Al- Abbasi A.M, PhD, FRCP, DCN, DTM & H
Prof. Of infections Diseases & Clinical Immunology, Coll. Of Med., Univ. of Baghdad, Baghdad, Iraq.CHOLERA

Robert Koch (third from the right) on a cholera research expedition in Egypt in 1884, one year after he identified V. cholerae.
Black and yellow Jack signal flags on ships
IDENTIFICATION
An acute bacterial enteric disease characterized in its sever form by:
Sudden onset, profuse painless
watery stool (rice-water stool),
nausea and profuse vomiting
early in the course of illness.
In untreated cases, rapid dehydration,
acidosis, circulatory collapse,hypoglycemia in children, and renal failure can rapidly
lead to death.

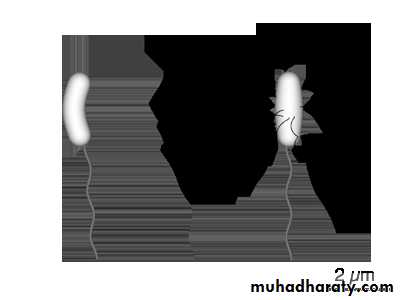
Single flagellum
Dehydration


CASE DEFINITIONWHO, CDC
DISEASE UNKNOWN IN AREA:Severe dehydration or death from acute watery diarrhea in a patient aged 5 or more.
ENDEMIC CHOLERA:
Acute watery diarrhea with or without vomiting in a patient aged 5 or more.EPIDEMIC CHOLERA:
Acute watery diarrhea with or without vomiting in any patient.Vibrio cholerae
Gram-negative, comma-shaped bacterium.V. cholerae is a facultative anaerobic organism and has a flagellum at one cell pole.
During infection, V. cholerae secretescholera toxin, a protein causes profuse, watery
diarrhea.
Two sero groups, O1 and O139, cause outbreaks of cholera.
O1 causes the majority of outbreaks, while O139 – first identified in Bangladesh in 1992 – is confined to South-East Asia.
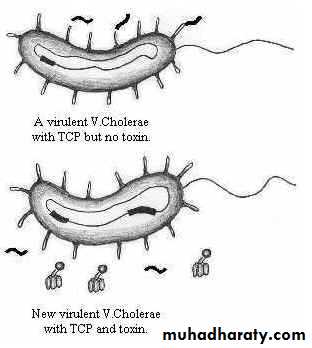
In 1996 Matthew K. Waldor and John J. Mekalanos of the U.S. reported a stunning discovery about the toxin.
The toxin was for the first time shown to be not a part of the bacterium but actually that of a virus (bacteriophage) that got integrated into the V. cholerae genome.
Normally this virus remains silent within V. cholerae but during infection it gets activated.
It then multiplies within the bacterium and escapes to infect other V. cholerae cells.
Under certain laboratory conditions it is possible to activate and release this virus or phage from V. cholerae.
It is called CTX phage, CT standing for cholera toxin.
Along with the toxin, a specific pilus called toxin- corregulated pilus (TCP) is also produced on the surface of V. cholerae.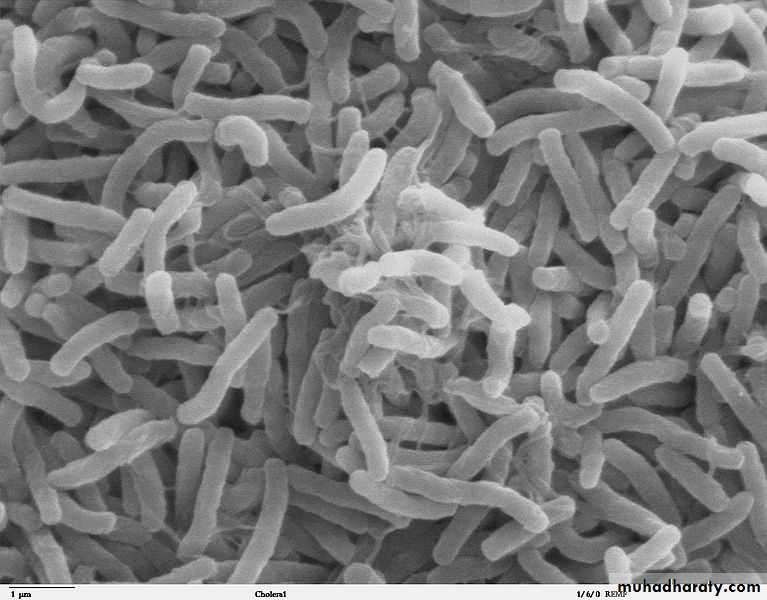
Scanning electron microscope image of Vibrio cholerae

