
1
Immune Deficiency
Learning Objectives
Terms: primary and secondary ID
C/P
Causes
Sequelae
Quiz
2

3
1)
Recurrent infections
:
Frequent, severe, by unusual organisms
& at unusual sites
2)
Autoimmunity
3) Susceptibility to
malignancy
Clinical features of immune defificency:
4
Causes of immune deficiency
:
Primary :
Phagocyte ↓
Complement Pathway ↓
Adaptive IS ↓
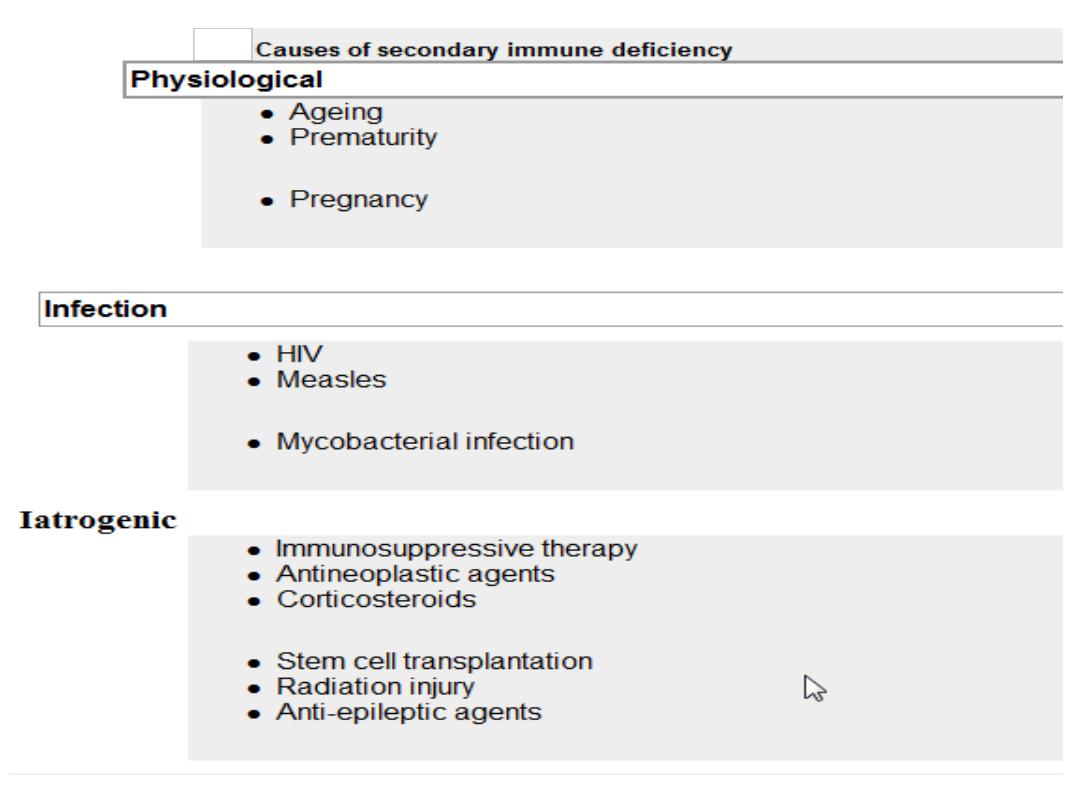
Secondary:
Physiological
Infection
