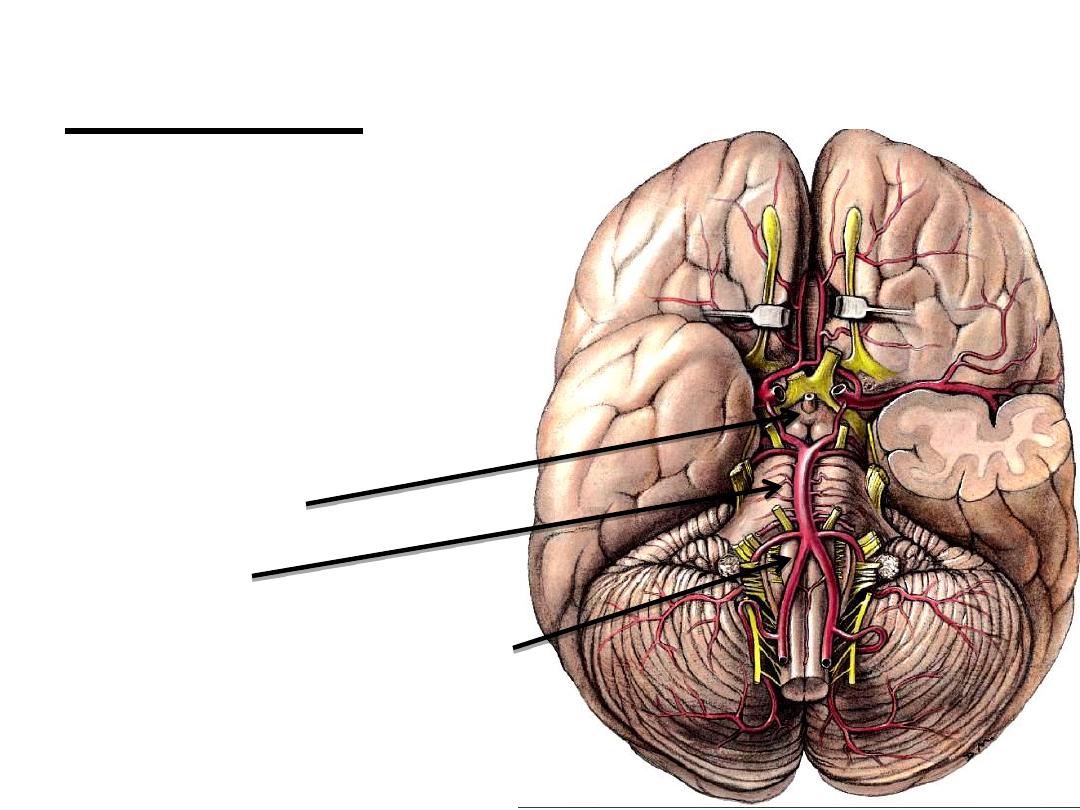
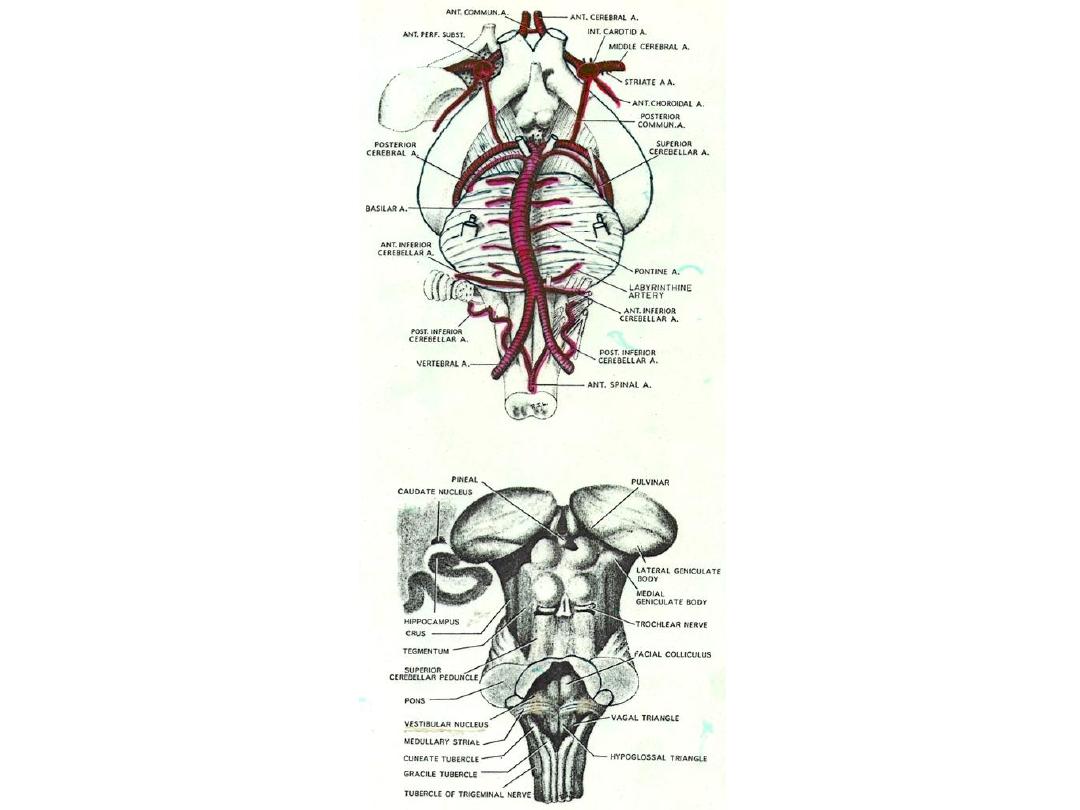
Brain Stem
1. Midbrain
2. Pons
3. Medulla Oblongata
1
Medulla Oblongata
Ext. features
*Direct continuation of Spinal Cord
*Extend from foramen magnum to lower Pons
*More than 2.5 cm in length.
*Lower part is
closed
& resemble spinal cord.
* Upper part is
open
& forms part of the floor of 4
th
.
Ventricle.
2
3
White Matter
*
(Pyramidal Fibers) Cortico-Spinal Fibers
Cortico-Nuclear Fibers
*
Medial
Longitudinal
Fasciculus
*
Spinal tract of Trigeminal Nerve
*
Post. & Ant. Spino-Cerebellar Tracts
*
Spinal Lemniscus (Spino-Thalamic Tracts)
Med. Lemniscus Fibers
*
Internal Arcate Fibers Olivo-Cerebellar Fibers
Reticulo-Cerebellar Fibers
*
Descending Tracts (Extra-Pyramidal)
4
Internal structure
Main Nuclei:
1. Gracile & Cuneate Nuclei
2. Accessory Cuneate Nuclei
3. Olivary Nuclei (main-pricipal)
4. Accessory olivary Nuclei
5. Arcuate Nuclei
6. Lat. Reticular Nuclei
7. Spinal Nucleus & Tract Trigeminal Nerve
8. Hypoglossal nerve Nuclei
9. Cranial Accessory Nerve Nuclei
10. Vagus Nerve Nuclei
11. Glossopharyngeal Nerve Nuclei
12. Solitory Nucleus & Tract
13. Ambiguus Nucleus
