AFTER MID
LEC: 2
DR. KHUDAIR
Oncology
Radiotherapy
TOTAL LEC: 2
Dr. Khudair

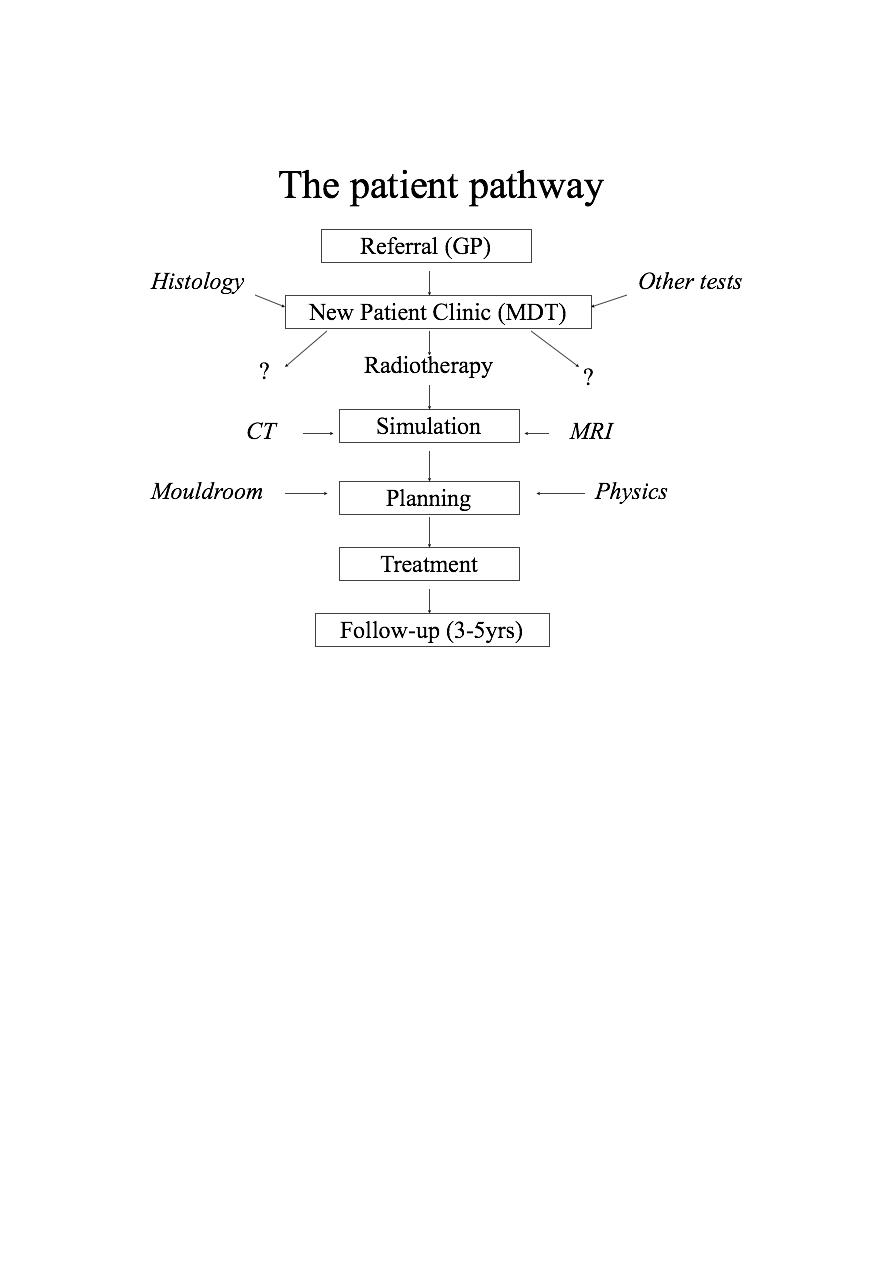
Radiotherapy – an overview
Dr.Khdhair Al-Rawaq
Radiotherapy – (medicine) ‘…the treatment of disease (especially cancer)
by exposure to radiation from a radioactive source or substance’
•
History and development of the use of radiation in medicine
•
What is cancer and what causes it?
•
Different types of radiotherapy – external beam, brachytherapy
and unsealed sources
•
Example patients and future advances
The past
William Conrad Roentgen (1845-1923)
Discovered x-rays in 1895 which revolutionised the field of physics and
medicine
William Crookes (1832-1919).
The Crookes tube – investigated behaviour of cathode rays in evacuated
glass tubes
Roentgen’s Laboratory in Wurzburg. Working with shrouded Crookes
tubes, noticed a barium screen across the room glowing. The birth of the
x-ray.
Radiograph of Frau Roentgen’s left hand
Roentgen’s x-ray apparatus.
Note the lack of any shielding around the Crookes tube.
Henri Becquerel (1852-1908)
Marie Curie (1867-1934)
Ernest Rutherford (1871-1937)
Early departments
Glasgow Royal Infirmary (1903).
Using a platinum target, x-rays could be focussed thus making useful
radiographs possible
Early radiotherapy for
breast cancer (1903).
