I
Name
:
______________________________
Class
:
_______________________________
"Pharmacology
NSAIDS (2)
Lecture
د
.
احمد الزهيري
NSAIDS (2)
Mahmood Saied ® 2011
Page 2
Dosage of Aspirin:
Optimal analgesic dose or antipyretic dose is less than 0.6 gm orally
(commonly used).
Large dose will prolong the effect.
Usual does can be repeated every 4 hrs and smaller doses (0.3 gm ) every 3
hrs.
Children dose (50-75 mg / kg/day) in divided doses (at least three).
Anti- inflammatory dose (4 gm/day) is fairly tolerated by adults.
Blood levels of 15-30 mg/dl are enough for anti-inflammatory effect.
Due to long t½ (about 12 hrs) of aspirin and its metabolites, frequent dosing is
not required
If daily doses needed are of 4 gm or more, it is better to give the total amount
in 3 divided doses and to be taken after meals (meals act as buffer to ↓ adverse
effect on GIT).
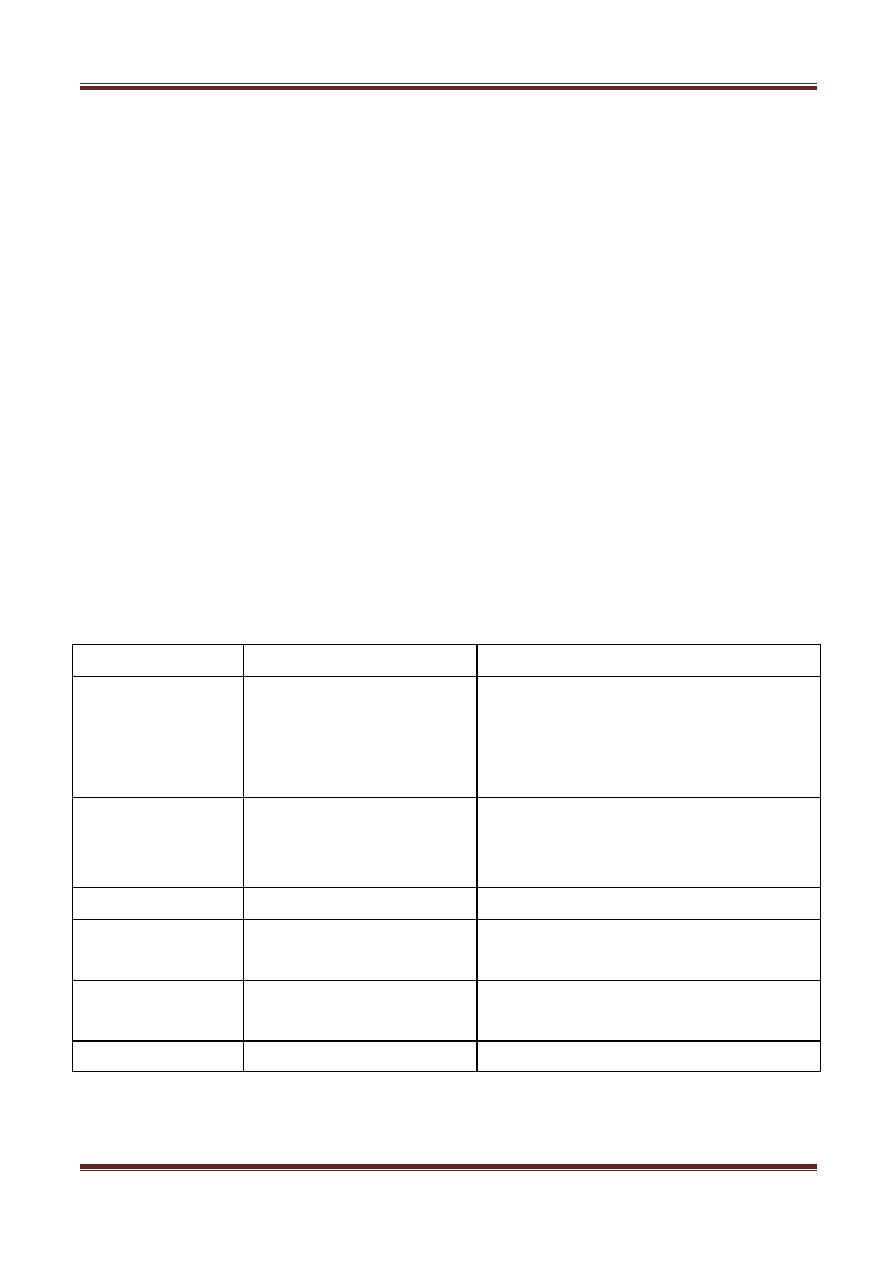
Relationship of plasma salicylates level to dynamics and complications:
Salicylate level
Effect
Complication
0-10 mg/dl
analgesic,
antiplatelet
aggregation,
antipyretic
gastric intolerance, bleeding,
allergy (hypersensitivity reactions)
and impaired hemostasis
10-50 mg/dl
anti-inflammatory,
uricosuric,
Rheumatoid Arthritis
gastric intolerance, bleeding,
allergy (hypersensitivity reactions)
and impaired hemostasis
50-80 mg/dl
mild intoxication
central hyperventilation, tinnitus
80- 110 mg/dl
moderate intoxication fever, dehydration and metabolic
acidosis
110-160 mg/dl
sever intoxication
vasomotor collapse coma and
hypoprothrombinemia
>160 mg/dl
lethal intoxication
renal and respiratory failure
NSAIDS (2)
Mahmood Saied ® 2011
Page 3
Adverse Effects of Aspirin:
1. On GIT:
At usual doses, Aspirin cause
gastric intolerance
(minimized by
suitable buffering food or milk).
Gastritis
/ associated with Aspirin therapy is due to:
1.
Undissolved tablets.
2.
stomach absorption of non-ionized salicylate.
3.
inhibition of protective PGs (I
2
and E
2
).
Vomiting