14. Inf. Salivatory nucleus
5
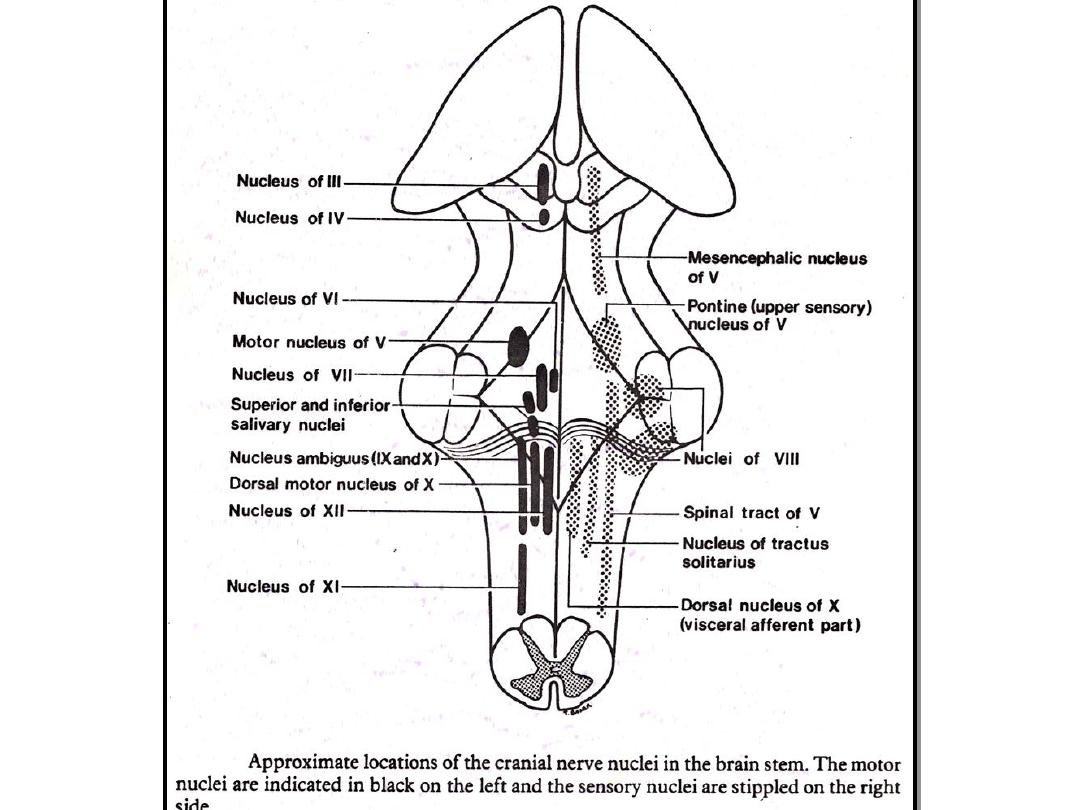
Nuclei of The Medulla Oblongata
A. Medullary-Cerebellar Relay Nuclei
1. Olivary nuclei (Main , Principle)
2. Accessory Olivary nuclei
3. Lat. Reticular nucleus
4. Arcuate nucleus
5. Accessory cuneate nucleus
B. Crainial Nerve Nuclei
1. Spinal Trigeminal nerve nucleus
2. Hypoglossal nerve nucleus
3. Cranial Accessory nerve nucleus
4. Vagus nerve nuclei
5. Glossophryngeal nerve nuclei
C. Other Nuclei
1. Gracilis & Cunate nuclei
6
7
8
Secondary Reflux Fibs of Trigeminal:
To various motor nuclei of cranial nerves (largely uncrossed)
Provide connections for many reflexes due to stimulation of
areas innervated by V
1.
Corneal Reflex (to motor nucl. VII)
2.
Lacrimal // (to sup. Salivatory nucl. Of NI)
3.
Sneezing // (to RF, N.Ambig, Phrenic N., IC muscles nuclei
in spinal cord)
4.
Vomitting Reflex (to DMN of X, N.Ambig, Solitary N.)
Eff. Fibs. Spinal Nucl. V:
1.
Trigemino-thalamic --- (most fibs., cross & join Med. Lemn.)
2.
Trigemino-Reticular --- (some fibs.)
3.
Trigemino-cerebellar --- (Inf cerebellar ped. (crossed &
uncrossed)
4.
Trigeminal (for reflexus) --- (Asc. & Dsc. on same side
