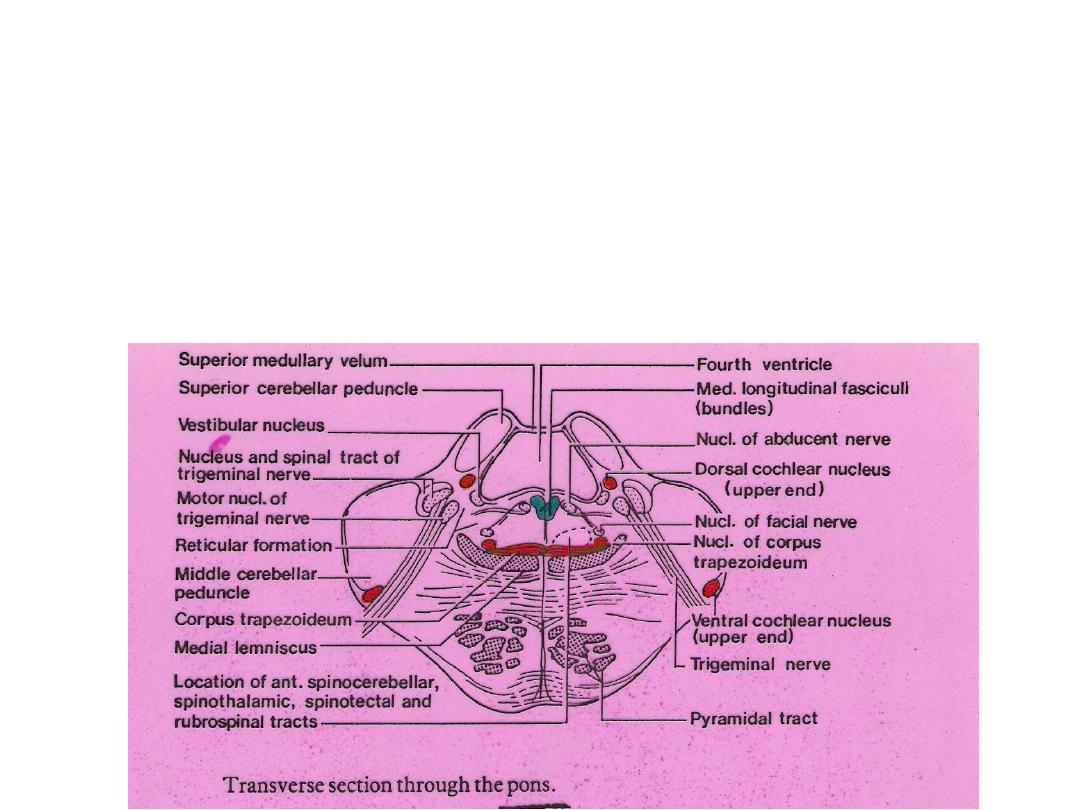
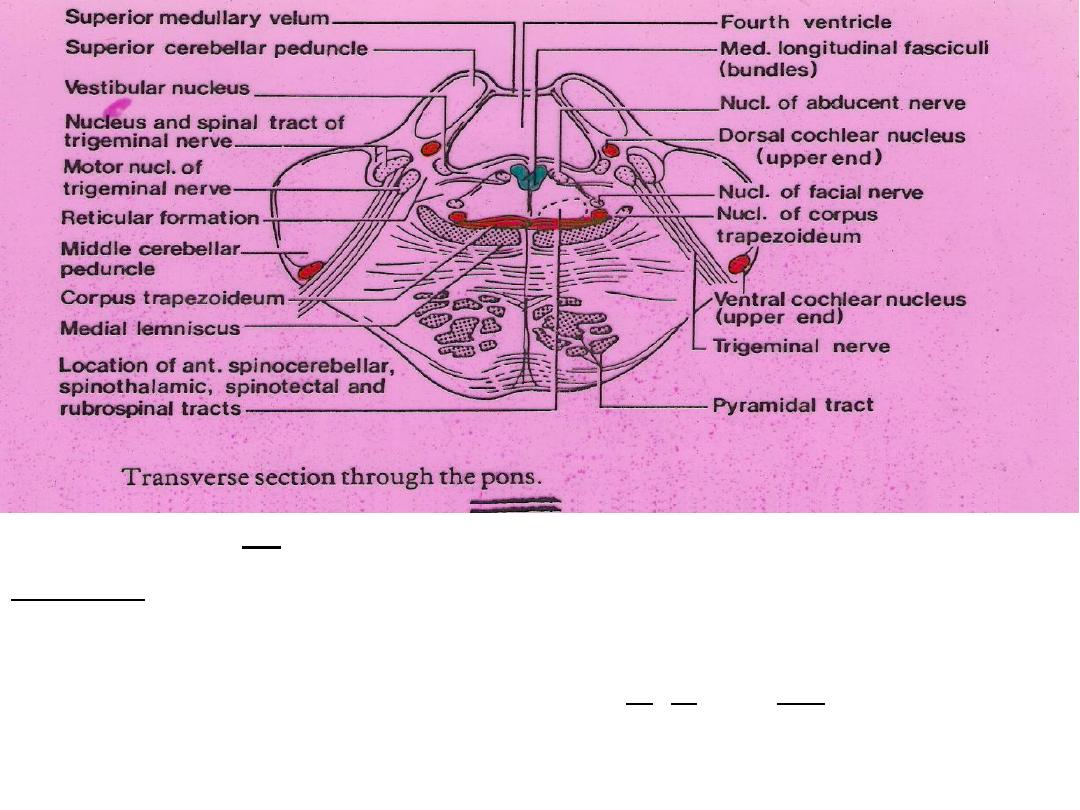
PONS
1

2
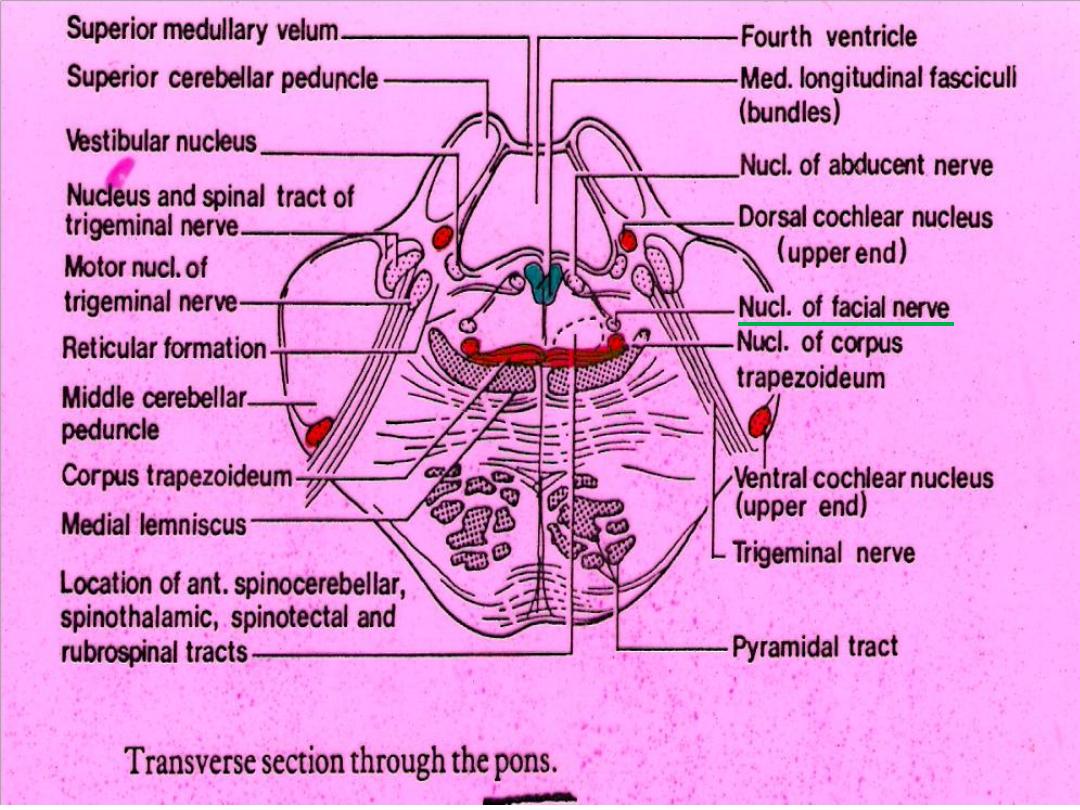
Trigeminal nuclei in Pons
*Lateral part = Principle sensory nucl. V (for touch)
*Medial part = Motor nucl. ( muscles of mastication +
Tensor tempani & Tensor veli palatini)
Central tegmental tract
*Lie dorsal to medial lemniscus
*Large bundle which originate (descending part) from mid-
brain tegmentum (priaqueductal grey & red nucl.)
and terminate in ipsilat. Principle Olivary nucl. and hence to
contralat.1/2 cerebellum.
*Ascending part (large) arises from med. Part of brainstem
reticular formation & project to certain thalamic nuclei.
3
VII Afferents
4
112
Aff. Fibers to facial motor nucleus
1.2ndary. (v) fibs.from spinal
nucleus.
2.Direct cortico-nuclear fibs.
3. Indirect cortico-nuclear fibs.
4. 2ndary. Auditory fibs.