CHOLERA SYNDROM ENZYMATIC DIARRHOEA
Vibrionaceae Family: four generaCholera: 139 strains
01 of Classical type & ELTOR biological type are the causes. Now O139 is blamed to cause the 8th pandemic.
Some other cause of a brief enzymatic diarrhea are:-
NAG, NCV&NVC.
NAG: Short sporadic diarrhea by non O1 vibrios especially V. parahemolyticus group 6.
NCV: Diarrhea by Aeromonas, Plasiomonas genera.
NVC: Other enzymatic diarrhea by non vibrio microorganisms e.g. E.coli.
NB: Vibrios of non O1 group might cause septicemia, wound infection, otitis media..etc.
PATHOGENESIS OF CHOLERA
Local B cellSystemic
B cells
Serum Ab.
Ingestion
Small IntestineEffect of strain
Attachment
Entrotoxin
Production
Attachment for
Life of cell
Antigen
absorption
Vaccination
SECRETION
Gastric acid
Secrtory IgA
T cell dependence
ACcAMP
Nutrition
AgglutinatingVibriocidal
Agglutinating
Copro Ab IgG IgM IgA not opsonizingDestroyed in gut.
Cholera Kinetics water/ Electrolyte Absorption
UPPER G.I. 8 LITERS DAILYPancreas
Saliva
IntestineGastric
Biliary
Intake
Active transport resorption in small GI:-
500-1000 mI only Large intestine
Net secretion of water stool/ day=100mI
ATP
AC
cAMP
AMP
80% Na+ absorbed actively with glucose/ amino acid, only 20%
with CL-.Glucose absorption not affected by cholera toxin.Cholera
Toxin
Irreversible
activation
phosphodiesterase
Electrolyte composition of diarrheal stools, oral and intravenous replacement solutions (mEq/L)for cholera.
• Substance
• Na+
• Cl-
• K+
• HCO
• glucose
• Stool
• 135
• 100
• 15
• 45
• -
• Adult
• Child
• 105• 90
• 25
• 30
• -
• Oral solution*
• 90
• 80
• 20
• 30
• 111
• IV solution †
• 134
• 99
• 13
• 48
• optional
*WHO solution, 3.5 gm NaCl, 2.5 gm NaHCO3, 1.5 gm KCl, glucose 20 gm/L (or sucrose 40 gm/L).
† Dacca solution (5/4/1)= 5 gm NaCl, 4 gm NaHCO3, 1 gm KCl /L.


Diarrhea "rice water" in nature and may have a fishy odor.
An untreated person with cholera may produce 10 to 20 liters (3 to 5 US gal) of diarrhea a day with fatal results.For every symptomatic person, 3 to 100 people get the infection but remain asymptomatic.
Cholera has been nicknamed the "blue death"as victim's skin turns bluish-gray from extreme loss of fluids.


Cholera/ Food poisoning
Intravenous fluids in treatment of vibriosis• I V. Fluid
• Na+
• K+
• HCO3-
• Cl-
• Ca++
• Plasma
• Sod.chloride
• 0.9%
• Hartmans
• Sod.bicarb.
• 1.4%
• Sod.lactate M/6
• 142
• 150
• 131
• 167
• 167
• 4.5
• -
• 5
• -
• -
• 26
• -
• 29
• 167
• 167
• 103
• 150
• 111
• -
• -
• 2.5
• -
• 2
• -
• -

FACTORS FAVORING ERADICATION
V. cholerae is fragile microorganismLarge doses are required for infection 1 billion mo. Vs 1 million for S. typhi & 100 mo for shigellosis
No bactremia
Lack of person-person transmission
Short incubation period
Impact of non-specific control measures
Public motivation
FACTORS IMPEDING ERADICATION
Persistence of V.cholerae in the aquatic environmentIncrease in the population density
Non existence of an adequate vaccine
Limited protection from natural immune system
Failure of other traditional public- health measures e.g. Chemoprophylaxis, quarantine, trade embargoRapid development of microbial resistance and lack of effective treatment
Flexibility & variety of microbial toxigenic strains

THANK YOU