Iatrogenic
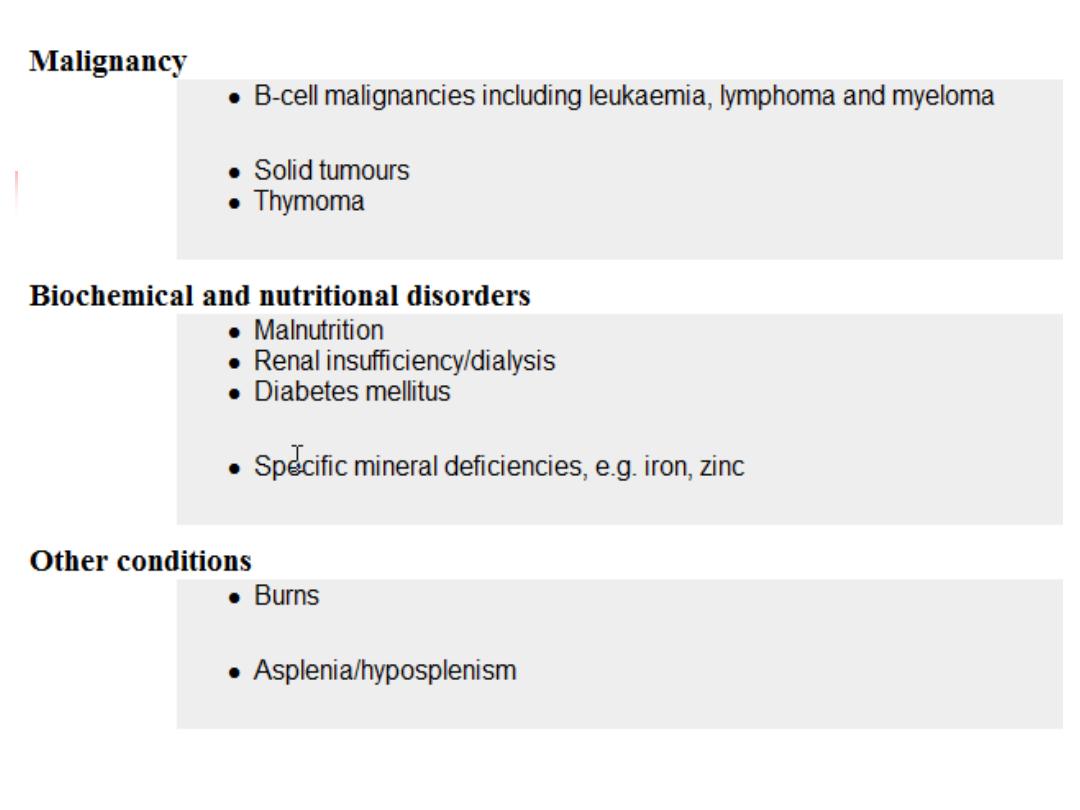
Malignancy
Biochemical & Nutritional
Others
5
6
A. Phagocyte ↓
↓WBC Adhesion Chronic Granul Dis ↓ Cytokine & Cytokine
receptors
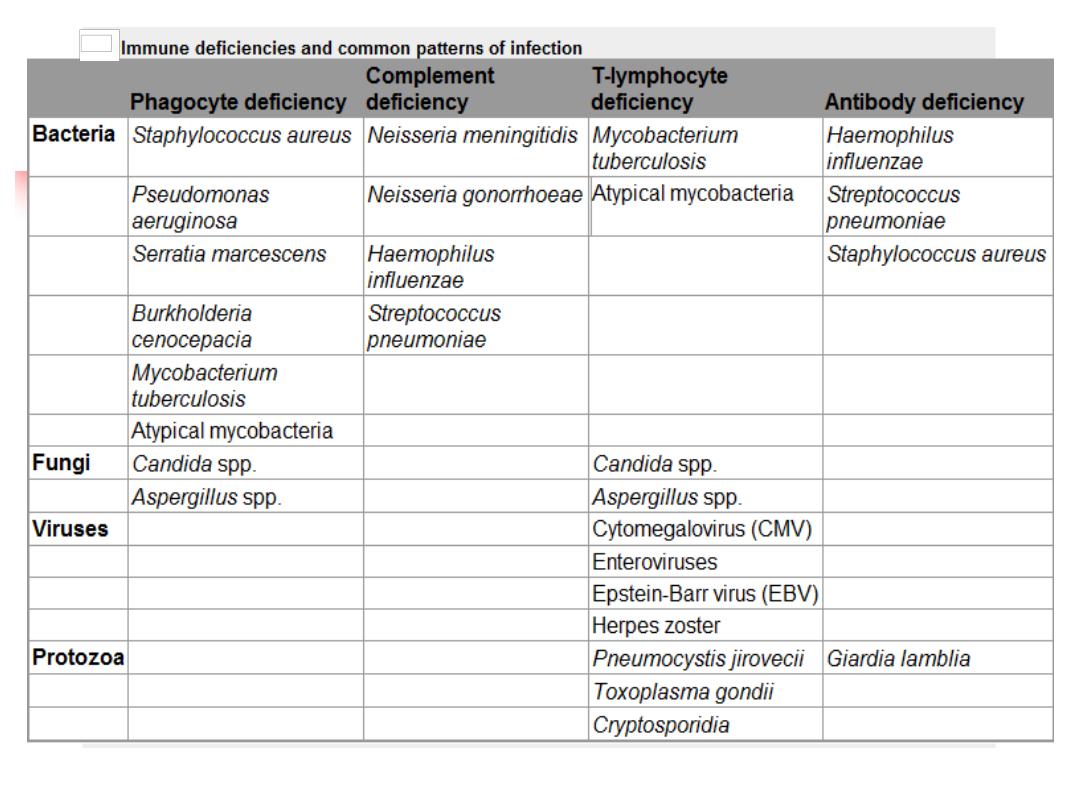
Staphyl.aureaus
Aspegillus
Bacterial Infection TB TB
7
A.Phagocyte
↓ sequlae
:-
1)↓WBC Adhesion
------- infection
2
) Chronic granulomatous disease
Catalase-positive organisms like
Staphyl. aureus
&
aspergillus.