may occur due to CNS stimulation after absorption of large
doses.
Upper GIT bleeding
usually due to large doses leading to erosive
gastritis.
Blood loss associated with Aspirin therapy (1 ml daily) increases
to (4 ml daily) with usual doses and more for higher doses.
2. On CNS:
Higher doses cause
"salicylism"
→ ↓ hearing, vertigo (these are
reversible when dosing is reduced or stopped).
Large doses cause
"
hyperapnea
"
by direct effect on medulla.
Low toxic doses causes
respiratory alkalosis
which cause increased
ventilation, then
acidosis
(metabolic)
due to accumulation of salicylic acid
derivatives & then
depression of respiratory centre
.
3. other side effects:
Aspirin in doses of 2 mg/day or less increases serum level of uric
acid(inhibiting its secretion).
Whereas by the doubling doses exceeding 4 mg/day, it decreases urate
blood level below 2.5 mg/dl & this is known as
(paradoxic effect of aspirin)
inhibiting its reabsorption.
15 % of patients show hypersensitivity, so they are benefited from using
other NSAIDs .

NSAIDS (2)
Mahmood Saied ® 2011
Page 4
Aspirin given during viral infection causes increased incidence of
Reye's syndrome
(fatal hepatitis with cerebral oedema) in children (so they
should take Acetaminophen instead of Aspirin).
Toxic doses directly depress cardiac function & dilate peripheral blood
vessels.
Lareg doses directly affect smooth m.
Hypersensitivity occurs in patients with asthma, nasal polyps (broncho-
constriction & shook) mediated by leukotriens.
Note:
Since Aspirin inhibit cyclo-oxygenase (COX) so all arachidonic acids possibly
metabolized by 5-lipoxygenase leading to excess leukotrien production.
Contraindications of Aspirin:
1. In hemophilia patients, since it causes blood loss.
2. Pregnancy, because it may lead to fetal malformation in the first 3 months of
pregnancy. Acetaminophen is preferred.
3. Peptic ulcer.
Over Dose & toxicity of Aspirin:
1. Serious intoxication occurs when the amount ingested exceeds 150-175
mg/kg (gastric lavage is devised).