connecting with motor nuclei of cranial nerves, eg. Trigemino-
Facial)
Lesions V Nerve
9
Whole Nerve produce:
1- Anesthesia of corresponding Ant. Half of scalp,
face, cornea, conjunctiva, mucous membranes
(nose, mouth, pre-sulcal tongue)
2- Paralysis & atrophy in muscles supplied by V
* Divisions produce:
1- Limited sensory loss & if lingual nerve is affected =
loss of taste in Ant. 2/3 of tongue
10
Hypoglossal nuclei (somatic motor)
Efferent fibers:
To muscles of tongue except Palatoglosses
Afferent fibers :
*
Receive fibers (crossed & uncrossed) & collaterals from
reticular neurons
(some of these fibs. Constitute the terminal part of a cortico-
bulbar system effecting voluntary movements of tongue
*
Receive fibers which are 2ndary Glossopharyngeal, Vagal &
Trigeminal which mediate reflex tongue movements in
response to stimuli from lingual oral, and pharyngeal mucous
membrane (ie. Taste, touch , thermal & pain
Lesions of Hypoglossal Nerve
1- LMN paralysis of ipsilat. ½ of tongue with loss of move ment, tone
& atrophy of muscles affected
PN:
Since genioglossus effects protrusion of tongue to opposite
side, the tongue, when protruded, will deviate to side of injury.