Intracellular killing of mycobacteria in macrophages is also
impaired.
Infections most commonly involve the lungs, lymph nodes,
soft tissues, bone, skin and urinary tract
3) Defects in cytokines and cytokine receptors
------failure of intracellular killing -----mycobacterial
infections
8
9
Management:
1)
Drugs:
IV AB, Longterm prophylaxis with antifungal
agents, and trimethoprim-sulfamethoxazole.
2)
Surgical
drainage of abscesses
3)
Specific
treatment depends upon the nature of the
defect.
4)
and
stem cell transplantation
10
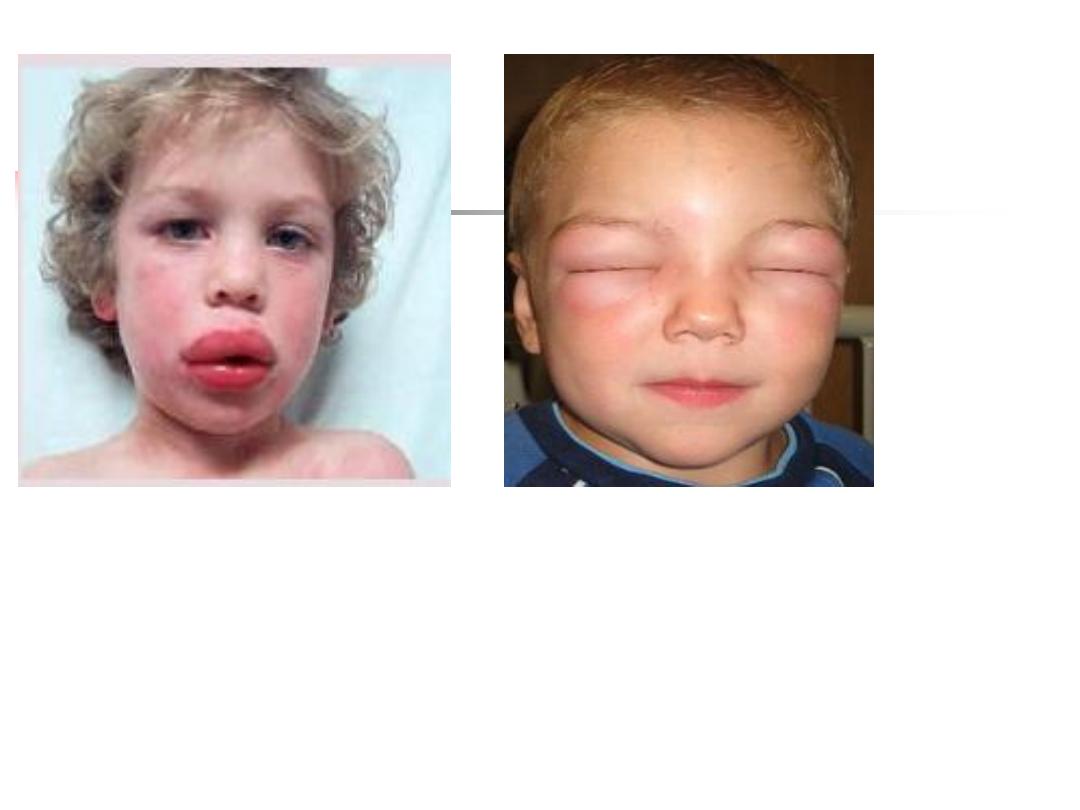
B. Complement Pathway ↓
Genetic deficiencies.
Deficiency of the
regulatory protein C1 inhibitor
--
recurrent angioedema.