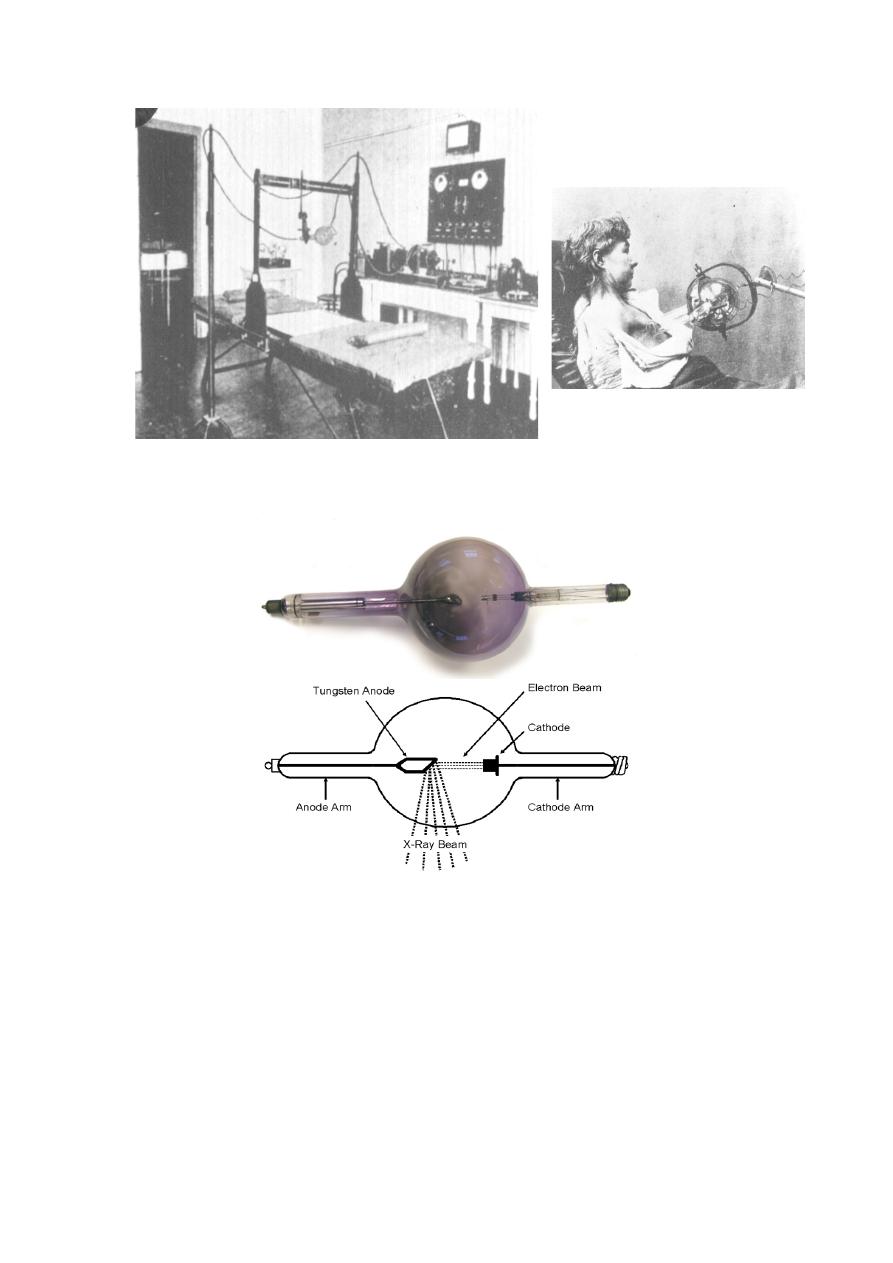
The Coolidge x-ray tube (1920)
The basic design is the same today
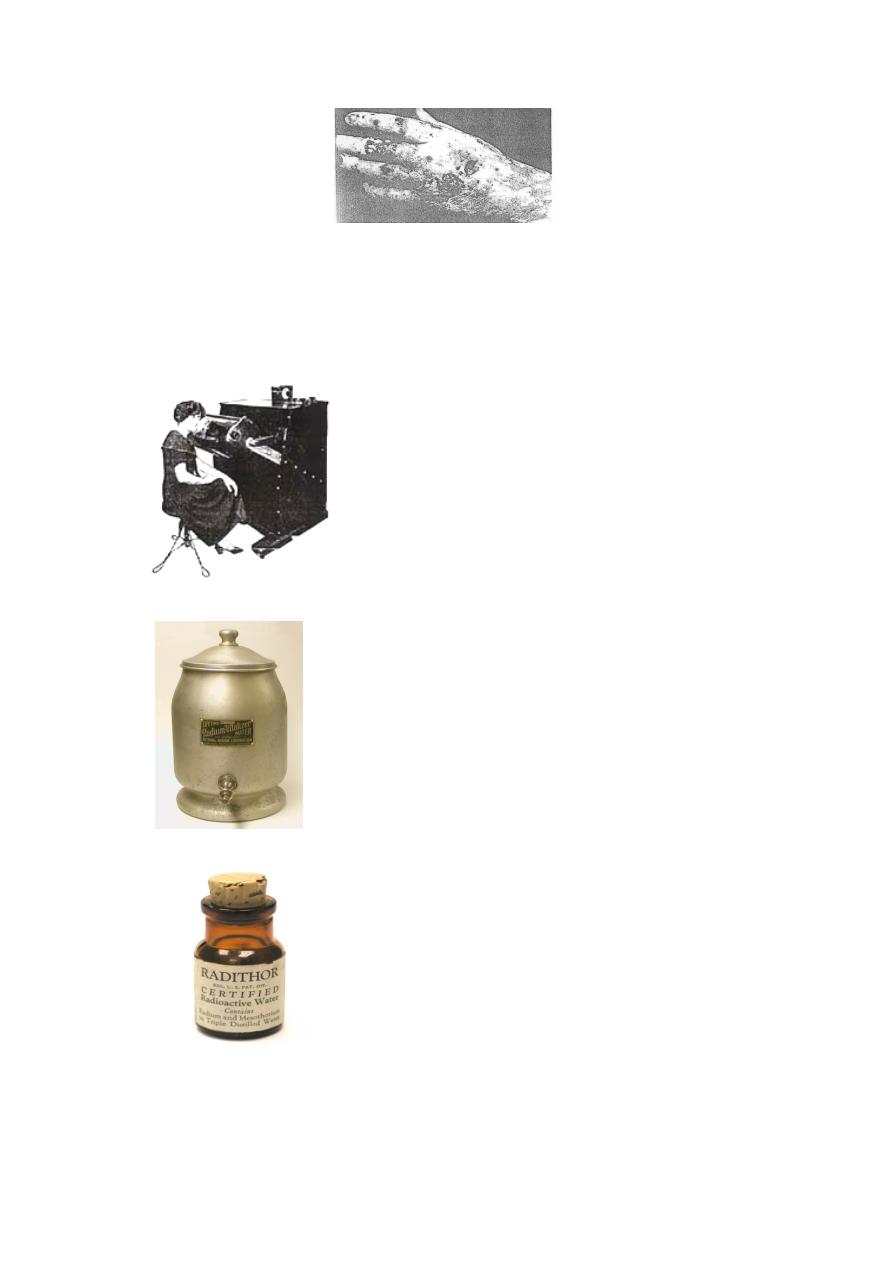
Radiation damage
Radiation-induced ulceration of a physician who used x-rays for 8 years.