(Acaustico-facial reflexes).
5. From cerebral cortex,
thalamus & globus pallidus
(Emotional facial expresion).
112
Aff. Fibers to facial motor nucleus
1.2ndary. (v) fibs.from spinal
nucleus.
2.Direct cortico-nuclear fibs.
3. Indirect cortico-nuclear fibs.
4. 2ndary. Auditory fibs.
(Acaustico-facial reflexes).
5. From cerebral cortex,
thalamus & globus pallidus
(Emotional facial expresion).
Lesions of Facial nerve
1. Of motor part
(At Stylomastoid foramen) (Bells palsy):
(a). Ipsi-lateral Paralysis of all facial movements.
(b). Ipsi-lateral loss of corneal reflex.
(c) . Ipsi-lateral paralysis of facial emotional movements.
2. Distal to geniculate gang.:
(a).All in lesion(1).
(b).
Ipsi-lateral impaired secretion of sub-mandibular & sub-lingual salivary
glands.
(c).
Ipsi-lateral impaired taste ant. 2/3 tongue (sometimes).
(d).
Ipsi-lateral hyperacusis.( )أحتداد ألسمع
3. Proximal to geniculate gang.:
(a). All in lesions (1 & 2).
(b).
Ipsi-lateral complete loss of taste ant.2/3 tongue.
(c).
Ipsi-lateral impaired lacrimation .
4. Supra-nuclear (central) lesions:
(a). Marked weakness of contra-lateral Muscles in lower 1/2 face.
(b). Emotional innervation may be preserved (largely involuntary).
5
6
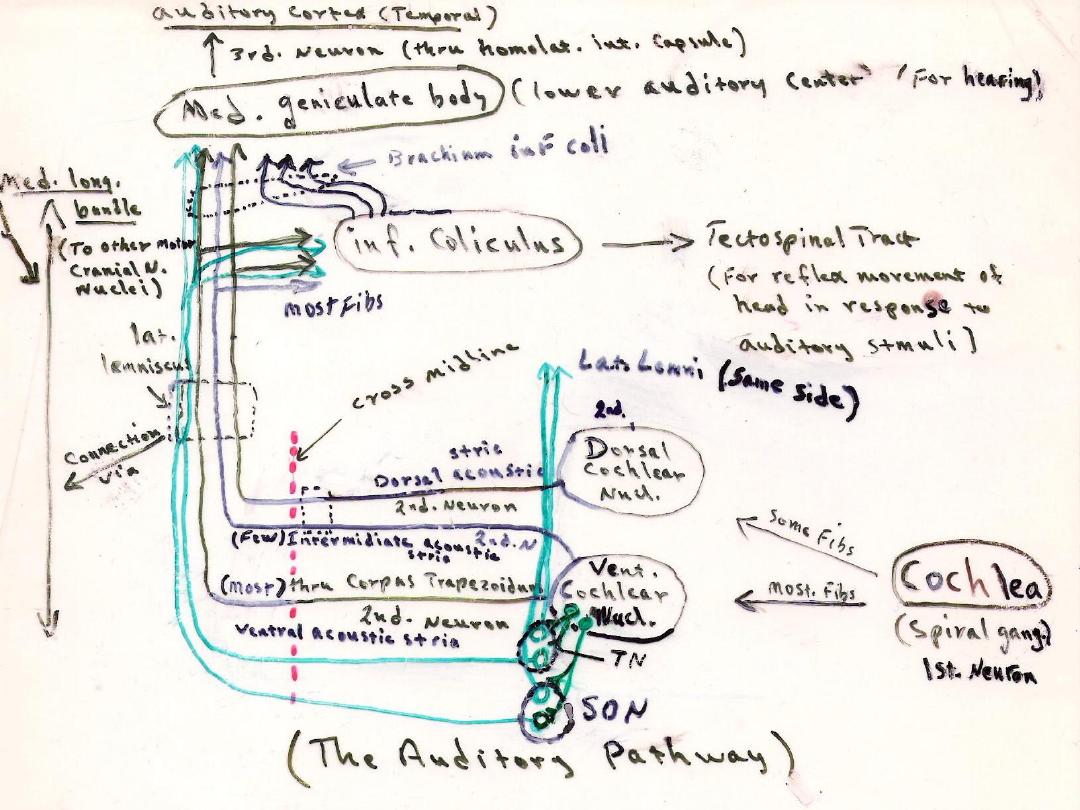
*Destruction of cochlear nerve or both nuclei of that side
produce
complete deafness
on same side.
*Lesion of one lat. Lemniscus or auditory cortex produce
Bilat. Diminution of hearing (
partial deafness
) that is more
marked in contralat. ear (2ndary cochlear pathways are both
crossed & uncrossed).
7
8
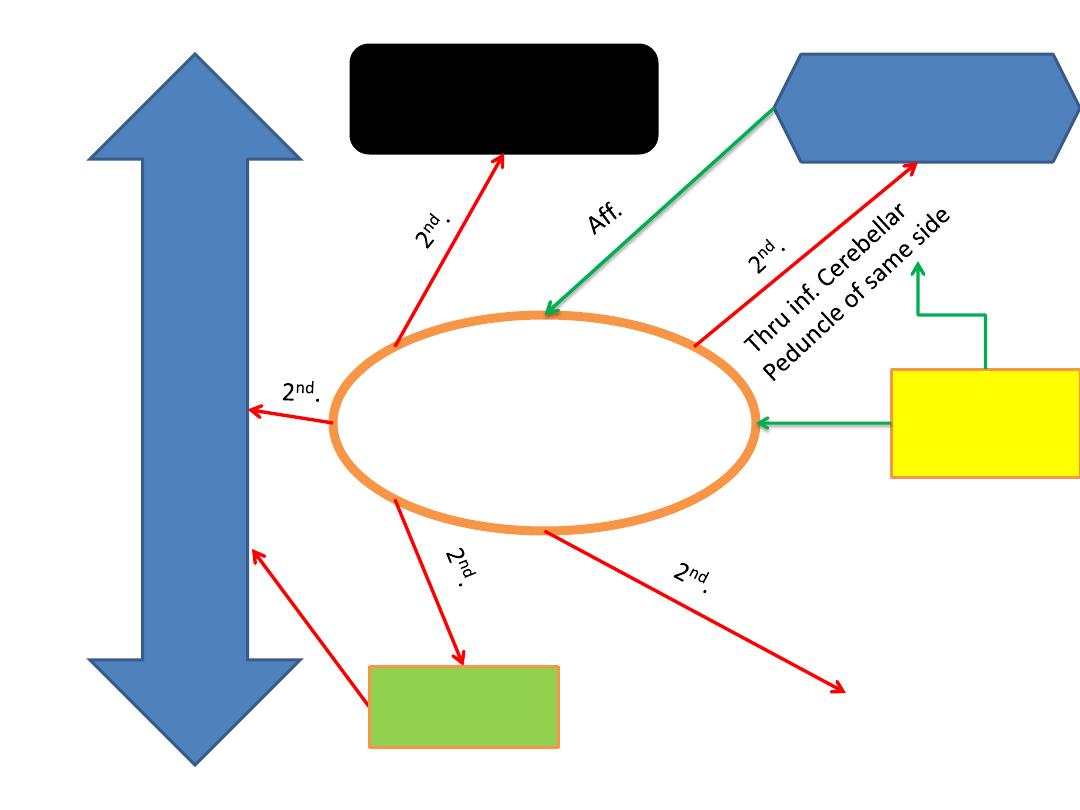
Vestibular Nucleus
Labyrinth
(Vestibular
Ganglia)
Cerebellum
(Fastigial nucl.---
Archaecerebellum)
Med.
Long.
Bundle
of both
sides
Midbrain
Medulla oblongata
Cerebral cortex
(Temporal lobe---post.
parts
1
st
. neuron
1
st
.
Linking
Vestibular
nucl. With
motor
ocular
nuclei
of cranial
nerves
& cervical
ant. Horn
cells
Lat. Leminiscus
Vestiblo-spinal Tract
To ant. Horn cells of same side

9
Medial Longitudinal Bundle
•Lies in mid- line, dorsal to Tecto-spinal tract.
• Extend’s through- out the brain stem.
Linking the Vestibular nucl. with:
1. Interstitial Nucleus.(of Cajal) in lat. Wall of 3
rd
. Ventricle.