C1, C2 and C4
------
autoimmune disease
(severe SLE)
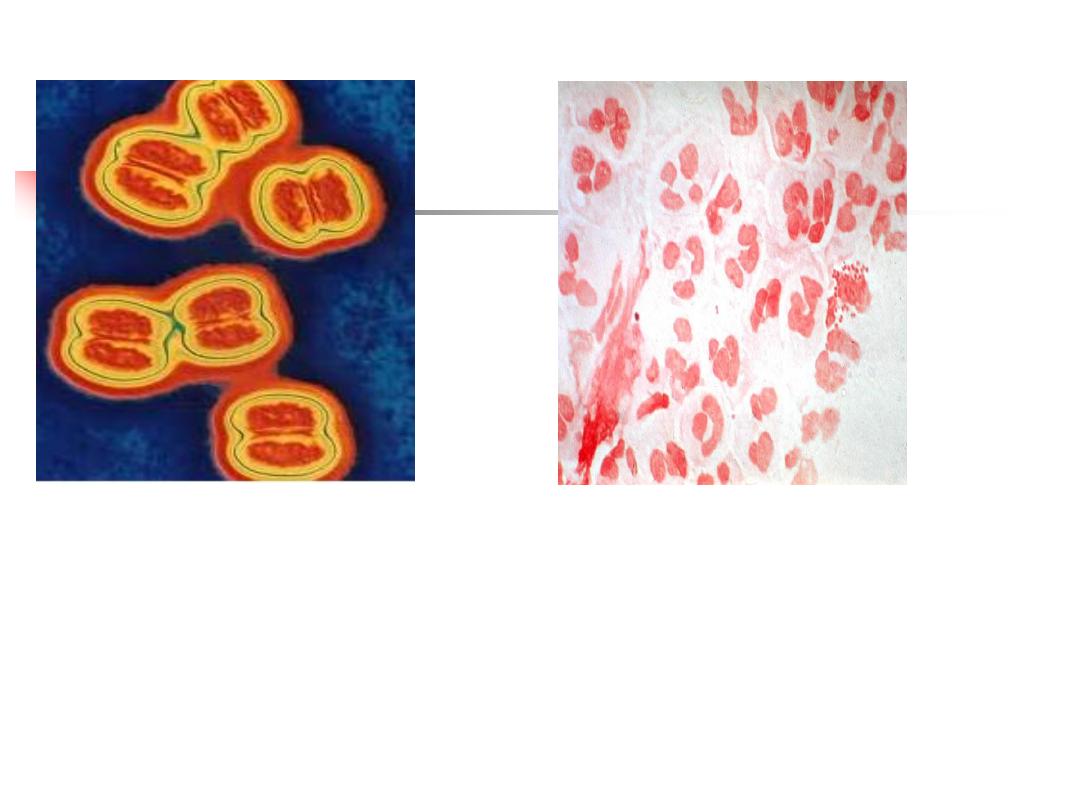
Classical and alternative pathway components
: recurrent
infection with
encapsulated bacteria
particularly
Neisseria
species
Mannose-binding lectin deficiency is
very common
11

12

13
14
Encapsulated Neisseria Species.
15
Investigations:
Blood for complement : C3 and C4 (routinely), CH50
Treatment:
1.
No definitive
2.
Vaccination: with meningococcal, pneumococcal and