2. Hyperthermia is treated with a topical sponges or ice patches.
3. Also, maintain high urine volume & treat acid base abnormality.
4. In severe toxic reaction, ventilatory assisstant may be recommended
NaHCO
3
infusion may be employed infusion to alkalinize urine & ↑ secretion
of salicylates.

NSAIDS (2)
Mahmood Saied ® 2011
Page 5
Drag interaction:
1. Drugs enhance salicylate intoxication as acetazolamid and NH
4
Cl.
2. Alcohol increase GIT bleeding induced by aspirin.
3. Aspirin displace some drugs from protein binding sites: tolbutamide,
phenytoin, clorpropamide, NSAIDs, methotrexate, probenecid) and thus ↑
their free amount → ↑ their effects.
4. Aspirin ↓ activity of spironolactone and intensify the effects of heparin.
5. Aspirin competes with penicillin G for renal tubular secretion and inhibits
uricosuric effect of sulphinpyrazon and probenecid.
Newer NSAIDs
Adverse effects of Aspirin have led to search for alternative compounds. In
1971 Ibuprofen and several other aspirin-like drugs were introduced later.
Chemistry: they are grouped in several classes, which are chemically diverse
and broad variety in their Kinetics & properties
Dynamics :
1. Their anti-inflammatory activity is similar to aspirin in mechanism (i.e.
by inhibition of PGs synthesis).
2. inflammation is reduced by ↓ release of mediators produced by
granulocytes, basophils & mast cells.
3. they ↓ sensitivity of vessels to bradykinin and histamine.
4. All are analgesics, anti-inflammatory, antipyretics and all inhibit
platelet aggregation.
5. All are gastric irritants, but less than aspirin.
6. Nephrotoxicity is observed for all of them.
7. Affect lymphokin production from T- lymphocytes and reverse
vasodilation.
8. Thy inhibit prothrombin synthesis.
Ibuprofen: t
1/2
= 2 hrs

NSAIDS (2)
Mahmood Saied ® 2011
Page 6
An analgesic, but inferior as anti-inflammatory agent t
1/2
.
Ibuprofen, when used in 2-4 gm/day, it equals 4 gm of aspirin as anti-
inflammatory, but causes less gastric irritation.
Metabolized by liver & abut 10% of it is excreted in urine unchanged.
GIT irritation & bleeding occurs, but less than Aspirin.
Contraindicated in
patients with nasal polyps (because it affect
airways) angioedema and bronchospastic reactivity of aspirin.
GIT symptoms:
rash, dizziness, headache, anxiety and fluid retention also reported.
Interaction with anti-coagulants is uncommon.
It also cause serious hemolytic effect granulocytosis, aplastic anemia,
effects on kidney: renal failure, nephritis, nephrotic syndrome.
Naproxen: t
1/2
= 13 hrs
Binds to plasma protein,
t
1/2
= 13 hrs.
Antacids delay its absorption.
Excreted in urine as inactive glucuronid metabolites.
Competes with aspirin for plasma protein binding sites & it
prolong prothrombin time.
Average doses for inflammatory arthritis is 375 mg twice a day.
Fenoprofen: t
1/2
= 2 hrs (needs multiple dosing)
Dose for inflammatory arthritis = 600-800 mg 4 times daily.
Adverse effects for naproxen and fenoprofen are similar to these of Ibuprofen.
Indomethacin:
t
1/2
= 2 hrs
more toxic than aspirin.

NSAIDS (2)
Mahmood Saied ® 2011
Page 7
more effective than aspirin and other NSAIDs.
the most potent inhibitor of PGs synthesis especially (in vitro).
well absorbed orally, high bound to plasma proteins, metabolized in liver
and excreted unchanged or as inactive metabolites (excreted in bile & in
urine).
Clinical uses:
-
not suggested for general use as analgesic except for the treatment of
patent ductus arteriosus.
-
should not be used in children.
-
useful in
acute gouty arthritis, ankylosing spondylitis &
osteoarthritis.
In acute gout, it is replaces (colchicin) as the initial medication.