2. Oculomotor Nucleus.
3. Trochlear Nucleus.
4. Abducent Nucleus.
5. Nucleus of Lateral Lemniscus
6. Spinal Accessory Nucleus.
For conjugate
متوافق
/
موحد
)
) eye movements
10
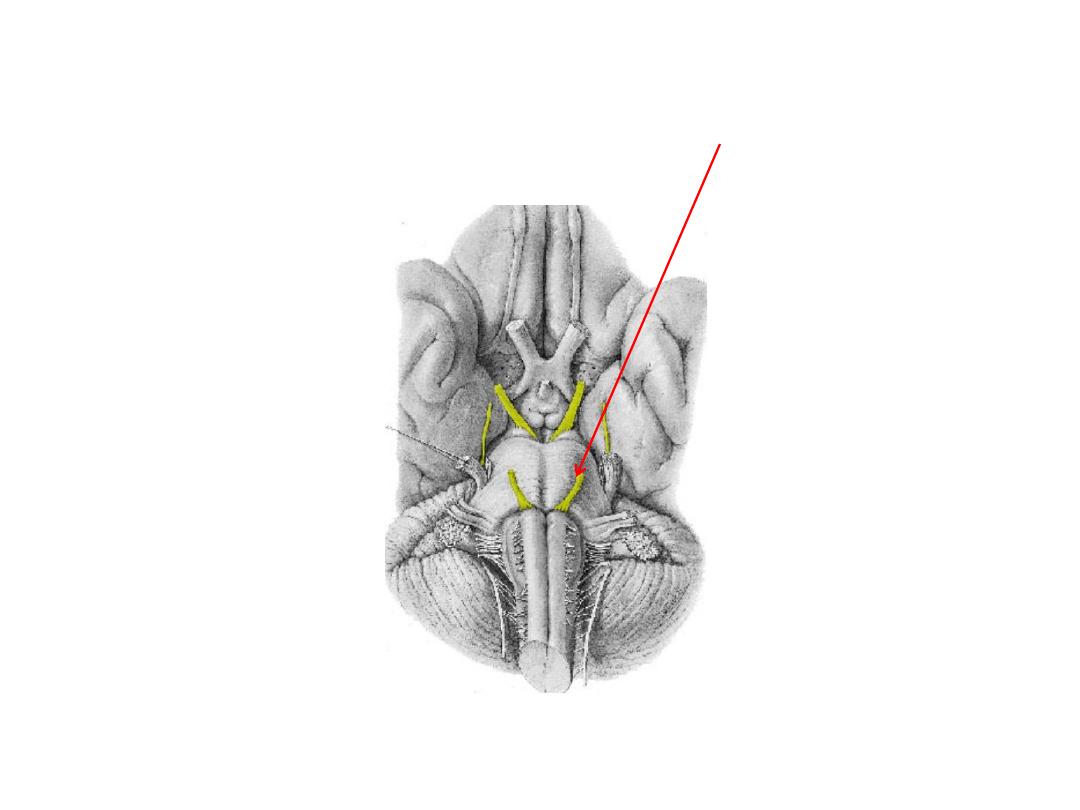
Abducent nerve
113
11
Connections of VI nucleus:
Afferents
1. Cortico-nuclear (mainly from contra-lat. Side).
2. Med. Long. Bundle (with nuclei of III, IV, and VIII).
3. Tecto-bulbar (connected to visual cortex & other centers
thru. Sup. Colliculus).
Lesions of Abducent nerve
(GSE) to Lat. Rectus Muscle
(Which rotates the eye laterally)
A. In brain stem or intra-cranial course produce:
Ipsilat. paralysis of lat. Rectus muscle which results in:
1. Adducted eye due to unopposed action of med. Rectus
(Med. or Convergent Squint). Contralat. eye is normal.
2. Diplopia on attempting to gaze to side of lesion. (Images are
seen side by side---horizontal diplopia)
B. Discreat unilat. Lesion of nucleus (LMN) produce:
Weakness or paralysis of ipsilat. Lateral gaze toward side of
lesion.
C. Lesions involving VI nerve roots & cortico-spinal tracts
produce:
Middle Alternating Hemiplegia (paralysis of ipsilat. Lat.
Rectus & contralat. Cortico-spinal tracts)
12
13
Lesions of III (Oculomotor Nerve)
1- Ext. strabismus (squint
َلِوَح
)
2- Inablity to move eye vertically or inward
3- Dropping of eyelid (Ptosis
ٍّلَدَت
جفن
العين
)
4- Dilatation of pupil (Mydriasis
تمدد
الحدقة
)
5- Loss of pupillary light reflex &
convergence بُراقَت
6- Loss of Accommodation فُّيَكَت reflex.
14
15
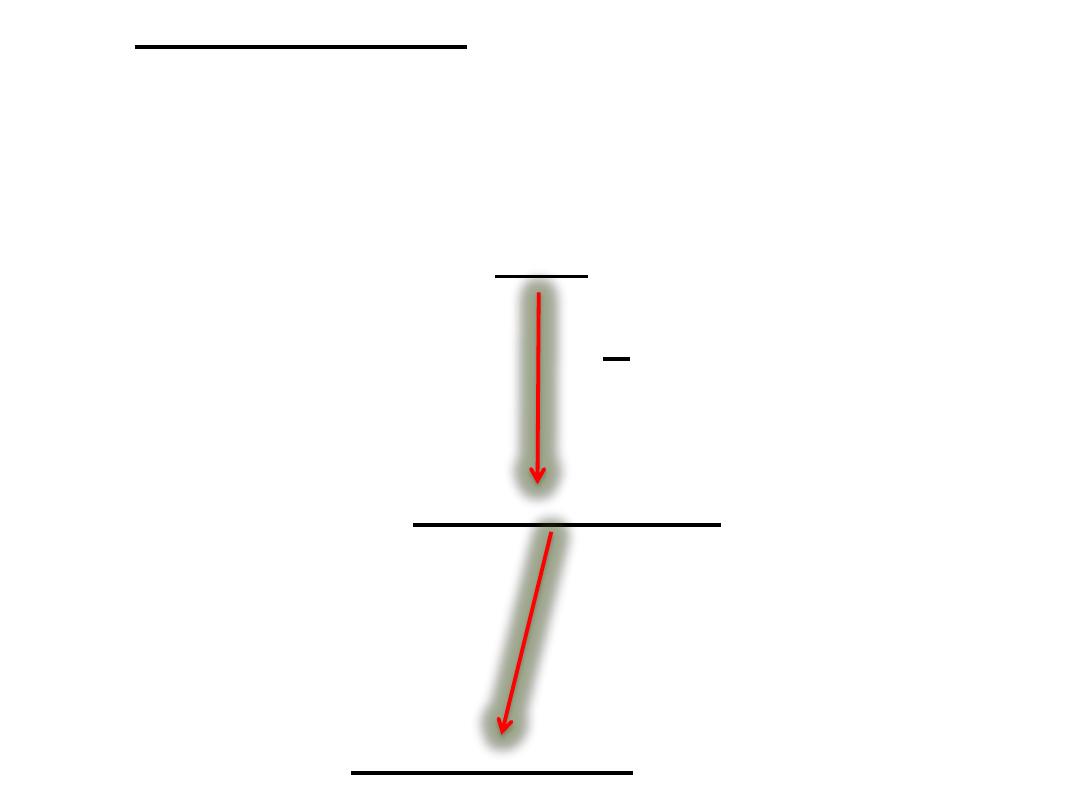
1. Corneal Reflex:
*Touch to cornea or conjunctiva produce
blinking of eye.
AFF.
(From Cornea)
Thru. V N.
Spinal nucleus V
2
nd
. Fibs. To
VII motor nucl.
(Of both sides thru. MLB)
16
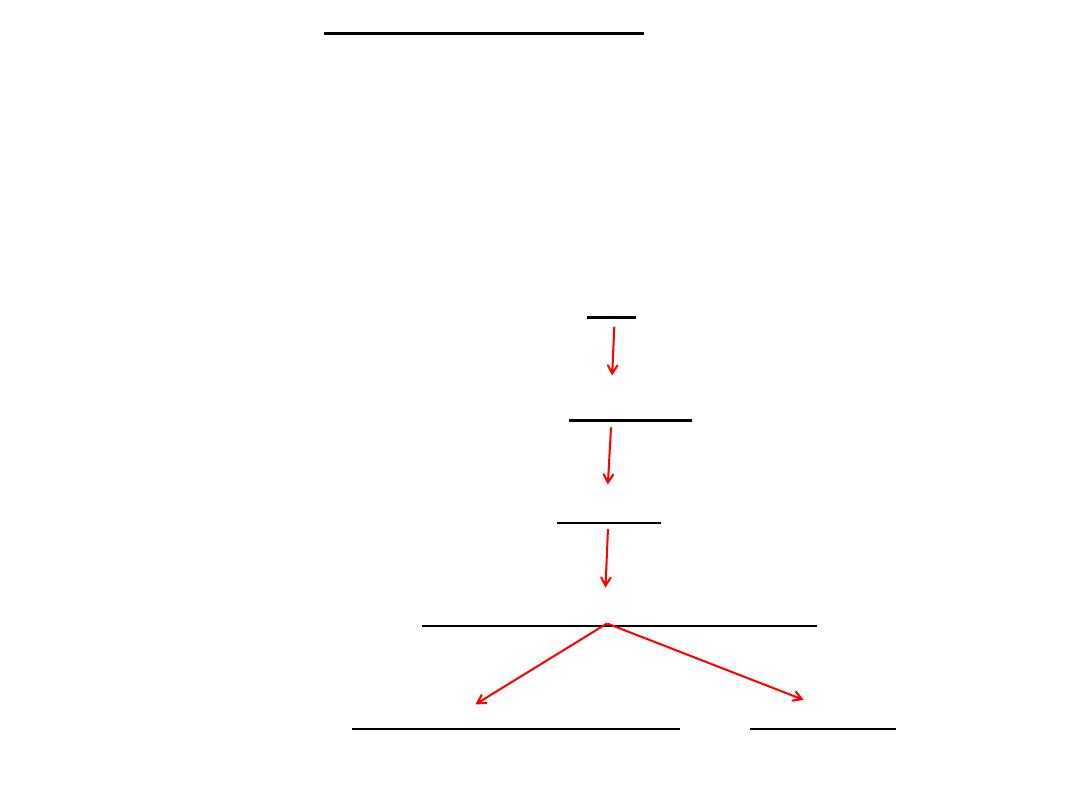
2. Visual Body Reflexes:
*Automatic scanning movements of eyes & head
when reading!