H.
influenzae
B vaccines to boost their adaptive immune
responses
3.
Life-long prophylactic penicillin
4.
Screening family members at-risk.
16
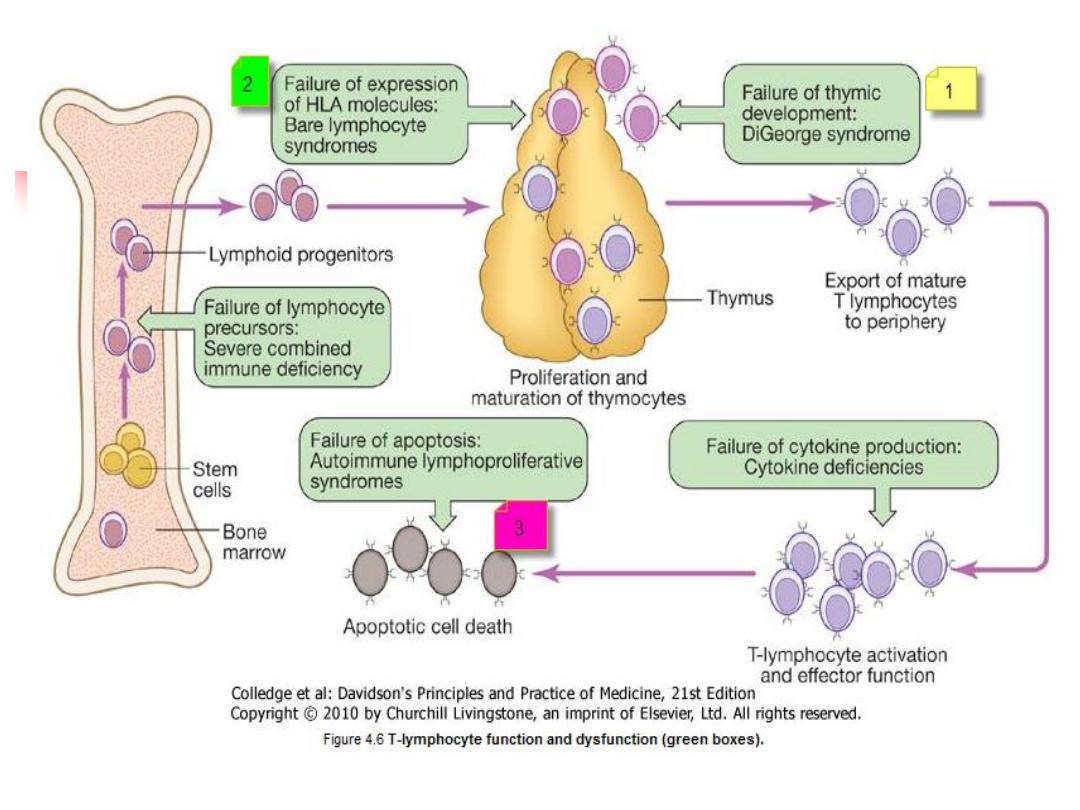
C.1⁰↓Adaptive immune system
Combined ↓ B & T lymphocytes
T lymph ↓ -
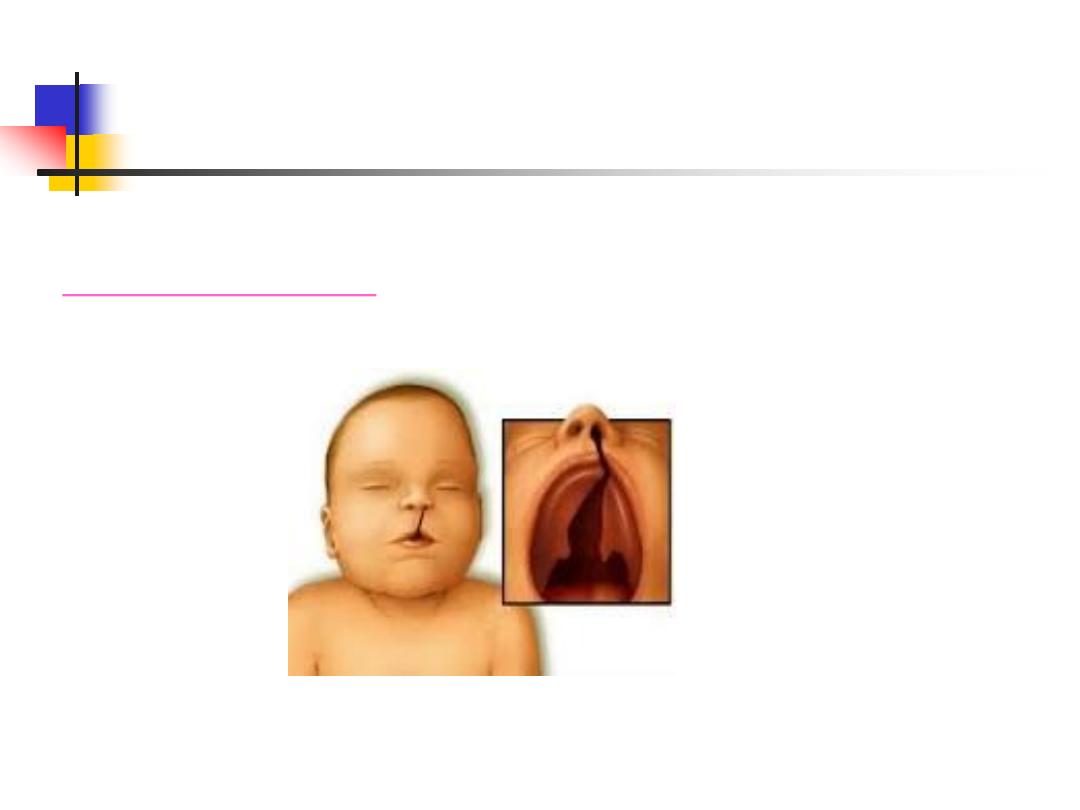
DiGeorge syndrome
- Bare lymphocyte syndromes
-Autoimmune
lymphoprolif. Syndrome
↓ B lymph
- Selective
IgA
-
CVID
- IgG
- overlap
- global
17
Primary T-lymphocyte Deficiencies