In the early days little was known about the dangers of radiation.
Quack cures
The ‘Tricho System’ (early 1920s) was one of a
number of systems which used x-rays to
remove unwanted hair
The ‘curative’ properties of spa water was thought
to be due to radon gas, hence the invention of
handy devices for home use
‘Radithor’ (1928)
The truth starts to sink in…….
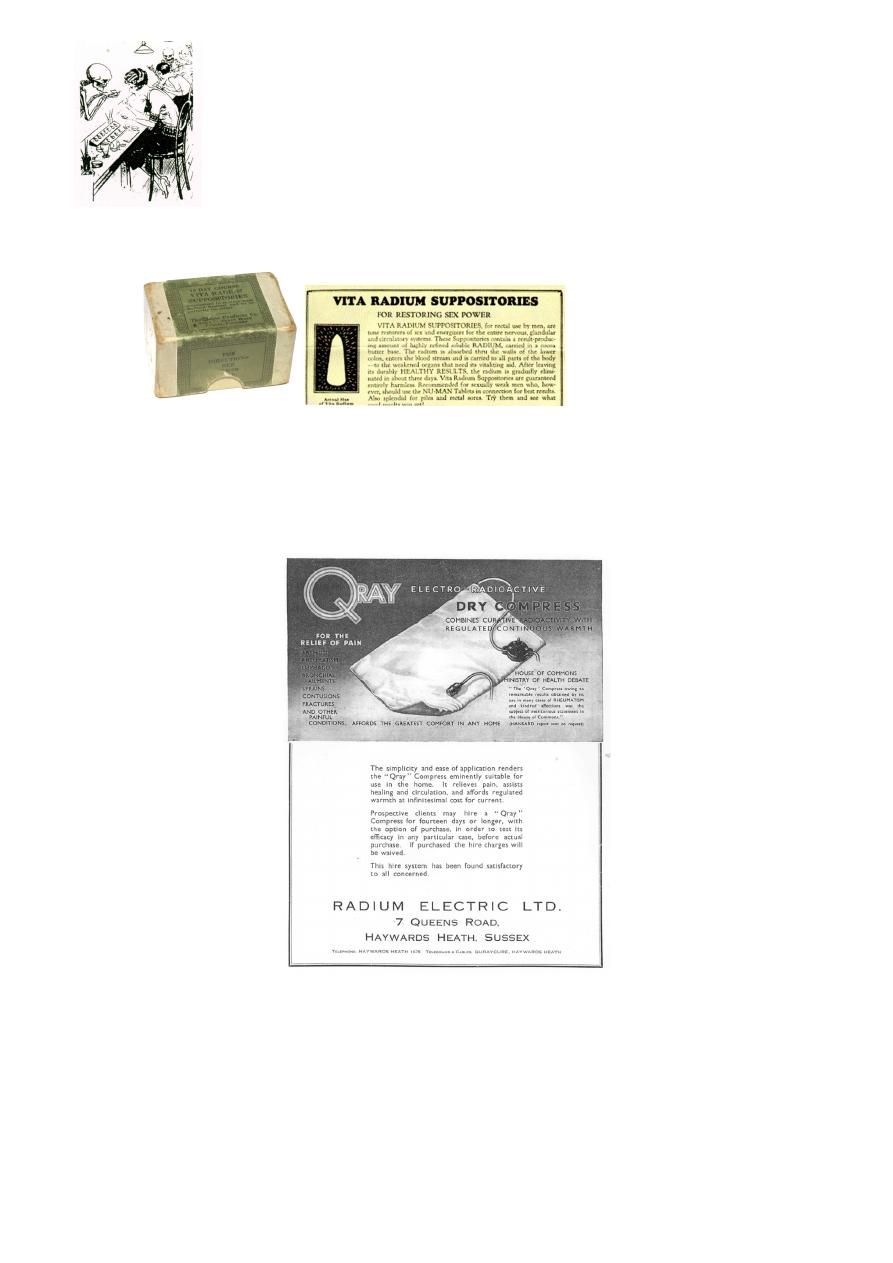
‘New York newspaper cartoon alluding to the ‘radium
poisoning’ of the watch dial painters (1924)
(1930)
Advert for the ‘Qray Compress – invaluable in the treatment of
bronchitis, colics, fractures, gout, insomnia, lumbago, shock, strains, etc’
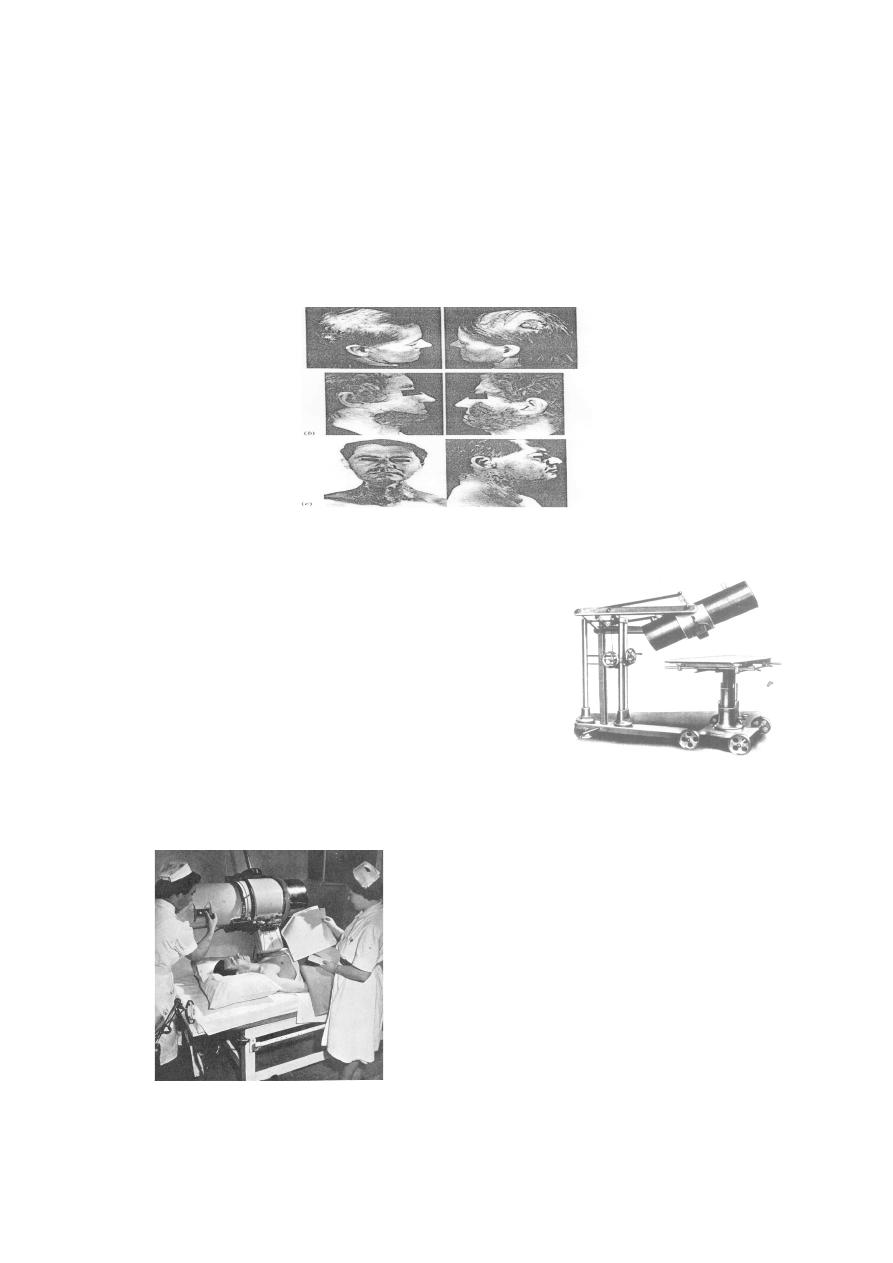
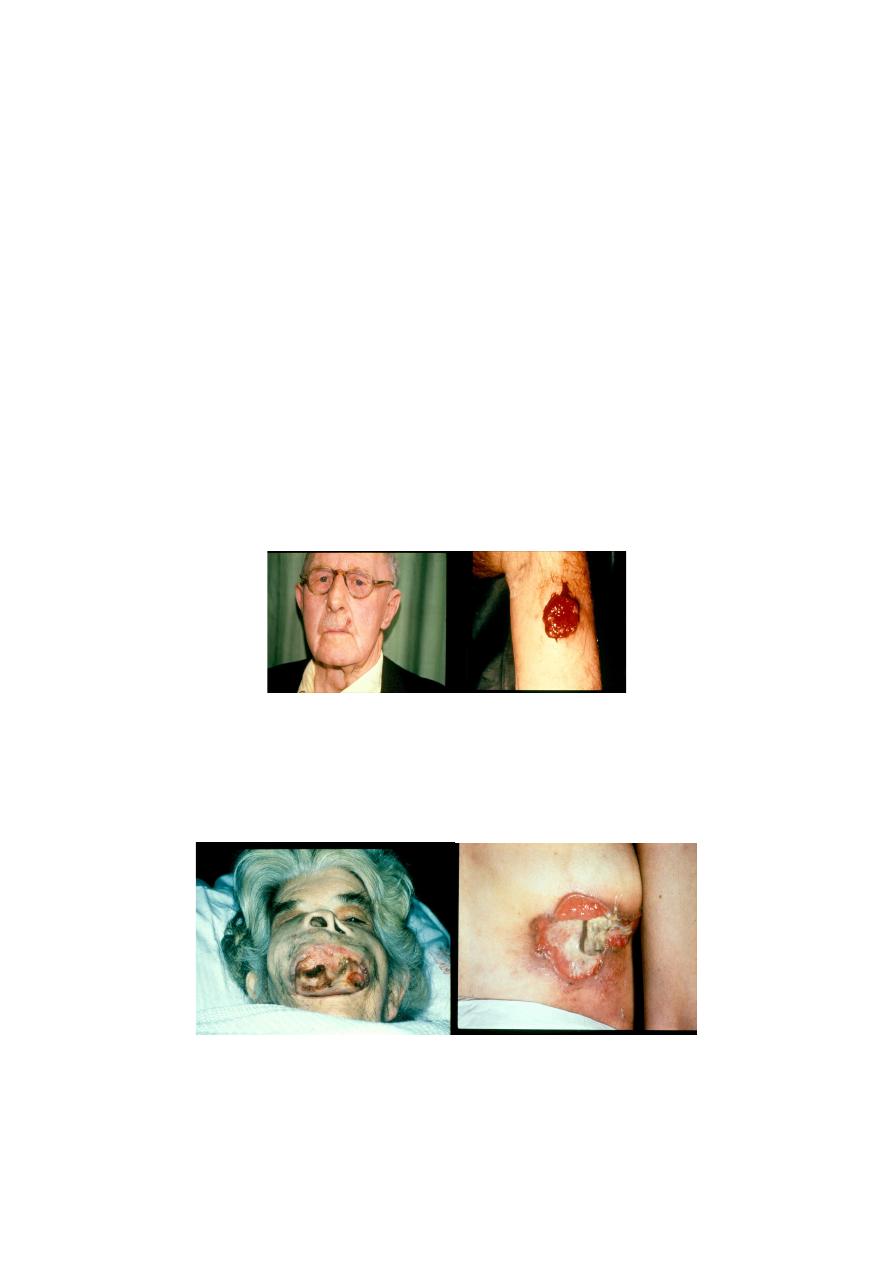
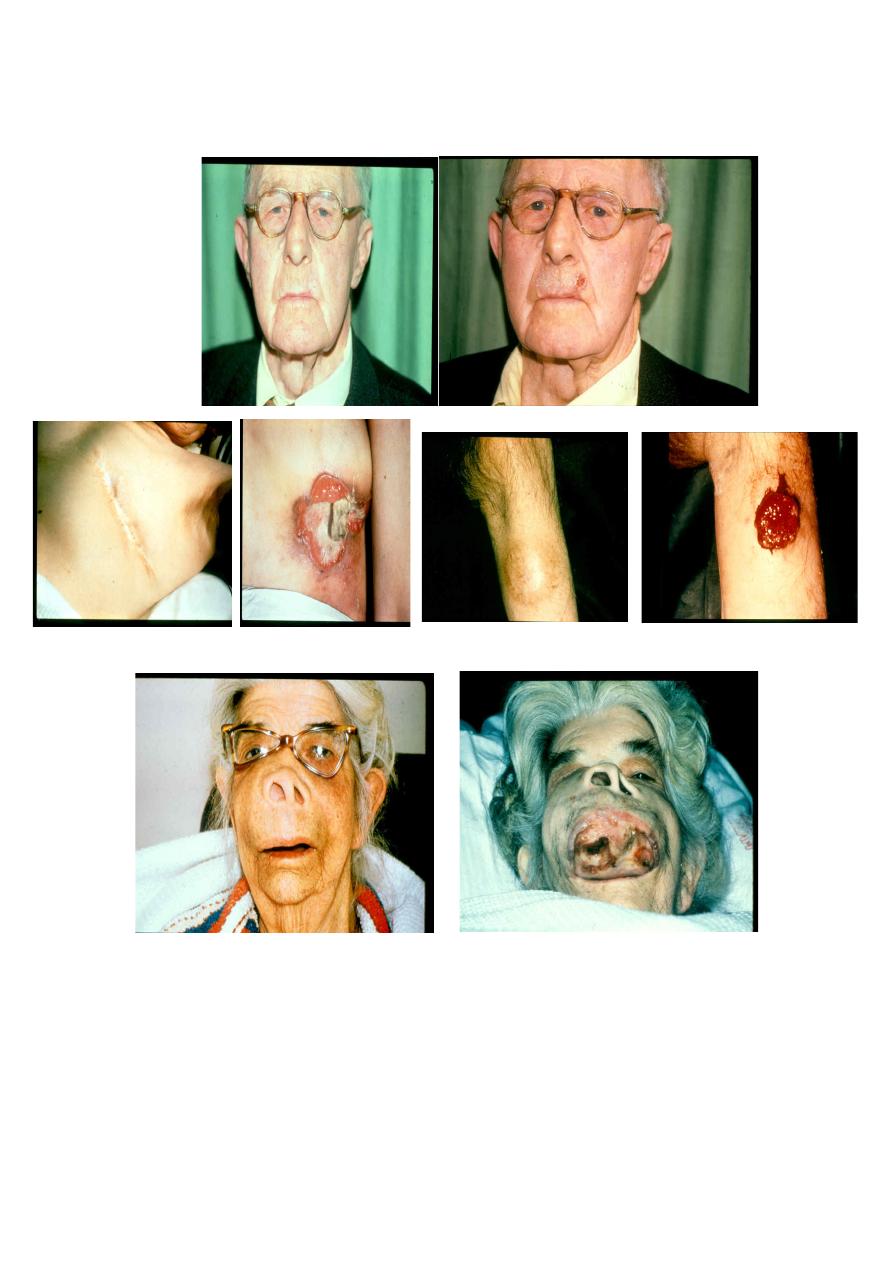
Radiation-induced cancers