*Automatic movements of eyes, head & neck toward
source of visual stimulus!
*Protective raising of arms & closing of eyes!
AFF. (From Optic nerve)
Optic Tract
Sup. Colli
Tecto-Spinal & Tecto- Bulbar Tracts
1. Ant. Horn cells of Spinal Cord 2. Motor nuclei
. of cranial nerves
17
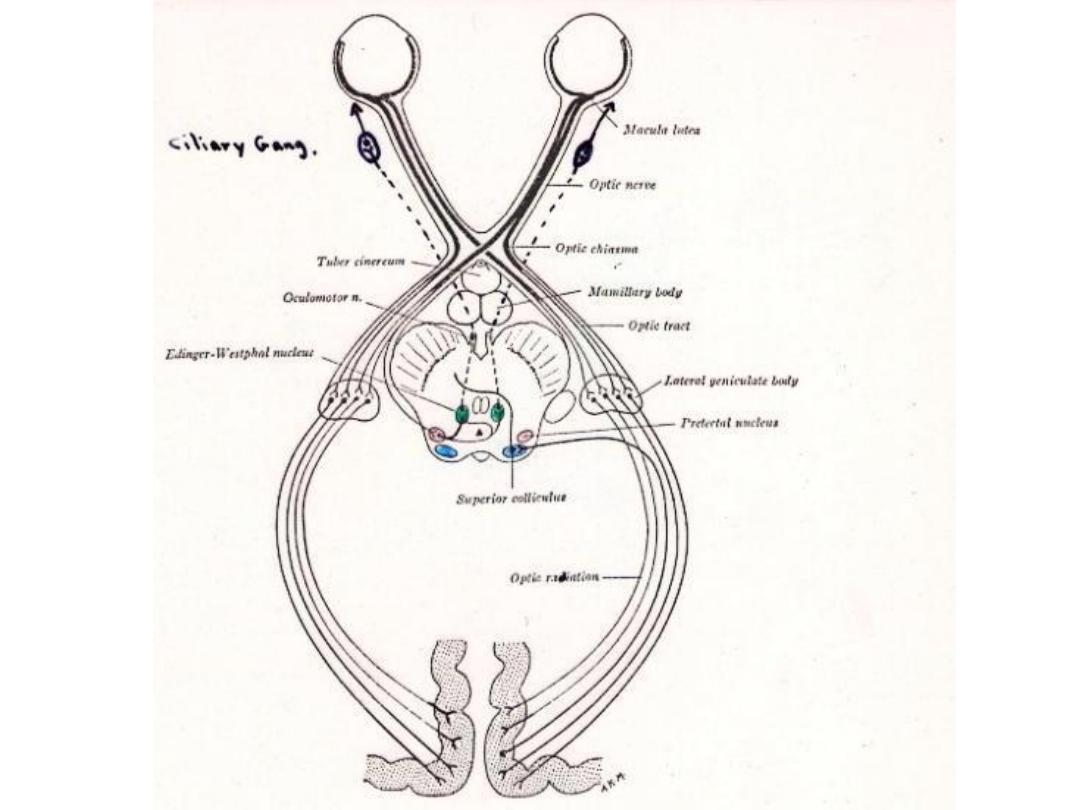
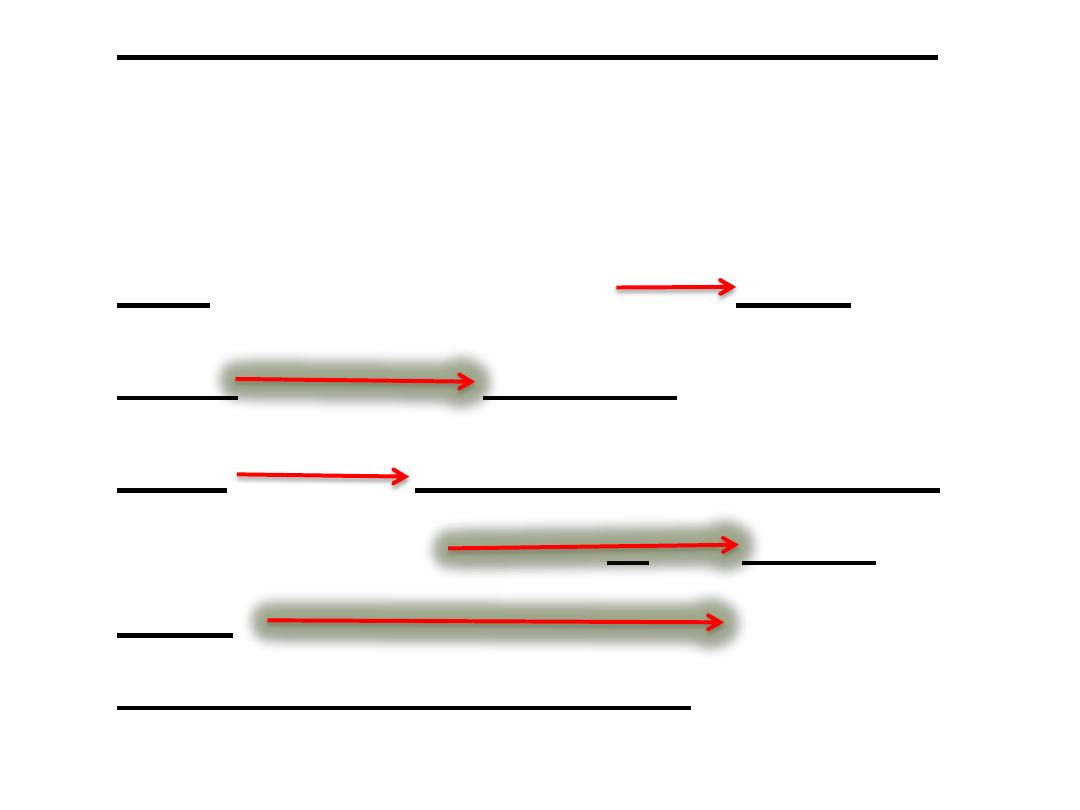
3. Direct & Consensual Light Reflex:
*Light shown into one eye produce pupil
constriction in both eyes.
AFF. (thru. Optic Nerve) Optic
Tract (few fibs.) Pretectal
Nucl. Edinger-Westphal nuclei
(of bothe sides) thru. III N. Cillary
gang. Short Ciliary nerves constrict
Sphincter Pupillae muscles of Iris (both
sides).
18
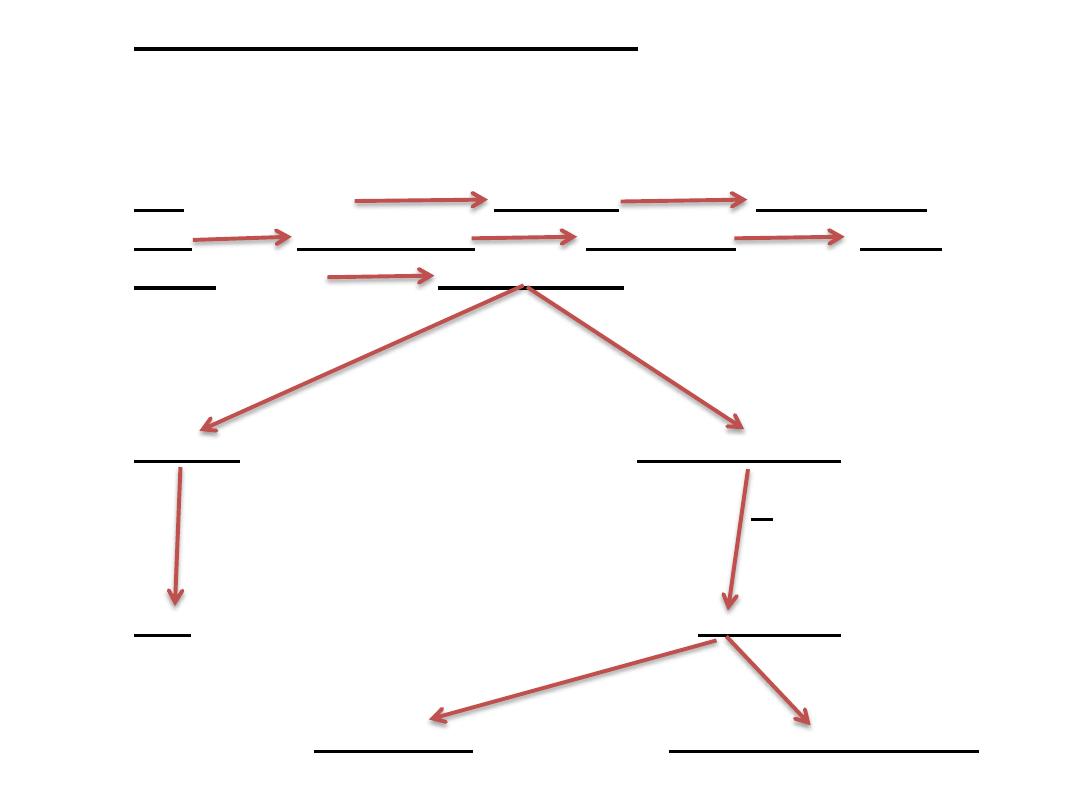
4.Accommodation Reflex:
*Eyes directed from far to near object (Med.Recti contract = convergence
of ocular axis).