Sequelae:
1)DiGeorge syndrome:

18
2)Bare lymphocyte syndromes:

19
3) Autoimmune lymphoproliferative syndrome:
20
21
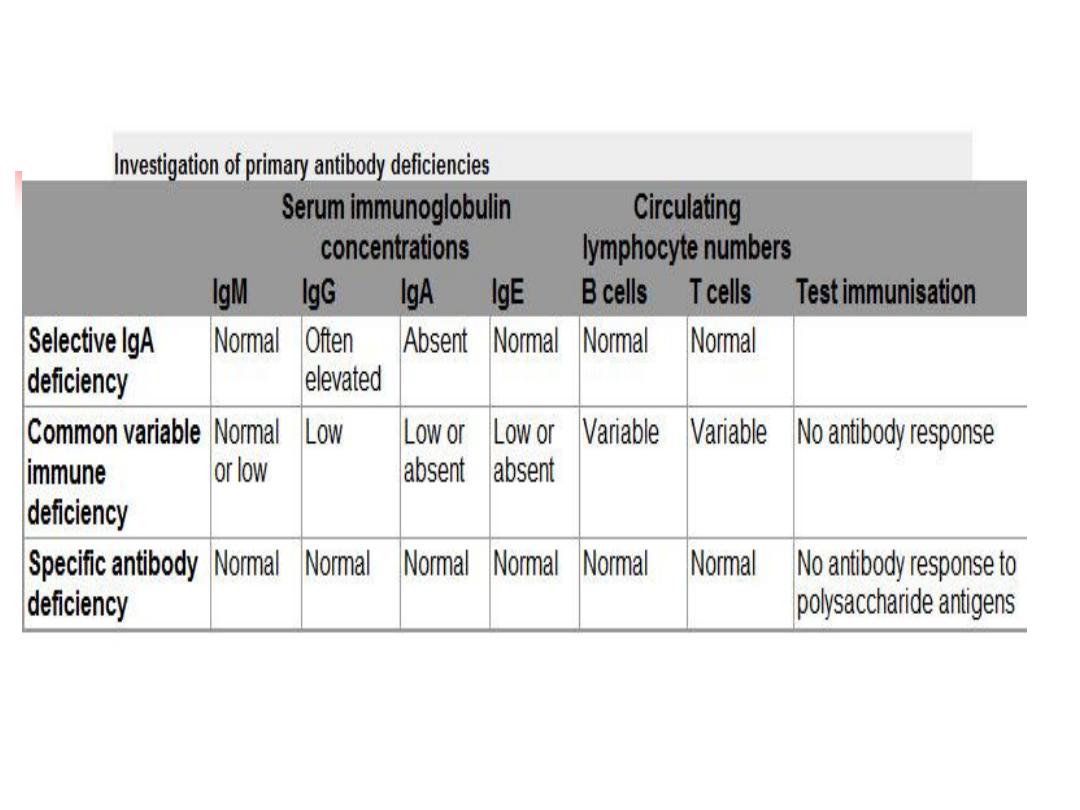
Investigations
Total lymphocyte count
Serum immunoglobulins
Functional tests of T-cell and/or an HIV test
Treatment:
Anti-
Pneumocystis
and antifungal
prophylaxis
Aggressive management of
specific
infections
Immunoglobulin replacement may be indicated if disease is
associated with defective antibody production