Basal cell carcinoma of scalp 24 years after treatment for ringworm
-
1
Squamous cell carcinoma 50 years after x-ray treatment of facial hair
-
2
Thyroid carcinoma 42 years after treatment in 1912 for enlarged lymph nodes
-
3
)ﻣﺛل ﻣﻣوﺿﺢ ﺑﺎﻟرﺳم اﻟﺟوه اﻟﻲ ھو
1
و
2
و
3
(
Radiotherapy from the 1920s
Deep x-ray therapy unit from the mid 1920s
Middlesex Hospital (1950)
The Metropolitan Vickers Deep X-ray Unit
(250kV)
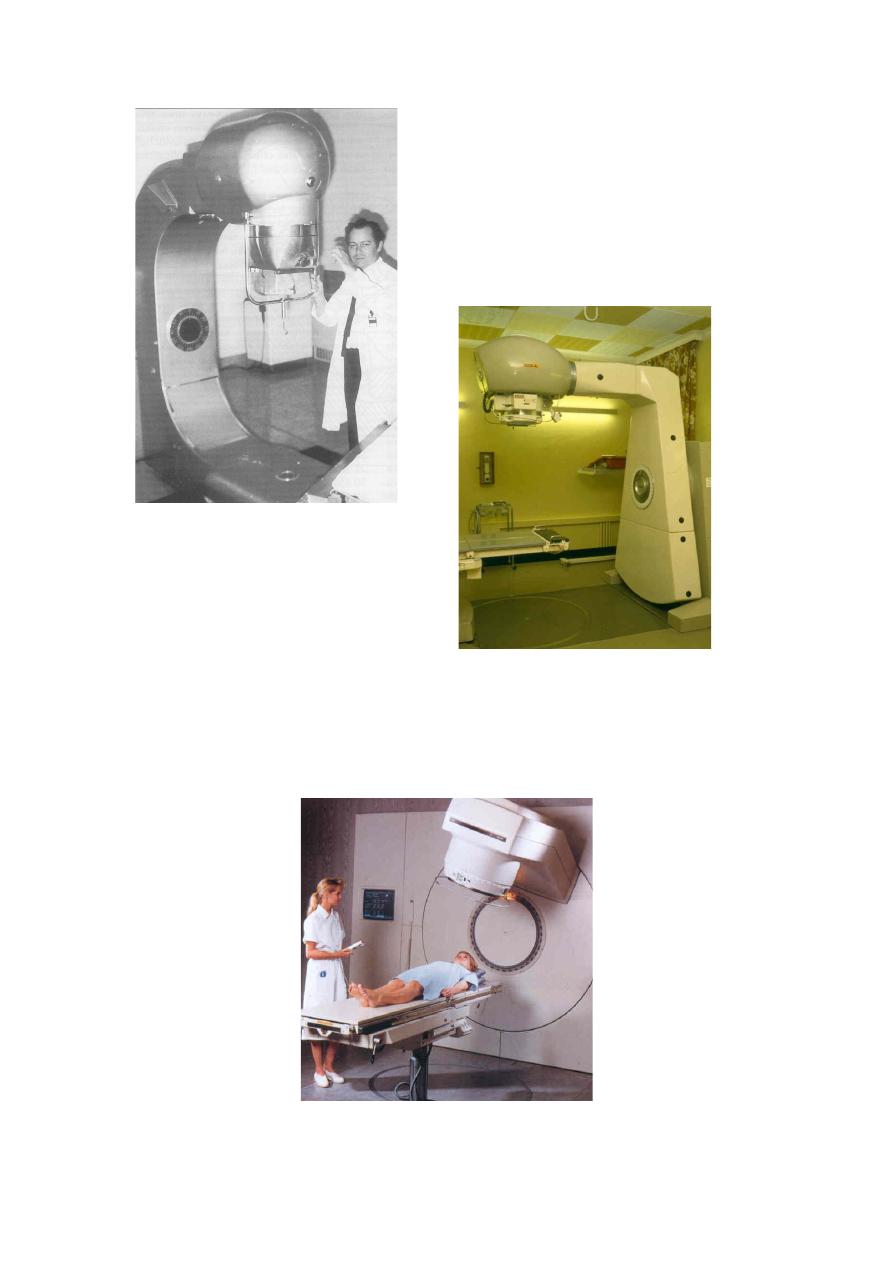
Early Cobalt Teletherapy Unit from the
1950s
Toronto, Canada
‘Mobaltron’ Cobalt Unit (1972)
Portsmouth
An ‘SL75’ linear accelerator (1998)
What is cancer?
•
1 in 4 deaths per year are cancer related
•
Subtle (or dramatic) changes in DNA coding lead to loss of normal
cell mechanisms – differentiation, proliferation, adhesion and
apoptosis