Adverse Effects:
1. produce high incidence of dose-related toxic effect.
2. At higher dose, 30% of patients have reactions requiring discontinuation of
therapy.
3. GIT effect are abdominal pain, diarrhea, GIT hemorrhage.
4. Severe headache is experience in 20-25 % of patients (may be with
confusion, dizziness & depression).
5. Hemolytic reactions are noted (thrombocytopenia & aplastic anemia).
6. Coronary vasoconstriciton also demonstrated.
7. Hyprekalemia is also reported due to inhibition of PGs & its effects on
kidneys.
Etodolac:
Similar to the effects of other NSAIDs, GIT problems are less common.

NSAIDS (2)
Mahmood Saied ® 2011
Page 8
Adverse effect: fluid retention, abnormal kidney and liver functions are
reported.
It may increase serum level & adverse effect of digoxin, lithium,
methotrexate, and enhance nephrotoxicity of cyclosporines.
Diclofenac:
Approved for
long term treatment of osteoarthritis, ankylosing
spondylitis & rheumatoid arthritis
More potent than indomethacin or naproxen.
It accumulates in synovial fluid so cause healing of arthritis.
Eliminated by urine.
Toxicity: similar to other NSAIDs.
GIT problems are common & it causes rise in hepatic enzymes level.
Ketorolac:
Its action is similar to other NSAIDs, it is given orally & IM in treatment of
postoperative pain and given topically in treatment of allergic
conjunctivitis.
it is metabolized by liver and eliminated in urine.
Side effect: like other NSAIDs.
Nebumeton:
as potent as aspirin in treating adult or juvenile rheumatoid
arthritis or osteoarthritis with few side effect.
Sulindac:
It is a prodrug effective only after conversion to sulfide by liver enzyme.
Excreted in bile and then reabsorbed from intestine.
The enterohepatic cycling prolongs its duration of action up to 16 hrs.
Indication and adverse effect are similar to other NSAIDs.
The dose for inflammatory arthritis = 200 mg twice daily (bid).
Mefenamic Acid (ponstan):
It has analgesics properties .

NSAIDS (2)
Mahmood Saied ® 2011
Page 9
It is less effective than aspirin as anti-inflammatory agent .
It is more toxic, not to be used for longer than 1 week & never used in
children below 12 years.
Meclofenate: t
1/2
= 2 hrs
It reaches peak plasma conc. in 30–60 min after administration.
Excreted in urine.
It has similar adverse effect to other NSAIDs, with no advantage over
time.
It enhances effects of oral anti-coagulants.
Contraindicated in pregnancy.
Dose for inflammatory arthritis = 200-400 mg/day divided into 4 doses
(qid).
Tolmetin: t
1/2
= 1 hr
Similar to aspirin as anti-inflammatory agent.
adult dose is 400 mg, 4 times daily (qid).
Piroxicam: t
1/2
= 24 hrs
Long t
1/2
=24 hrs.
Because of long t 1/2 , it is used once a day.
Rapidly absorbed from stomach & reaches 80% of peak plasma conc. in 1
hr.
Used for rheumatoid disease and musculoskeletal disorders.
Adverse effect, as GIT effects, occur in 20 % of patients, (headache
and rash).
Diflunisal: t
1/2
= 8-12 hrs
like Aspirin, it has analgesic & anti-inflammatory effects.
It is indicated in pain & osteoarthritis.
Adverse effects: similar to other NSAIDs.
COX-2 Selective inhibitors:

NSAIDS (2)
Mahmood Saied ® 2011
Page 10
Coxibs
were developed to inhibit prostacyclin synthesis at site of
inflammation without affecting the action of the constitutively active
"housekeeping" COX-1 isoenzyme found in GIT, kidneys and platelets.
COXIBs selectively bind to and block the active site of the COX-2 enzymes
much more effectively than that of COX-1.
Coxibs have analgesic, antipyretic and anti-inflammatory effects (have
fewer GIT side effect).
They have NO effect on platelets aggregation.