Stem cell transplantation ---in bare lymphocyte
syndromes
Thymic transplantation - in DiGeorge syndrome
22
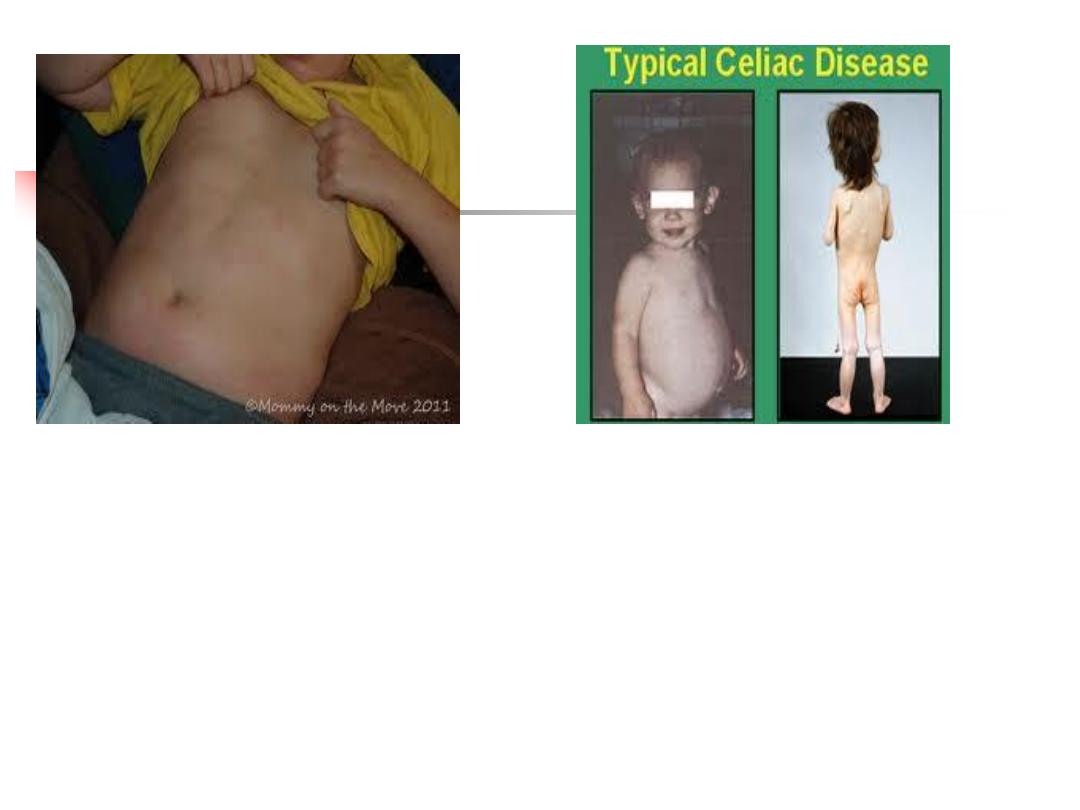
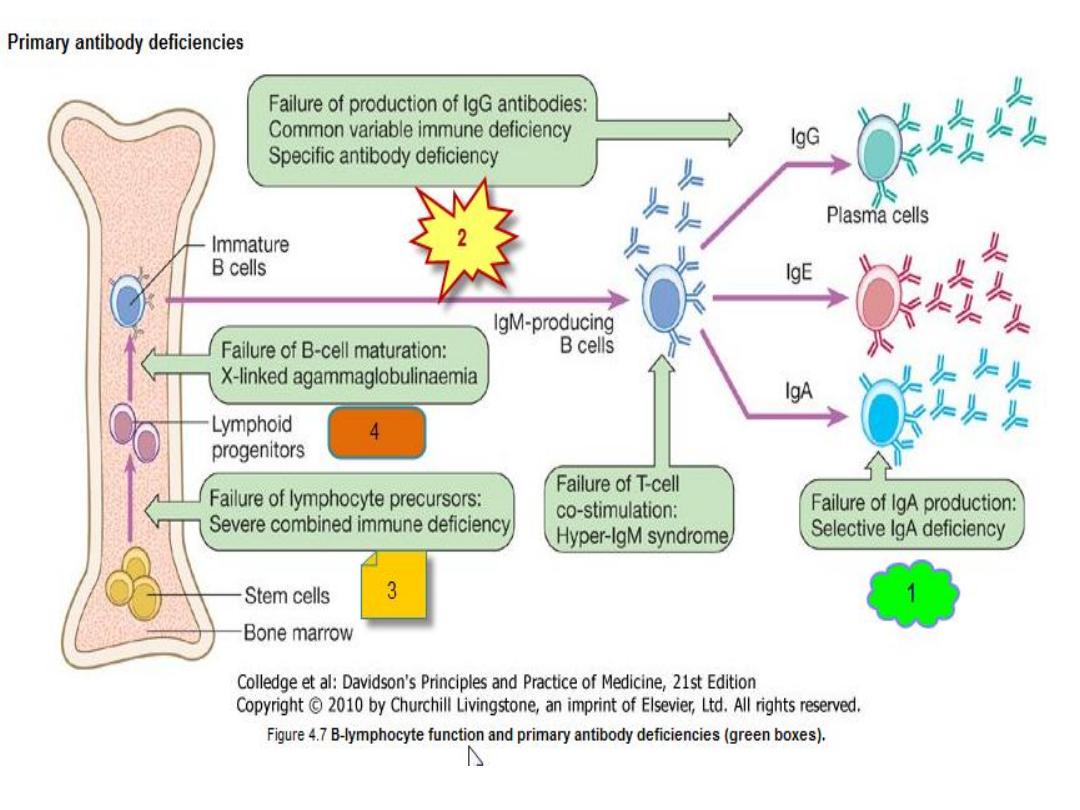
3) Primary B lymphocyte deficiency(Ab ↓):
1)Selective IgA deficiency:
is the
most common
primary immune deficiency
Mostly,
an incidental finding with no clinical
sequelae
30%
of individuals experience recurrent mild
respiratory and gastrointestinal infections
.