•
Balance between population loss and gain is uncoupled, leading to
excessive proliferation – a tumour – and subsequent local invasion
and metastasis
•
Everyone has a cancer at some point – controlled by normal
defence mechanisms
SCC above knee
Typical small basal cell ca
Stage 3 breast tumour
Extensive tumour upper palate

The causes of cancer
•
Genetic – oncogene over-expression, loss of tumour suppressor
genes, various syndromes
•
Chemical – smoking, asbestos, dyes, soot, oils, chrome, arsenic,
alcohol, diet?
•
Physical – solar radiation (UV), ionising radiation (radon, medical),
heat, trauma
•
Viral – human papilloma virus (cervix), T-cell types (HIV), hepatitis
B
•
Immune – AIDS, transplant patients
•
Endocrine – long-term oestrogen exposure?
To treat or not to treat?
•
Not every patient with cancer would benefit from active
treatment (surgery, radiotherapy, chemotherapy, hormonal)
•
Treatment should always have a positive benefit for the patient
but the outcome is not always predictable
•
Balancing the probability of improving patient’s condition,
whether by palliative symptom control or radical cure, against the
discomfort caused, the disturbance to lifestyle and the risk of
induced cancer
Radical and palliative
•
Radical – treatment given with the intent of long-term control or
cure
•
Palliative – improves quality of life or treats symptoms with no
implied impact on survival
Sometimes difficult to define aims in these terms
•
Adjuvant – prophylactic use of local or systemic treatment,
following a radical approach, to prevent recurrence (chemo,
hormonal).