AFF. (Optic Nerve) Optic Tract Lat. Geniculate
Body Optic Radiation Visual Cortex Frontal
Cortex (eye field) Internal Capsule
III Nuclei Edinger-Westphal (both sides)
Thru. III Nerve
Recti (contract) Ciliary Gang.
Thru. Short Ciliary Nerve
Ciliary Muscle (contract) Constricter Pupillae muscle
Substantia Nigra
(Main Connections)
Afferent fibers:
1.Strionigral (most)
2.Tegmentonigral
3.Corticonigral
4.Subthalamonigral
5.Rubronigral
Efferent fibers:
1.Nigrostriatal (most)
2.Nigrothalamic
3.Nigrotectal
4.Nigrotegmental
5.Nigrocortical
19
20
Red Nucleus
(main connections)
Afferents:
1.Cerebral Cortex (Corticorubral Tract) precental gyrus
2.Diencephalon (Globus Pallidus, Subthalamic Nucl.,
Nucl. Ventalis Laterals of thalamus)
3.Superior Colliculus.
4.Cerebelum (Dentate, Globosus, Emboliformis nuclei)
Efferents:
1.Rubrospinal
2.Rubrobulbar (thru. Reticular formation to some cranial nerves)
3.Rubrocerebellar
4.Rubrothalamic (VL nucl.)
5.Rubro-olivary
21
Superior Colliculus
(main connections)
Afferents:
1.Retina
2.Visual Cortex
3.Lat. Geniculate Body
4.Inf. Colliculus
5.Spinotectal tract
Efferents:
1.Retina
2.Tectospinal Tract
3.Tectoreticular
4.Tectobulbar
5.Tectotegmental
22
Inferior Colliculus
(main connections)
Afferents:
1.Cocchlea (thru. Lat lemniscus)
2.Inf. Colliculus opposite side
3.Med. Geniculate body
4.Auditory cortex
Efferents:
1.Med. Geniculate body
2.Inf. Colliculus opposite side
3.Sup.colliculus
4.Reticular formation
5.Auditory nuclei (Trapezoid body, Lat. Lemniscus)
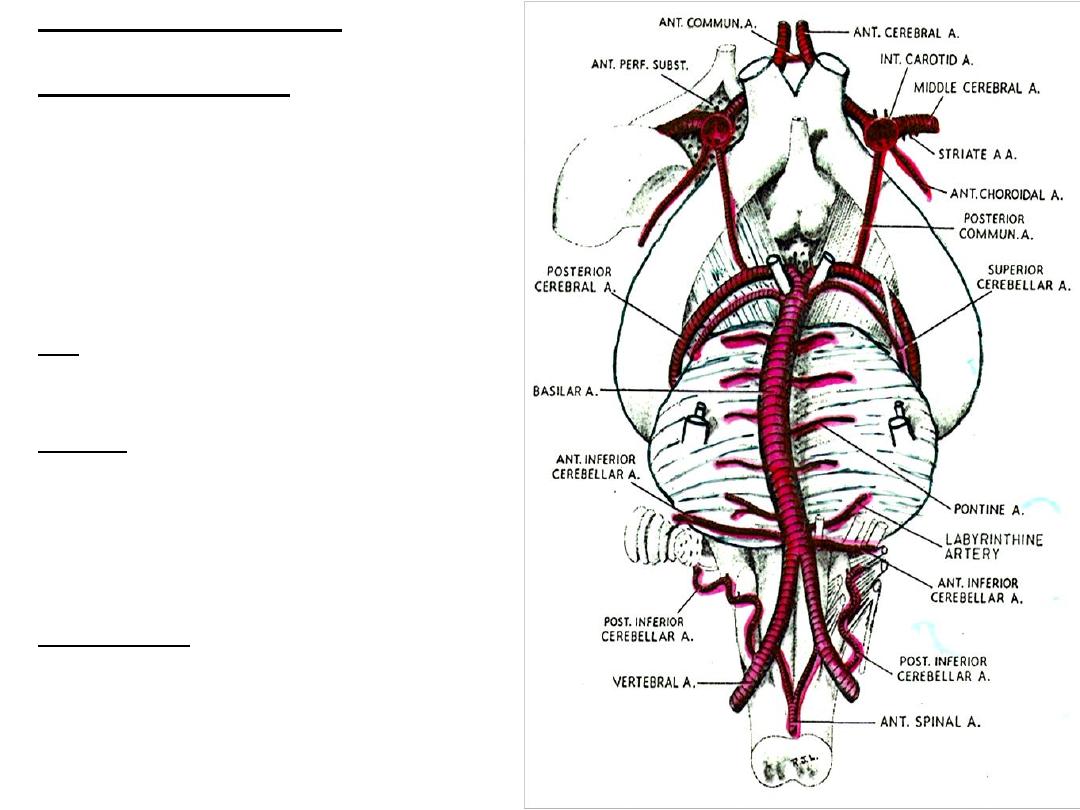
Blood Supply of Brain Stem
A. Medulla Oblongata:
Ventrally: 1.Basilar Art.
2.Vertebral Art.
Lat. & Dorsally: 1.Post. Inf. Cerebellar Art.
Venous Drainage:
Ventrally: 1.Basilar venous plexus
2. Inf. Petrosal Sinus
Dorsally: 1.Occiptal Sinus
P.N.: Medullary veins communicate with
spinal veins.
B. Pons:
Pontine branches of Basilar Art.
Venous Drainage:
1. Basilar venous plexus
2. Inf. Petrosal Sinus
C. Mid- brain:
Post. Cerebral Art.
Venous Drainage:
1. Basal Vein
2. Great Cerebral Vein
23
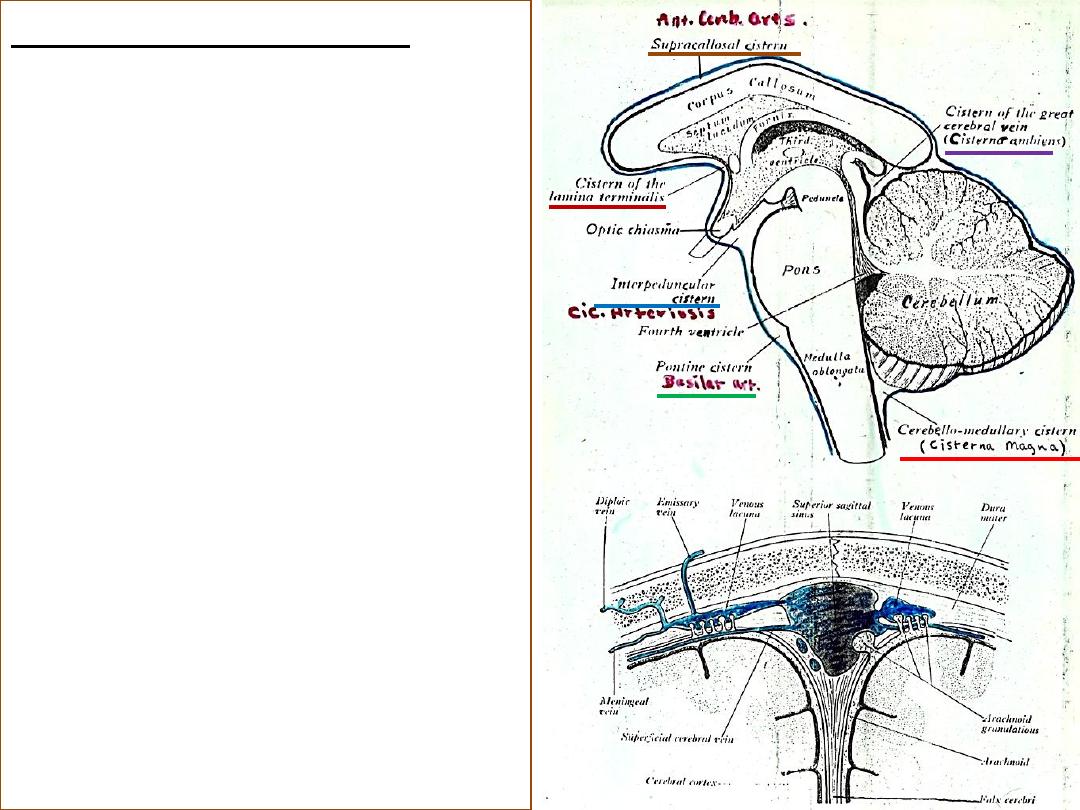
Sub-Arachnoid cisterns
1. Cerebello-Medullary
Cistern
2. Pontin Cistern
3. Inter-Peduncular Cistern
4. Cistern of the Lamina
Terminals
5. Supra-Callosal Cistern
6. Cistern of the Great
Cerebral Vein
24
25
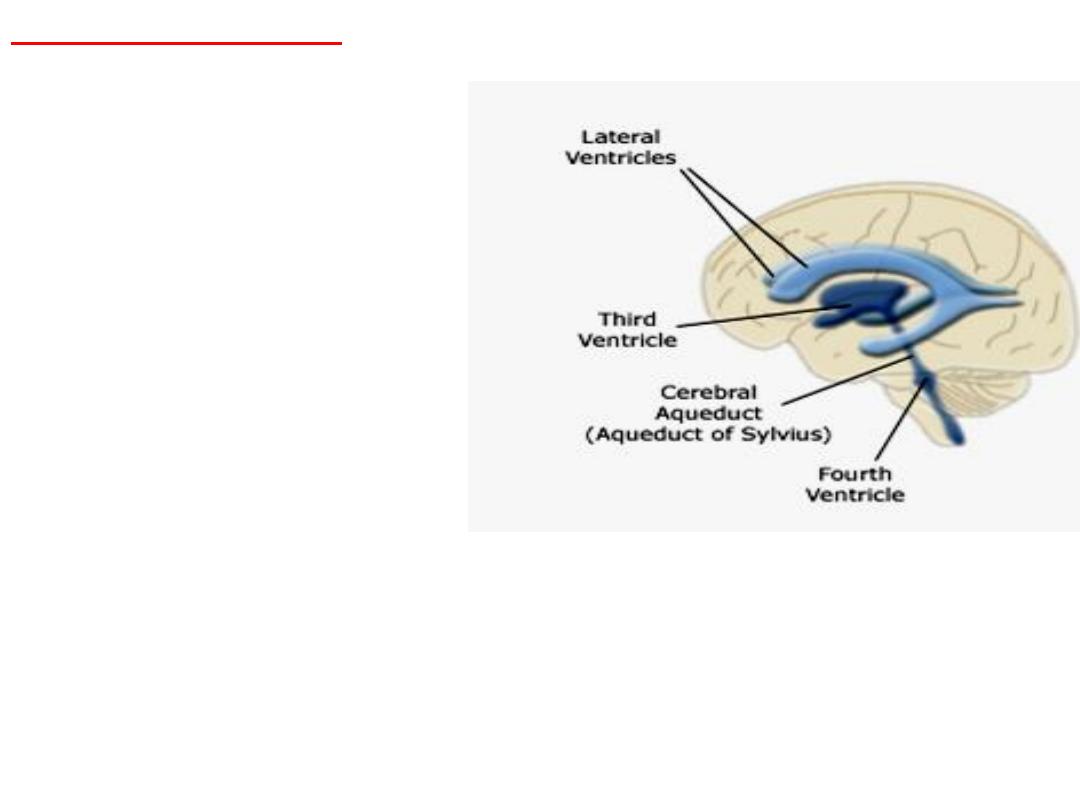
VENTRICLES OF BRAIN
•They are cavities within the brain
•Irregularly shaped
•Lined with ependymal cells
•Four in number
•
Lateral ventricle
(each hemisphere)
•
Third ventricle
(in diencephalon)
•
Cerebral aqueduct
(in midbrain)
•
Fourth ventricle
(lies between pons,
upper part of medulla
and cerebellum, continuous with
central canal of spinal cord)
26
Cerebro-Spinal Fluid (CSF)
*
Ultrafiltrate of blood plasma (except for differences in protein concentration ;
plasma=6500 mg./100g, CSF= 25mg./100g
*
70% secreted by Choroid plexus
*
30% secreted by capillary bed of brain & metabolic H2O production
*
Absorbed by Arachnoid villi into the venous blood (passively / one way valve)
*
Total volume = 140 ml. ( 23 ml. in ventricles)
*
Net production = 400 ml. / day.
*