Because COX-2 is constitutively active within the kidney, COX-2 inhibitors
cause renal toxicities similar to traditional NSAIDs.
Also, it has been found that a higher incidence or cardiovascular thrombotic
events associated with COX-2 inhibitors (rofecoxib).
Celecoxib:
highly selective COX-2 inhibitor (10-20 times more selective for CXO-2 than
COX-1).
It has a t
1/2
of 11 hrs and 27% of its dose excreted in urine (unchanged).
It is effective as the NSAIDs in rheumatoid arthritis and osteoarthritis
(cause fewer endoscopic ulcer than other NSAIDs).
It may cause rashes (salfomamide).
Etoricoxib:
A second generation COX-2 selective inhibitor with the highest selectivity
ratio of any Coxib for inhibition of COX-2 relative to COX-1.
It is extensively metabolized by hepatic P
450
enzymes and excretion is
renal (t
1/2
= 22 hrs ).
It is used for the treatment of signs and symptoms of osteoarthritis, gouty
arthritis, relief of acute musculoskeletal pain.
Meloxicam:

NSAIDS (2)
Mahmood Saied ® 2011
Page 11
This agent shown to inhibit COX-2 more than COX-1 (especially at lower
doses).
it is not as selective as other coxibs, it is used for the treatment of most
rheumatic diseases.
its use is associated with fewer clinical GIT symptoms & complications
than piroxicam, diclofenac and naproxen.
t
1/2
= 20 hrs.
Rofecoxib:
A potent, selective COX-2 inhibitor, it is approved for the treatment of
asteoarthritis and rheumatoid arthritis.
it is an analgesic and antipyretic, it has no effect on platelets aggregation
and small effect on GIT PGs.
At high dose, it causes edema and hypertension (occasional).
Other toxicities, similar to other coxibs .
t
1/2
= 17 hrs .
Valdecoxib:
A new, highly selective COX-2 inhibitor.
t
1/2
= 8-11 hrs and 90% eliminated unchanged by kidney.
GI and other toxicities are similar to other coxibs with no effect on
platelets (bleeding time)
In treatment of dysmenorrheal, it is as effective as non selective NSAIDs
for this indication.
Non-Narcotic Analgesics
NSAIDS (2)
Mahmood Saied ® 2011
Page 12
o
They have little or even no anti-inflammatory effect (unlike NSAIDs).
o
They have therapeutic advantages over narcotic analgesics (not causing
dependence or tolerance).
o
These are Acetaminophen & phenacetin.
Acetaminophen:
Mechanism of action:
Act by inhibiting PG synthesis in the CNS (this explains its anti-pyretic
and analgesic properties).
It has less effects on COX enzyme in peripheral tissue and this accounts
for is weak anti-inflammatory effect.
It doesn’t affect platelet function or increase blood clotting time & also
lacks side effect of aspirin & doesn’t cause treatogenicity (i.e. it doesn’t
increase bleeding time so producing no effect on bleeding time).