Physics of Radiotherapy
•
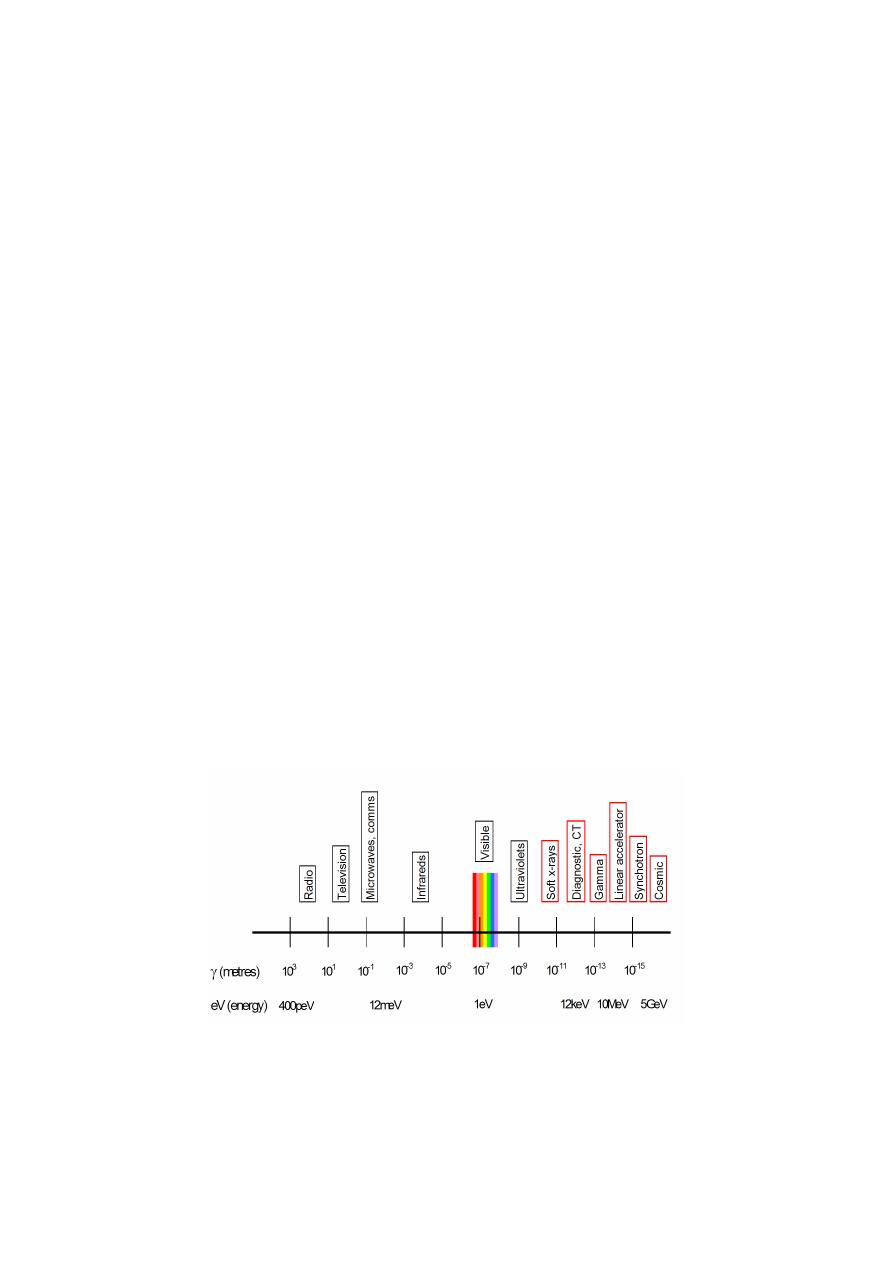
Both electromagnetic and particulate radiation is used in
radiotherapy
•
Electromagnetic radiation (photons) for external beam are
generated in x-ray tubes or linear accelerators
•
Particulates (electrons, protons, neutrons) are either generated
artificially or are emitted following radioactive decay processes
The electromagnetic spectrum

Ionisation and absorbed dose
•
Photons interact with atomic structure (ionisation) – shell
electrons and more photons are scattered
•
The ‘free’ electrons are stopped quickly, releasing their energy
into tissue
•
Ionised DNA and free radicals cause cell damage – repair
commences
•
Severe damage is not repaired and cell dies
•
The amount of energy delivered to and retained in tissue is called
the ‘absorbed dose’
•
Unit of absorbed dose is the Gray
1 Gray = 1 Joule/kg
•
Absorbed dose decreases with depth – the depth dose curve
•
Increase photon beam energy = increase in depth dose
Typical depth dose curve
10 X 10 cm field
10MV photons
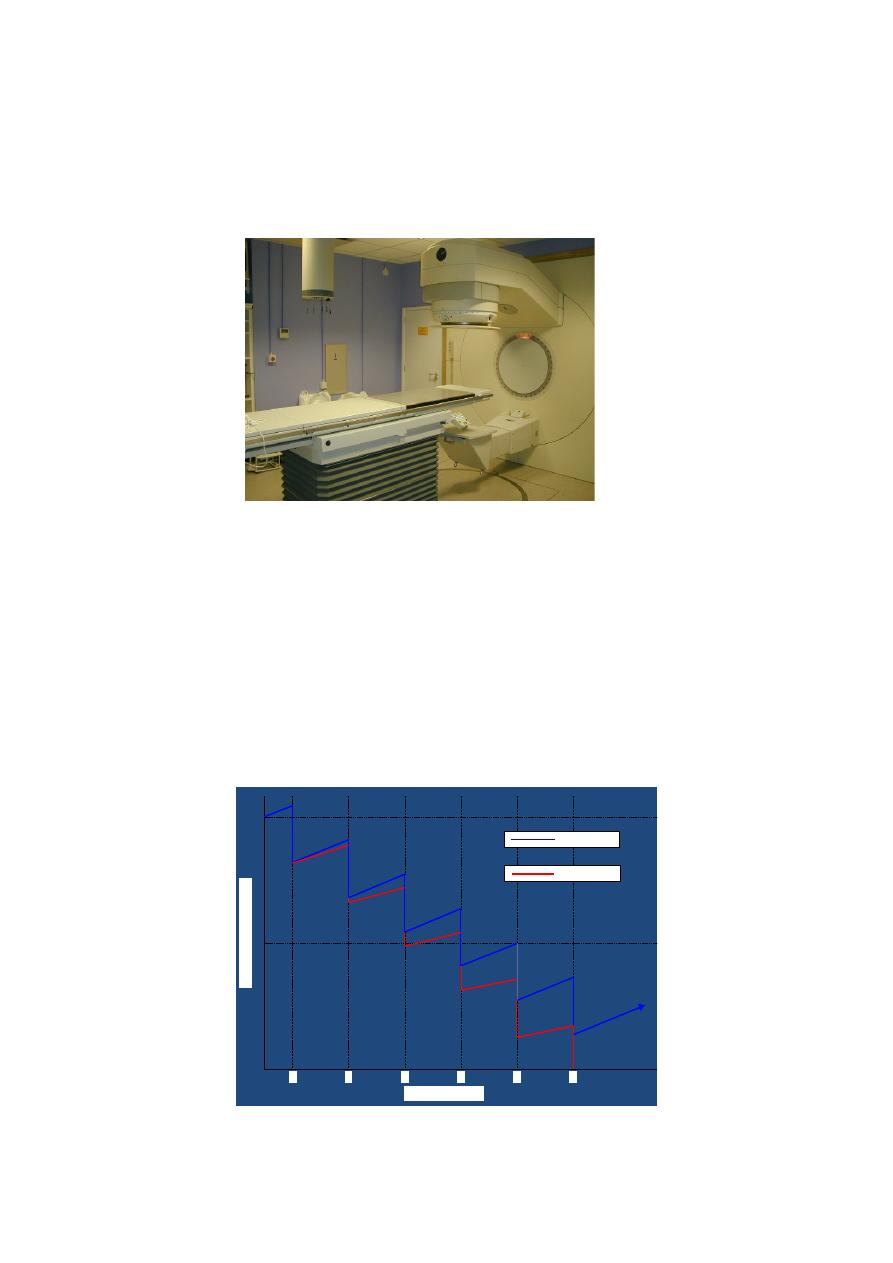