2- The close proximity of the emerging roots of the XII nerve & the
pyramidal tracts forms the basis of the
Inferior (or Hypoglossal) alternating hemiplegia
which results from ventral lessions of this area.
= a. LMN paralysis of ipsilateral ½ of the tongue
b. A contralateral hemiplegia
11
12
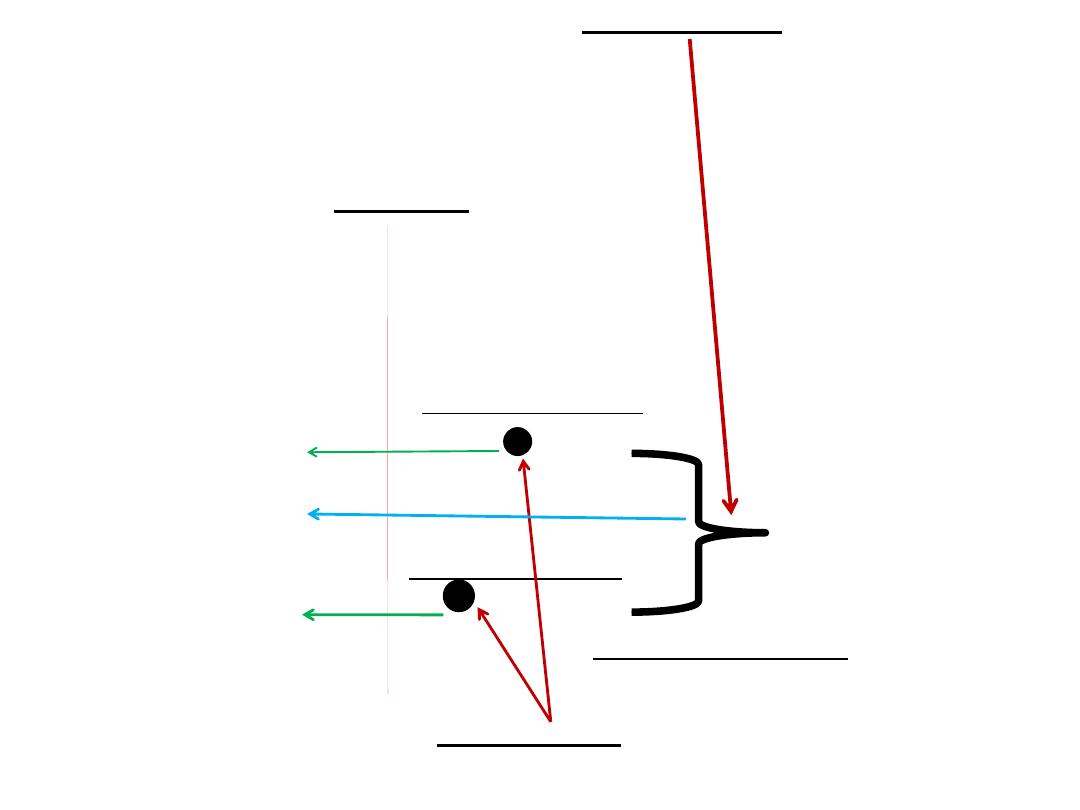
Desc. Fibs from:
1. Cerebral Cortex
(cortico-olivary)
2. Red Nucl. (rubro-olivary)
3. Periaqueductal grey mater
MIDLINE
Dorsal Accessory Olivary Nucl.
Par-olivo-Cerebellar Fibs
Olivo-Cerebellar Fibs.
Med. Accessory Olivary Nucl.
Parolivo-Cerebellar Fibs
Principal Olivary Nucl.