Clear, colorless, Sp.g. = 1007, contains small amount of protein, glucose,
Potassium & large amounts of Na cl.
*
No substances, no cells.
Functions:
1.Support & cushion CNS ( brain Wt. = 1500g. in air = 50g. in CSF )
2.Reduce momentum & acceleration, therefore, reduce concussive damage.
3.Removes waste products.
4.Integrate brain & peripheral endocrine functions
5.Influences the microenviroment of neurons
6.Normal CSF pressure (measured at
lumbar cistern
)
Recumbent = 100-150 mm. H2O
Sitting = 200-300 mm. H2O
27
Hydrocephalus
Hydrocephalus = Excessive amount of CSF in ventricles of
brain, leading to an
increase
in CSF pressure
Causes:
1-
Inc. production
of CSF
2-
Obstruction
of CSF = Internal Hydrocephalus (
most
cases
) (e.g. stenosis of the cerebral aqueduct, obstruction
of the inter-ventricular foraminae - foramen of Monro).
This can be secondary to tumors, hemorrhages, infections
or congenital malfomations.
3-
Inadequate absorption
= External hydrocephalus
(Communicating hydrocephalus) eg. Blockage of
arachnoid granulation due to infection
28
FOURTH VENTRICLE
Roof (Posterior wall)
Tent shaped cavity & covered by cerebellum
Upper part:
Lies over pons. The Ependyma (Columnar epithelium with stereocilia) is covered with a thin
lamina of white matter called the
Superior Medullary Velum
(bounded by Sup. Cerebellar Ped.)
Lower part:
Lies over medulla. The ependema is covered , in its upper part, by the
Inf. Medullary Velum
, but
in its lower part, by Ependema & Pia matter alone. The lower margin of roof is attached to margins of Gracile
& Cuneate tubercles and is perforated by a midline
Median Aperture
(Foramen of Magendie). Through which
CSF escapes into the cisterna Cerebellomedullaris.
* The cavity extends laterally (
lat. Recess
) in relation to Inf. Cerebellar Ped. Here the roof is attached to
margins of
Medullary Stria
. Each lat. Recess opens into the Cisterna Pontis through the
Lateral Aperture
(Foramen of Luschka).
Choroid Plexus of 4
th
. Ventricle:
T-shped highly vascular tufts of pia matter which invagenates the medullary part of the roof. Starts at each
lat. Aperture by a branch of Post. Inf. Cerebellar Art., to meet in the midline and the two turn down towards
the Median Aperture
Floor:
Diamond Shaped (Rhomboid Fossa)
Bounded sup. By the sup. Cerebellar ped.. Inf. By the gracile & cuneate tubercles and inf. Cerebellar ped.
Has a deep midline groove (median Sulcus)
Widest part of floor is crossed by the Medullary Stria. At its lat.angle lies the
Vestibular eminence
.
The
facial Colliculus
lies in the midline of the pontine part of the floor.
The
inf. Fovea
divide the medullary floor into two triangles (the med. Is the
Hypoglossal
& the lateral is the
Vagal
triangles)
* In addtion to all the cranial nerve nuclei mentioned,
Vital Centers
connected with cardiovascular,
respiratory & metabolic functions, besides many important tracts, are located in this region.
Cerebellum
Functions of Cerebellum:
1.Coordination of somatic motor activity.
2.Regulation of muscle tone.
3.Participationn in the mechanisms that influence & maintain
equilibrium.