23
24
Selective IgA deficiency
25
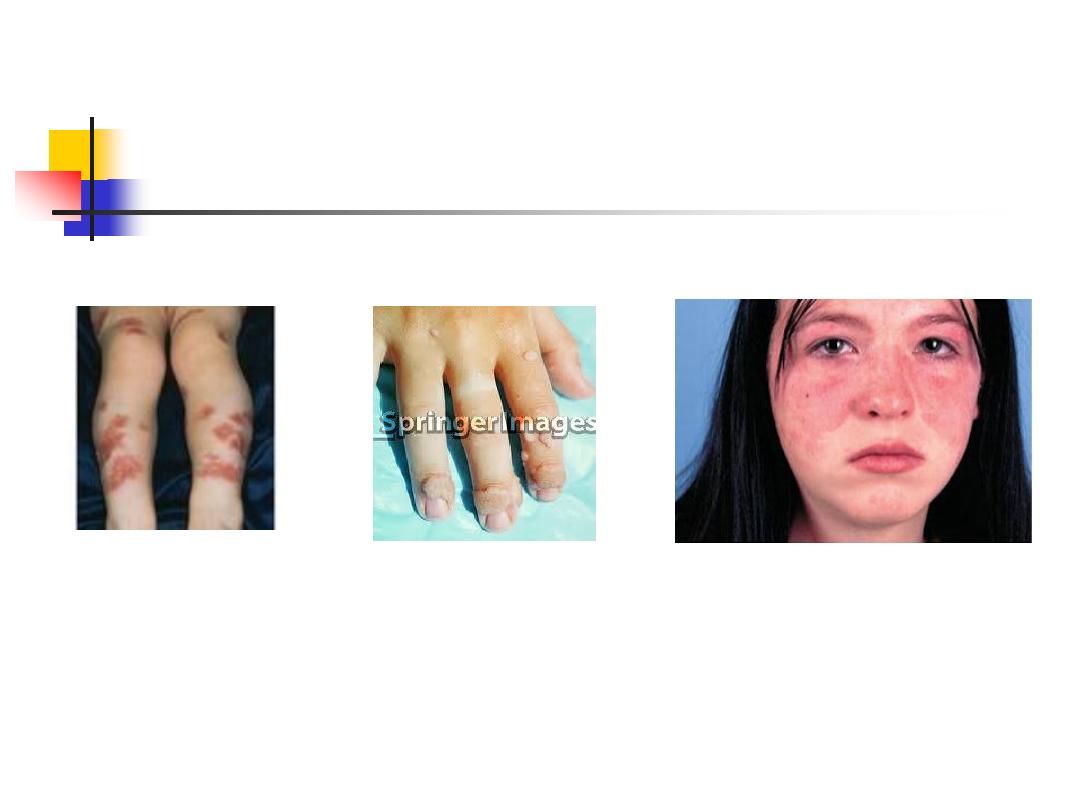
2)Common variable immune deficiency (CVID):
Unknown cause
Characterized by low serum IgG levels and failure to
make antibody responses to exogenous pathogens
Antibody-mediated autoimmune diseases &
increased risk of malignancy.
26
27
3)Specific antibody deficiency or functional IgG
antibody deficiency
4)
There
is
overlap
between specific antibody deficiency
,
IgA deficiency and CVID
,
and some patients may progress to a more
global
antibody deficiency over time
28
29
Investigations:
Serum immunoglobulins & protein and urine electrophoresis
Specific antibody :measuring IgG antibodies against
tetanus,
H. influenzae
and
S. pneumonia
30
Management:
1. Aggressive treatment of infections, and prophylactic
antibiotics
2. The mainstay of treatment is IVIG & life-long
.
3. Immunization is generally not effective (because of the
defect in IgG antibody production) except in selective IgA
deficiency.
4. live vaccines should be avoided
31
32
33
2 ⁰ >> 1⁰ immune deficiencies
Infection is a common cause of secondary immune
deficiency, particularly HIV infection, measles and other viral
illnesses
Immune deficiency is also an expected side-effect of some
drugs (immune suppressive)
May be an idiosyncratic effect of other agents, particularly
anti-epileptic medication
Physiological immune deficiency occurs at the extremes of
life
Summary
ID presented with infection, autoimmune, malignancy.
Causes are 1
⁰ ( phagocyte↓, cmm ↓, Ad ↓), 2 ⁰ ( Phys, inf,
iatrog, malig, biochem--).
Phagocyte ↓---W ↓, CGd, ↓CCR
cmm
↓-angioedema, autoimmune, inf
Ad
↓----- both B & T ↓- inf
T
↓---Digeorge, Bare, & Autoimm Lymph
B
↓-- ↓ IgA, CVD, IgG, Overlap & global
34