Asc. Fibs from:
Spino-Olivary Tract
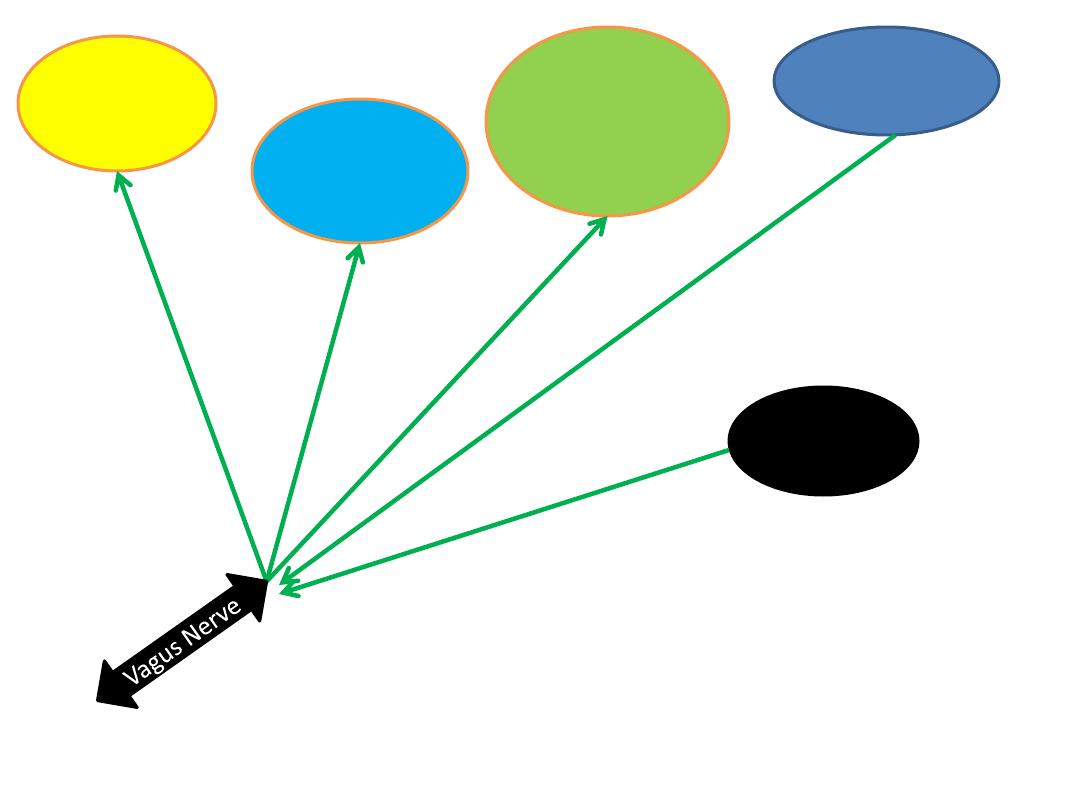
Vagus Nerve Functional components
GSA (general somatic afferents) (cell bodies in
superior
ganglia of vagus ---relay on Spinal Nucl. Trigeminal N.
)
GVA (general visceral afferents) ( cell bodies in
inferior
(Nodose) ganglia of vagus --- relay on dorsal vagal
sensory nucl. (Med.Solitary Nucl.)
)
SVA (special visceral afferents) ( cell bodies in
inferior
(Nodose) ganglia of vagus --- relay on lat. Solitary nucl.
)
GVE (general visceral efferents)
SVE (special visceral efferents) ( cell bodies in
nucl.
Ambiguus
)
Dorsal vagal motor nucl.
---
smooth muscle
Inf. Salivatory nucl.
---- glands
Cell bodies in:
14
Dorsal Vagal
motor nucl.
(GVE)
Lat. Solitary
nucl.
(SVA)
(Gustatory
Nucl.)
Med. Solitary
Nucl.
(GVA)
(Dorsal Vagal
sensory
nucl.)
Nucleus
Ambiguus
(SVE)
Spinal
Nucl.
Trigeminal
(GSA)
Secondary Fibers X Nerve
*
From sensory nuclei X & IX go to various motor nuclei of cranial &
spinal nerves
e.g.:
to hypoglossal & salivatory nuclei for lingual & secretory
reflexus.