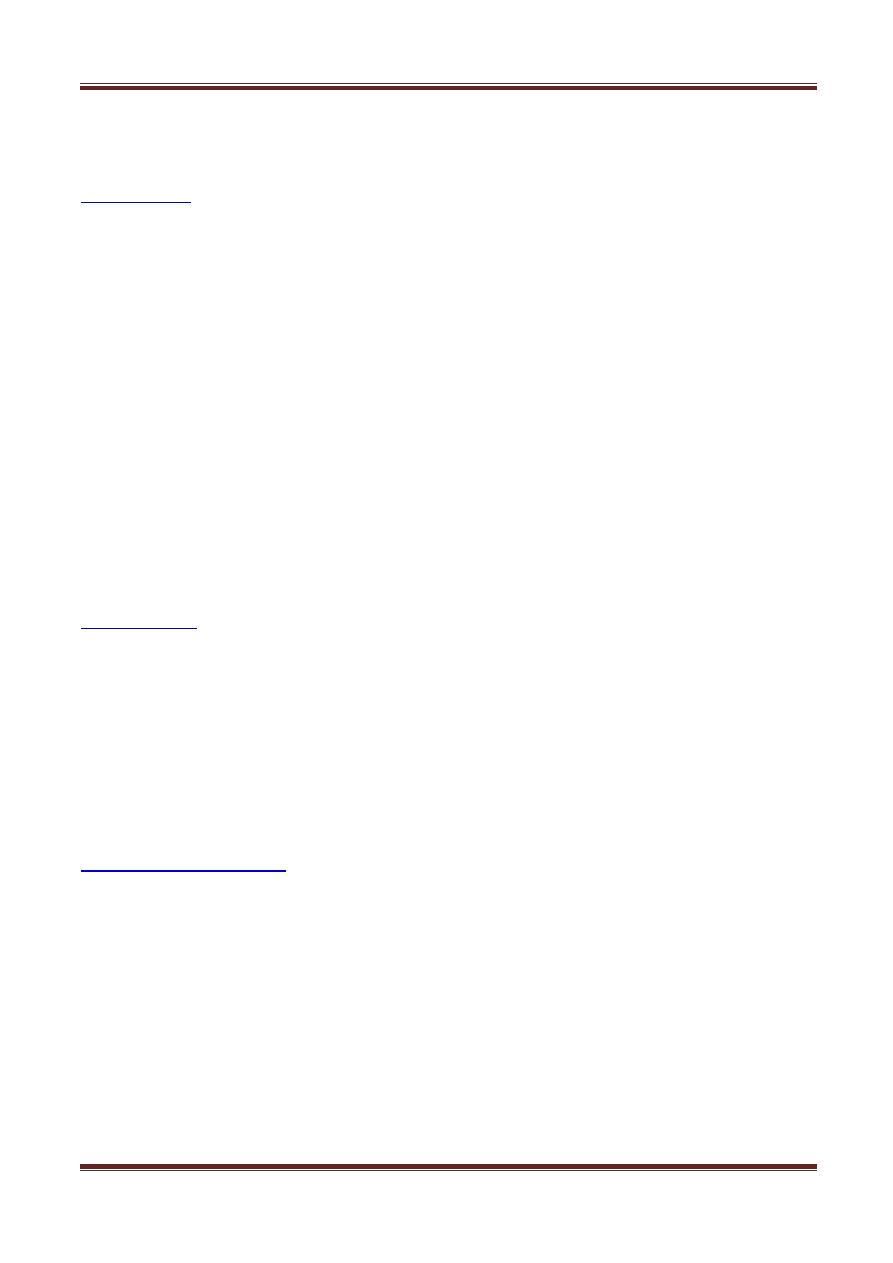
Major Differences between and Aspirin and Acetaminohen: مهم
feature
Aspirin
Acetaminophen
Site of inhibition
peripherally
centrally
COX inhibition
irreversible
reversible
Effect on inflammation
yes
no
Effect on platelet agg.
yes
no
Effect on bleeding time
yes
no
Side effects (SE)
too many
Few and in ↑ dose
Uses:

NSAIDS (2)
Mahmood Saied ® 2011
Page 13
1. Suitable substitute for aspirin as antipyretic and analgesic especially
in patients with gastric problems and prolongation of bleeding time.
2. It is the drugs of choice (as analgesic & antipyretic) in children with
viral infection or chicken pox.
3. It doesn’t antagonize uricosuric agents probenecid and may be used in
gouty patients using proberecid.
Kinetics:
Rapidly absorbed from GIT, 1
st
pass metabolism occurs in luminal cells
of the intestine and hepatocytes.
Conjugated in liver and a portion is hydroxylated to N-acetyl
benzoquineimine (NABQI) which is highly reactive & dangerous
metabolite with sulfhydryl group of glutathione forming non toxic
substance.
Excreted in urine.
Adverse Effects:
1) At normal therapeutic doses, are nearly without side effects.
2) Skin rash and minor allergic reaction occur rarely.
3) Renal tubular necrosis and hypoglycemic coma are rare complication with
prolonged large dose therapy.