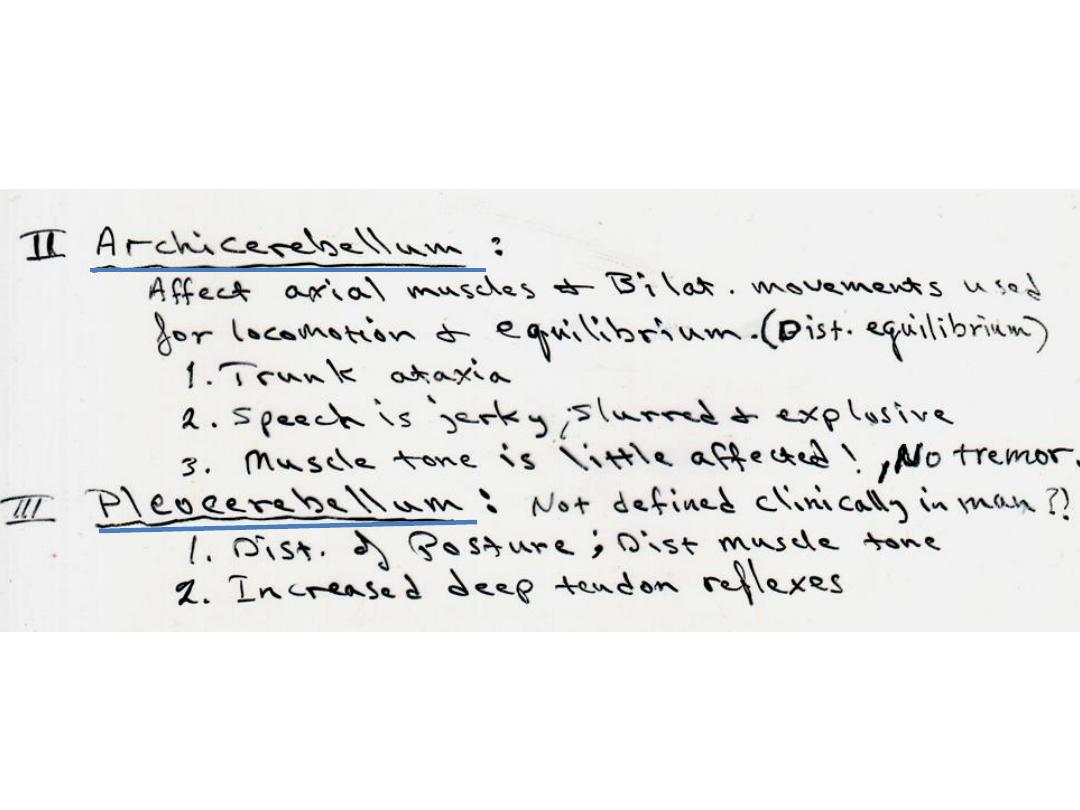
*Three
distinct morphological parts which have evolved
sequentially
1. Archicerebellum (Vestibulocerebellum)
(concerned with
equilibrium)
2. Paleocerebellum (Spinocerebellum)
(concerned with
postural and righting reflexes)
3. Neocerebellum (Pontocerebellum)
(concerned with
coordination of skilled voluntary movements)
29
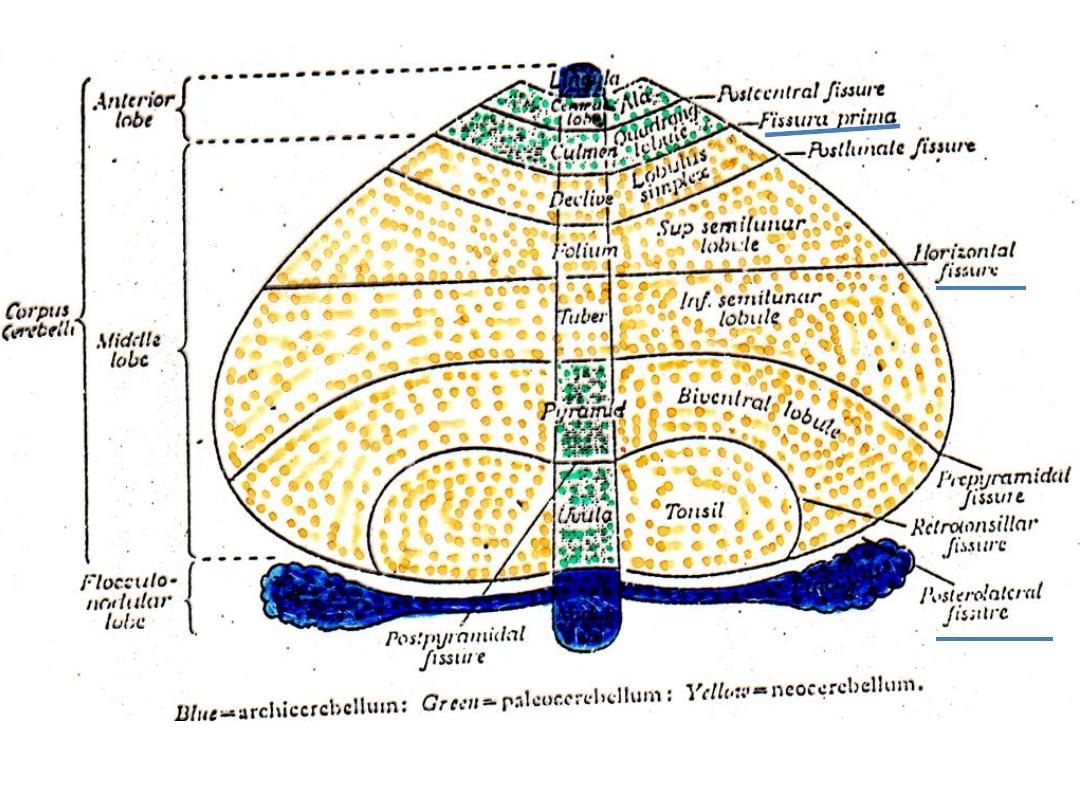
External shape and parts
Two
hemispheres
united in the midline by the
Vermis
(The Vermis is concerned with Axial functions such as speech,
maintenance of upright posture of trunk, standing, and walking )
Three lobes
1.Small
anterior lobe
(lie in front of fissure prima)
2. large
middle lobe
(behind fissure prima)
3. Small
posterior lobe
(Flocculonodular lobule)
Main fissures
• Horizontal fissure (no known functional significance)
• Primary fissure (separates ant. Lobe from middle lobe ie.
Paleocerebellum from neocerebellum)
• Posterolateral fissure (separates post. Lobe from remainder of
cerebellum )
30
31
32
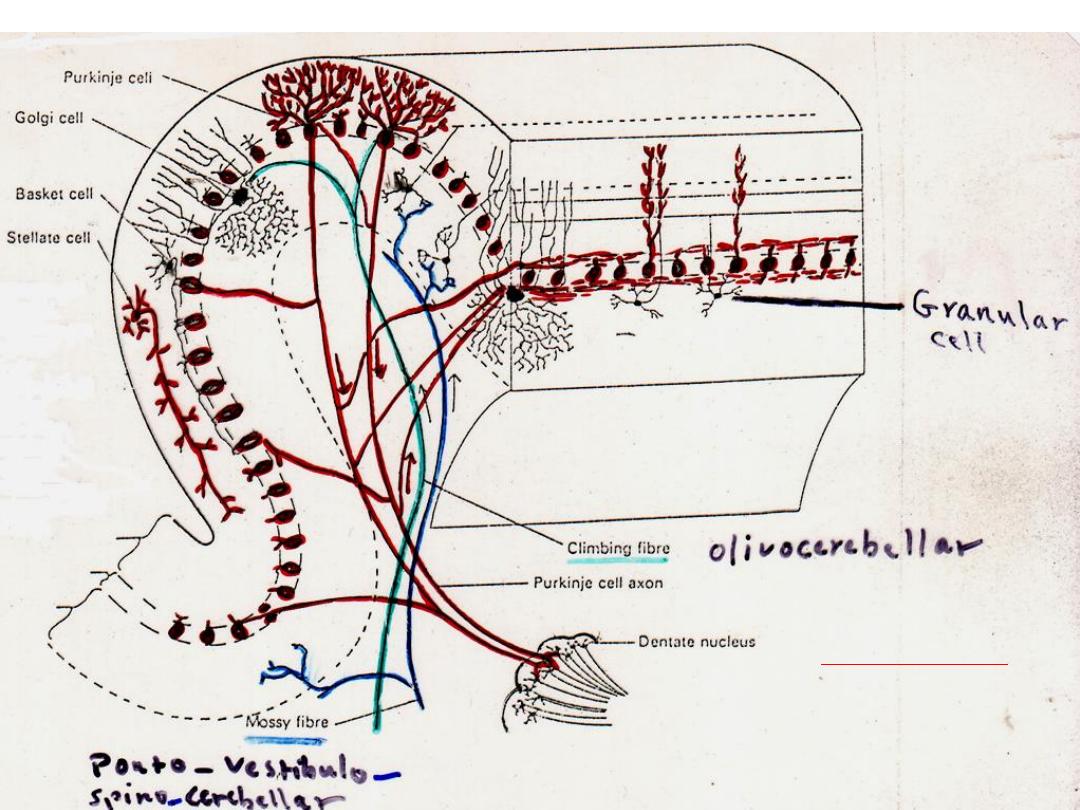
Cerebellar cortex
3 layers:
1.Molecular
2.Purkinje
3.Granular
Cerebellar cortical mechanism
Incoming(Aff.)fibers are of only 2 kinds (Mossy
& Climbing) & both activate Purkinje cells
Single Climbing Fib. Single Mossy Fib
(+) (+)
excite One purkinje cell excite thousand of purkinje cells
via granular cells
(Inhibitory)
Purkinje axon
Inf. olivary complex (-)
(+)
(excitatory)
Deep cerebellar nuclei
(+)
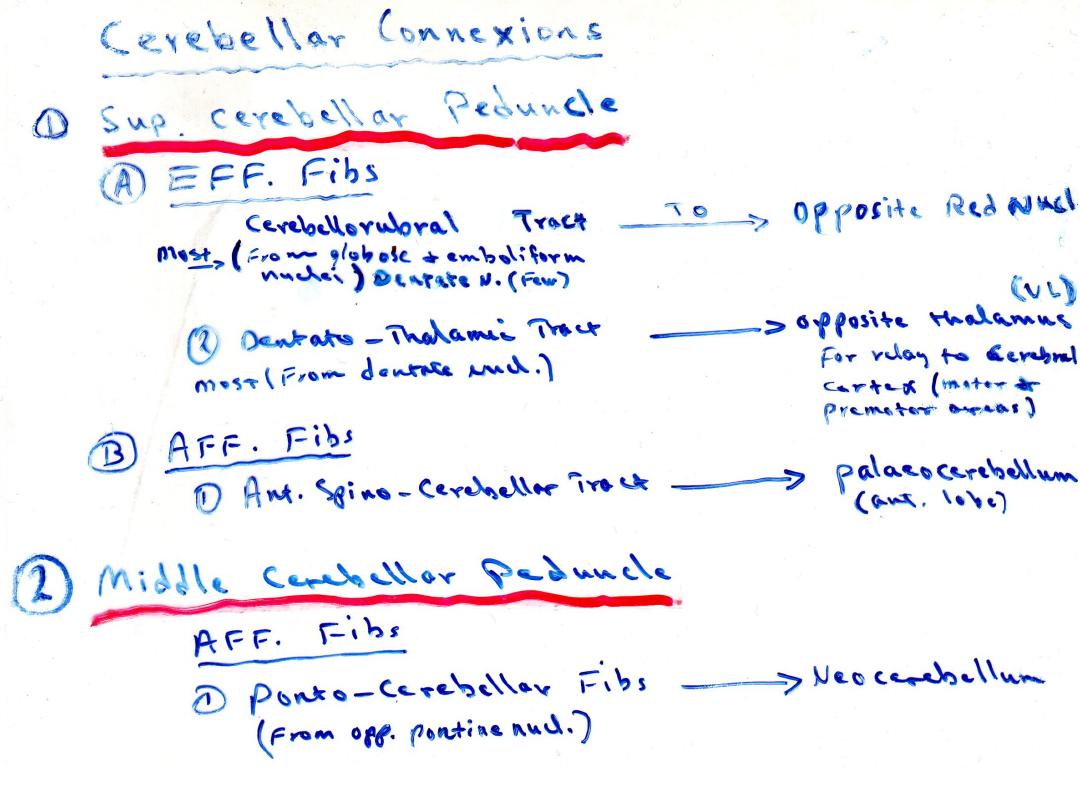
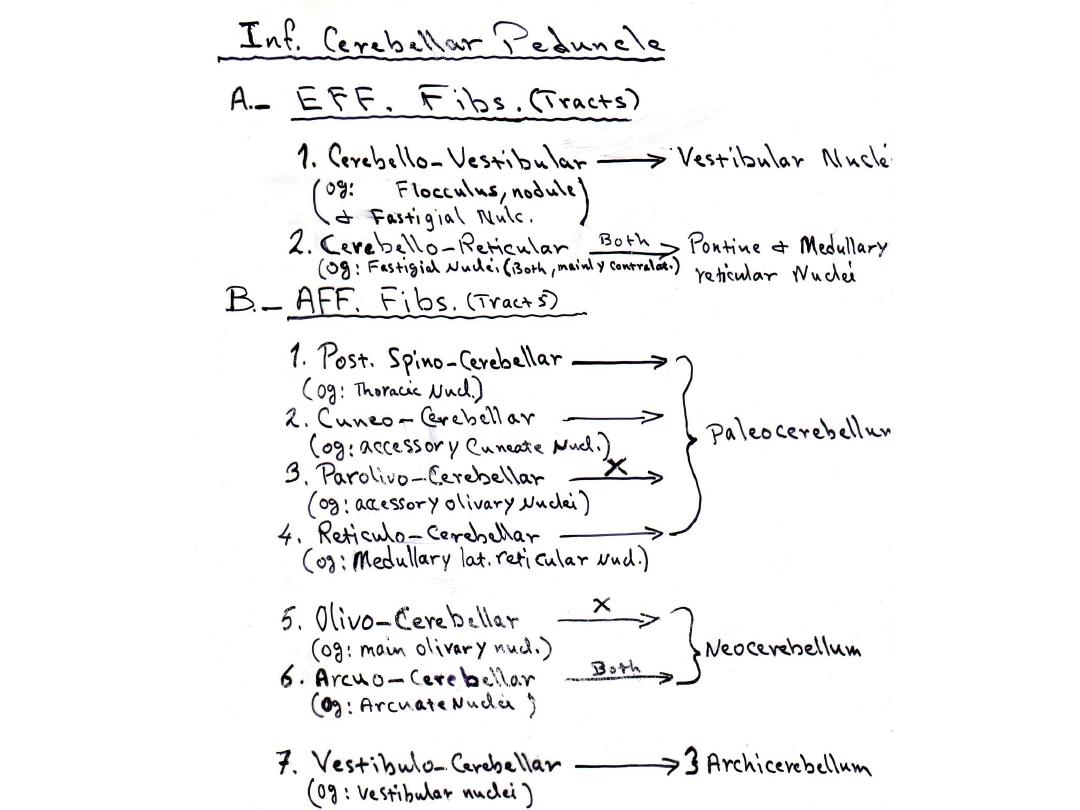
Cerebellar efferents
33
34
Afferents
From
Purkinje
Cells of
Paravermal
zone
Emboliforms
Globosus
(Paleocerebellum)
Sup.cerebellar ped.
Sup.cerebellar ped.
Red nucl.
(Opposite side)
Thalamus
(Opposite side)
Vestibular nuclei,
Reticular nuclei of
Pons & Medulla