*
From pharyngeal, respiratory & alimentary mucus membranes pass
to nucl. Ambiguus and are involved in pharyngeal & laryngeal reflexes
*
Other nerve impulses go to dorsal motor nucl. Of X, Phrenic nucl. &
nuclei of intercostal muscles in spinal cord which are involved in
coughing, vomiting & respiratory reflexes
15
Lesions of X nerve
*
Bilat. Destruction of X (fatal)
1- Paralysis of larynx = Asphyxia أختناق
)
)
2- Paralysis of esophagus & stomach = pain & sever vomiting
3- Loss of vagal reflexes
e.g:
respiratory reflex = Dyspnea صعوبة التنفس
)
)& cardiac
acceleration
*
Unilat. Destruction of X
Produces Ipsilat. Paralysis of :
Soft palate = Hoarseness
بحة
)
) of voice
Pharynx = Dysphagia
(
صعوبة البلع
)
, anesthesia خدر
)
)
Larynx = Dyspnea (therefore ipsilat. Loss of cough &
palatal reflexes)
*
Destruction of visceral motor fibers = ipsilat. Loss of Carotid
Sinus reflexes
16
Glossopharyngeal Nerve Functional components
17
GSA (general somatic afferents) (cell bodies in
superior ganglia of IX --- relay on Spinal Nucl.
Trigeminal N.
)
GVA (general visceral afferents) (cell bodies in
inf. Ganglia (Petrous gang.) of IX--- relay on
dorsal vagal sensory nucl.(Med.Solitary Nucl.)
)
SVA (special visceral afferents) (cell bodies in
inf. Ganglia (Petrous gang.) of IX--- relay on Lat.
Solitary Nucl.
)
GVE (general visceral efferents) (
Inf. Salivatory
Nucl.
)
SVE (special visceral efferents) (
Nucl. Ambiguus
)
Lesions of IX Nerve
Major symptoms include:
1- Loss of pharyngeal (gag) rflex
2- Loss of Carotid Sinus reflex
3- Loss of taste in Post. 1/3
rd
. Of
tongue
18

19
Nucleus ambiguus (SVE)
*
Composed of typical LMN whose axons innervate Larynx & Pharynx
*
Lie ventrally between Hypoglossal & Dorsal vagal nuclei.
*
Fibers from upper end of this nucl. Travel in Glossopharyngeal nerve (to
Stylopharyngeus muscle)
*
Fibers from lower end travel in Vagus & Cranial accessory nerves
*
It supply striated muscles of soft palate, Pharynx & Larynx.
*
Inferiorly it is continues with spinal nucl. of Accessory nerve.
Efferents:
*
To striated muscles of Larynx & pharynx.
Afferents:
*
Terminals from cortico-nuclear tracts (both crossed & uncrossed) for the voluntary
control of swallowing & phonation.
*
Receives impulses from pharyngeal & Laryngeal muscles for tonic control .
*
Receives impulses from 2ndary. X, XI and V which convey impulses from oral,
pharyngeal, & respiratory mucosa that mediate various reflexes (e.g.. Coughing,
vomiting, pharyngeal and laryngeal reflexes)
Lateral Medullary Syndrome (Of Wallenberg)
Symptoms & Signs Damage
1. Dysphagia,Dysarthria Nucl.Ambiguus
2. Ipsilat. Analgesia & Thermoanaesthesia of face Spinal Nucl.&Tract Trigeminal
3.Contralat. Pain & temp. loss of body & neck Spinal lemniscus
4.Ipsilat. Limb & gait ataxia. Inf. Cerebellar peduncle
5.Ipsilat. Horner's syndrome Desc. Sympathetic fibers
6.Vertigo, Nystagmus, Nausea & Vomiting Vestibular Nuclei
(Caused by thrombosis of post. Inf. Cerebellar art.)
20
Medial Medullary Syndrome
Symptoms & Signs Damage
1.Contralateral Hemiparesis Pyramidal Tracts
2. II impairment of position sense. Med. Lemniscus
3.Ipsilateral paralysis of tongue Hypoglossal Nucl.
(with deviation to paralyzed side when protruded)
(Caused by thrombosis of medullary branch of Vertebral art.)
21