4) With large doses, the available glutathione in the liver is depleted and
NABQI reacts with sulfhydryl (SH) groups of hepatic proteins forming
covalent bonds → leading to hepatic necrosis and very serious life-
threatening condition can result.
5) Also renal tubular necrosis may occur.
NSAIDS (2)
Mahmood Saied ® 2011
Page 14
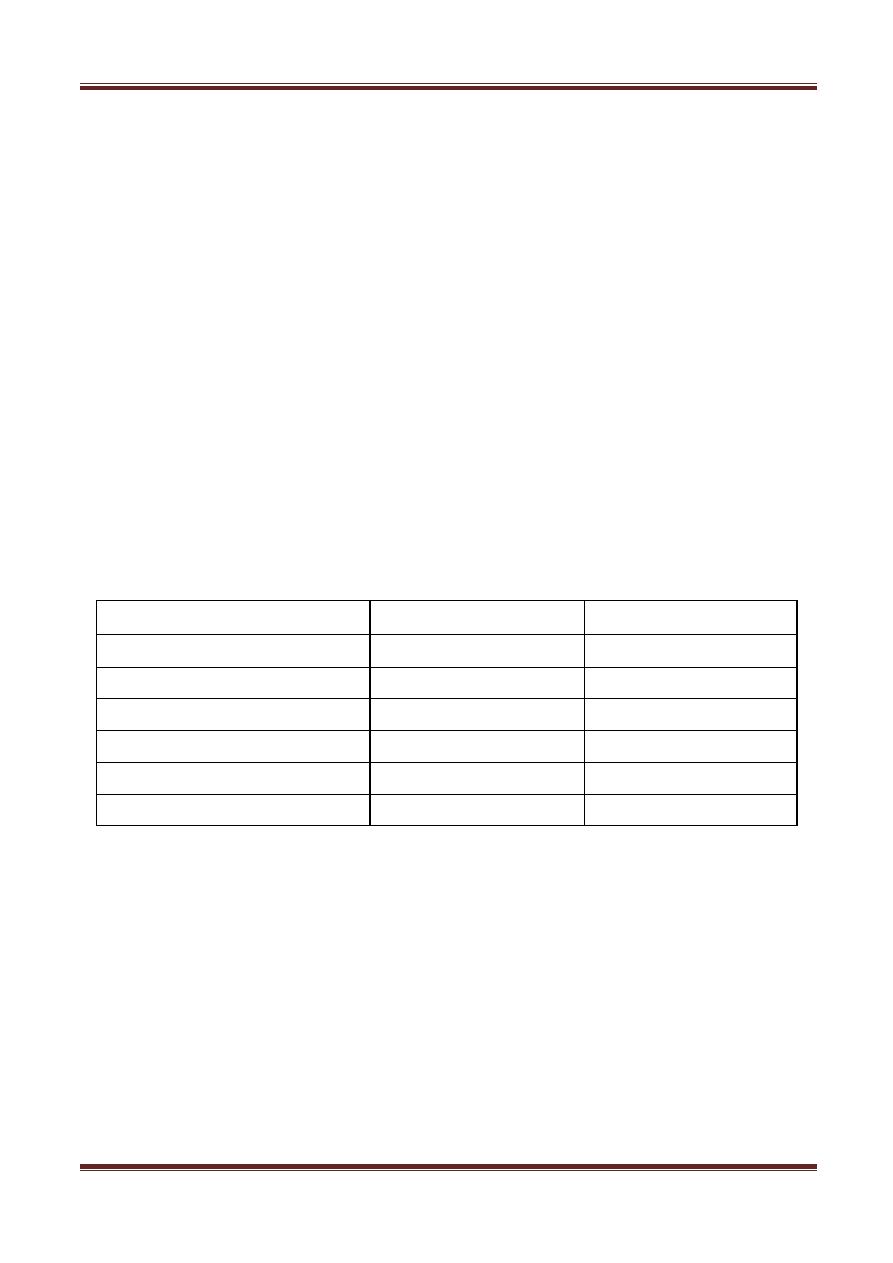