Rubrospinal
tract
Vestibulospial
& Reticulospinal
tracts
(Archicerebellum)
(Neocerebellum)
Vermal zone
Lat. Hemispheric
zone
Fastigii
Inf. Cerebellar ped.
Dentate
Dentatothalamic
tract
Eff.
Eff.
Eff.
Deep cerebellar nuclei (Intrinsic nuclei)
1. Dentate
2. Emboliforms
3. Globosus Roof nuclei
4. Fastigii
-------------------------------------------------------------------------------------------------------------
Roof nuclei lie med. To hilum of Dentate nucl. & in the following order,
E G F (from Lateral to Medial)
35
36
37

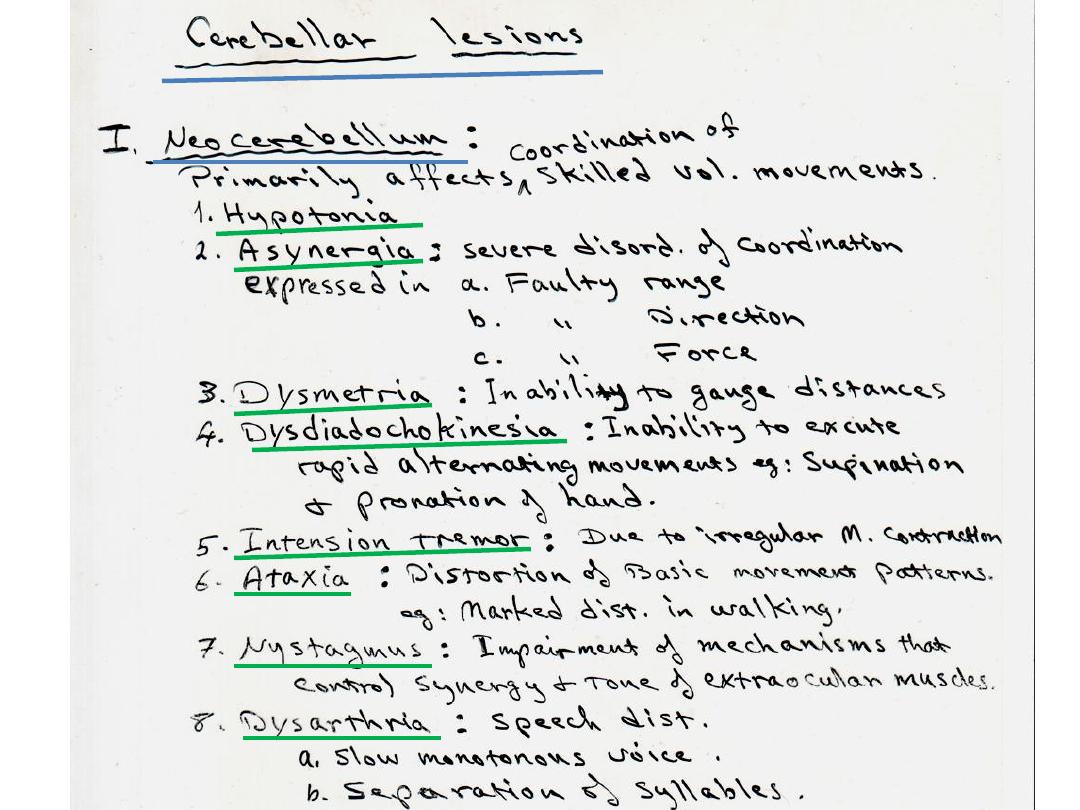
Cerebellar lesions
Lesion of neocerebellum
*Primarily affects coordination of skilled voluntary
movements
1.Hypotonia رُّت
َوَّتلا ُصْقَن
2.Asynergia رُزآَّتلا ُدْقَف
3.Dysmetria سايِقلا ُلَل َخ
4.Dysdiadochokinesia تاك
َ رَحلا ِةَّيِب ُوانَت ُلَلَخ
5.Intention tremor
ّيِد ْصَق ٌشاعُر
(
ةَك َر َحلا ُشاعُر
)
6.Ataxia حَن
َ ر
7.Nystagmus ةَأ
َرْأ َر
8.Dysarthria
ةَّتُر
(
ظُّفَلَّتلا ُر ْسُع
)
38
39
Blood Supply of Cerebellum
*All arteries anastomose with each other on cerebellar surface, but their
perforating branches into cerebellar substance are End Arteries (similar to
other parts of CNS)
1. Posterior Inferior Cerebellar Artery
* Most tortuous artery in body
* Supplies Choroid plexus of 4
th
. Ventricle & Pot. & Inf. Cerebellar surfaces.
* Adjacent parts of Medulla Oblongata.
2. Anterior Inferior Cerebellar Artery
* Arises from Basilar Art.
* Supply Inf. Cerebellar Surface & Flocculus.
* Give rise to Labyrinthine art.
3. Superior Cerebellar Artery
* Arises from Basilar Art.
* Supply Sup. Surface of Cerebellum.
Venous drainage
* Sup. & Post. Surfaces drain into Straight & Transverse sinuses
* Inf. Surface drains into Inf. Petrosal, Sigmoid & Occipital sinuses.
* Sup. Vermis drains into Great Cerebral Vein
40