treatment of gastric damage
induced by NSAIDs.
7) Action on kidney:
Inhibition of COX prevents the synthesis of PGI
2
and PGE
2
which are
responsible for maintaining normal renal blood flow (especially in the
presence of vasoconstrictors)
Diminished synthesis of above PGs can result in Na
+
and water retention
causing edema and hypokalemia in some patients.
Clinical uses of Aspirin:
1. Analgesic and anti inflammatory:
I.
Analgesic effect:
Aspirin most frequently is used to reduce mild to moderate pain
*
.
Aspirin may be combined with other analgesics (as opioids) and
called as OTC drugs (out of the counter drugs that are solid with
prescriptions).
These combination are not more effective or less toxic than aspirin
but they are only more expensive. The disadvantage of these

NSAIDS (1
)
Mahmood Saied ® 2011
Page 8
combinations is that poisoning with them is difficult to treat
because we don't know exactly what member is the true cause of
poisoning.
Aspirin is not effective in the treatment of visceral pain such as
(acute abdomen, MI, or renal colic).
II.
anti-inflammatory action
of salicylates in high dose are
responsible for their recommendations as initial major therapy in
rheumatoid arthritis, acute rheumatic fever and other inflammatory
conditions.
2. Other indication:
a)
Antipyretic:
aspirin is the best available drug for ↓ fever.
b)
Inhibition of platelet aggregation:
aspirin used in
1)
transient
ischemic
attacks (TIAs) and
2)
unstable angina
**
.
c)
External application:
salicylic acid is used topically for treatment
of
corns and calluses epidermititis.
Methyl salicylic acid (oil of wintergreen) is used externally as
counter irritant in ointments.