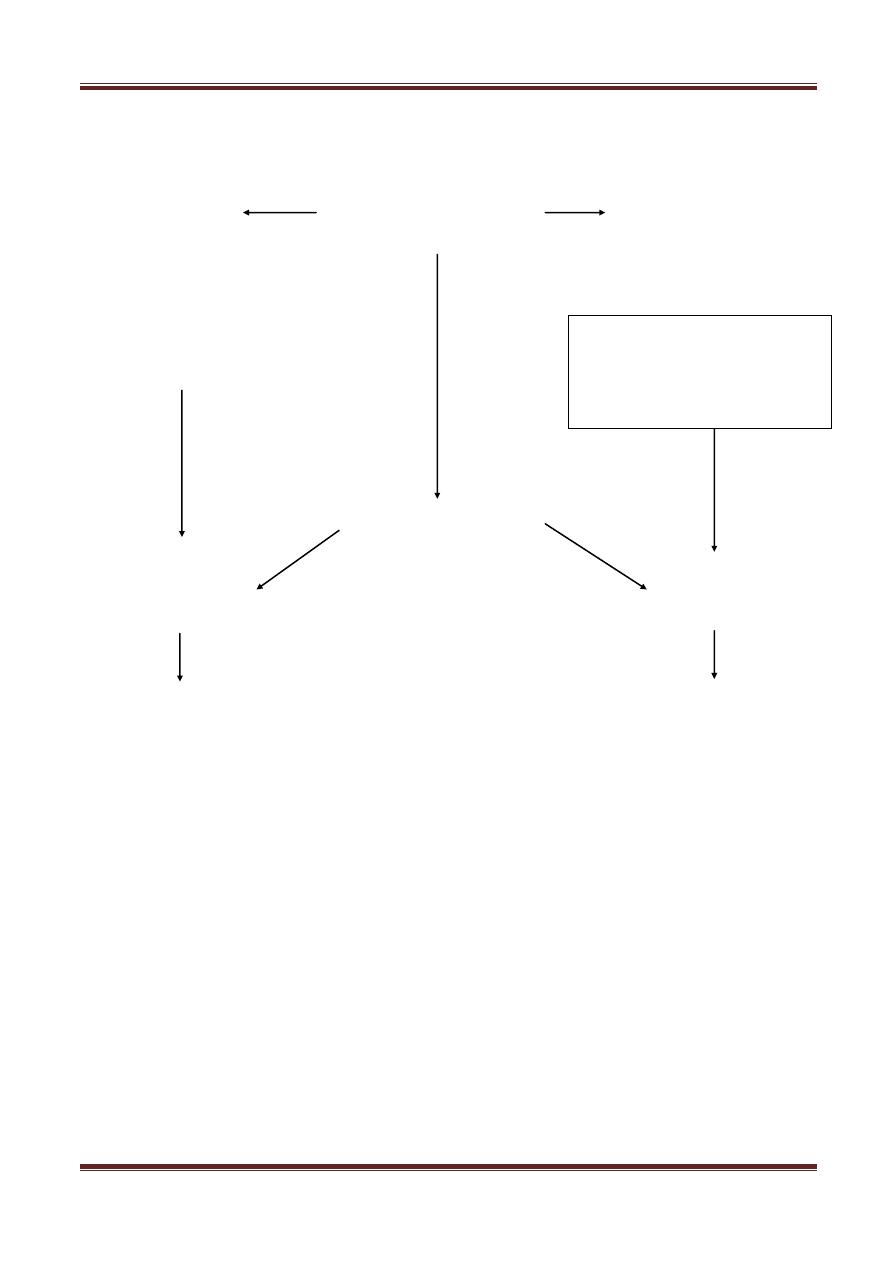
Metabolism & Excretion of Acetaminophen:
Sulfate
Acetaminophen
Glucouronide
Glutathion nucleophilic
Hepatic cell proteins
toxic intermediate
therapeutic dose toxic dose
-----------
This lecture was revised by Dr. Ahmed
himself, edited by Qatooooob
Cytochrome P
450
(mixed oxidase
function)
Mercapturic
(non- toxic )
Macromolecular
Cell death