The Linear Accelerator
How does it work – fractionation
•
High energy radiation damages or destroys both normal and
tumour cells
•
In most cases, normal cell repair mechanisms are slightly more
efficient than those of tumour cells
•
Radical treatment doses are delivered in small daily fractions over
several weeks
Fractionation and survival
100
50
0
1
2
3
4
5
6
%
ce
ll
s
rem
ai
n
in
g
Treatment fraction
Normal cells
Tumour cells
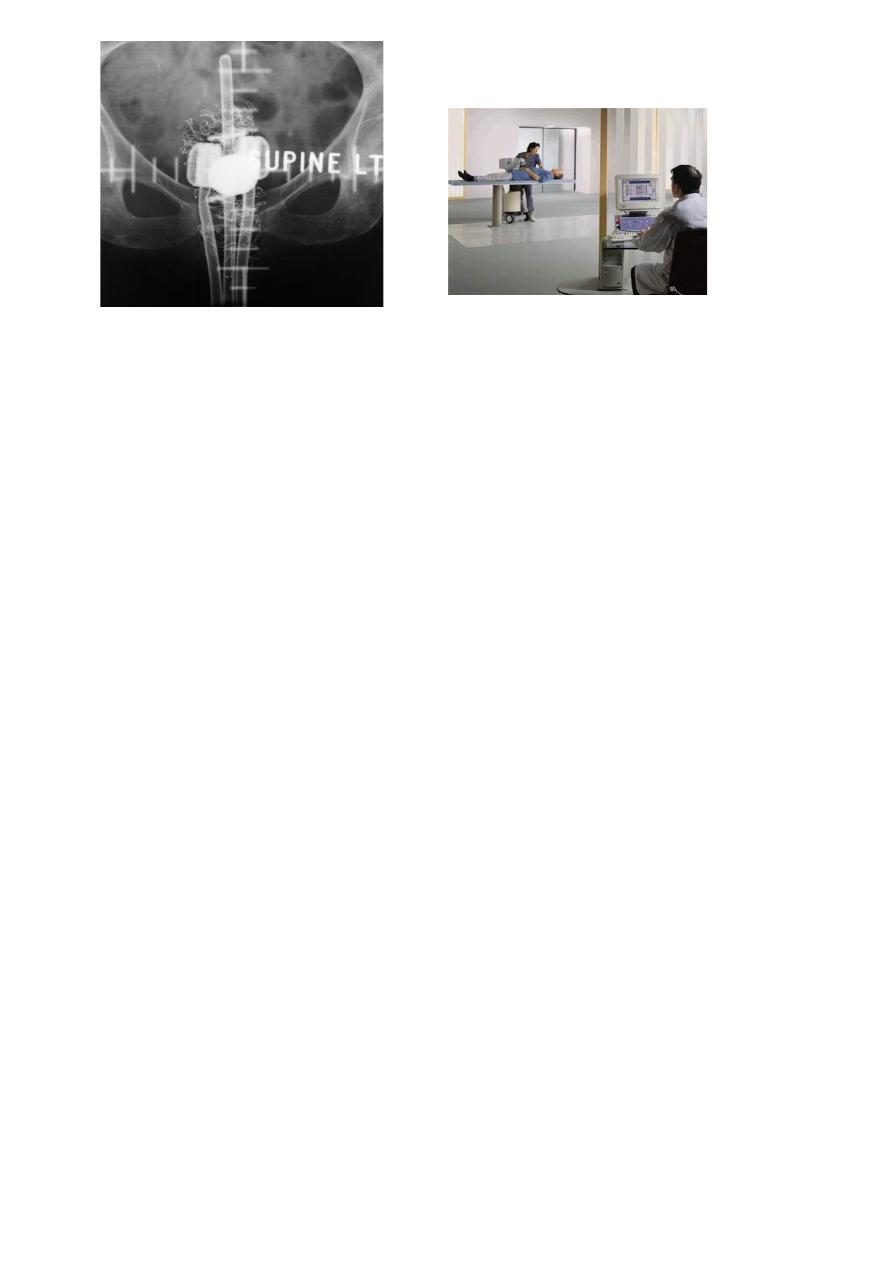
Delivering the dose
•
Palliative treatments – simple single or opposed fields using visual
marking or x-rays
(bony pain, advanced lung tumours, large brain tumours, obstruction,
haemorrhage)
•
Radical treatments – complex multi-field treatment plans using
image sets and customised field shapes
(prostate, bladder, head & neck sites, radical brain tumours, early
breast)
It’s all about accuracy
•
Need to deliver a high, even dose to the tumour, whilst avoiding
normal and sensitive tissue
•
Localisation of tumour volume is very important
•
Many diagnostic procedures available:
Diagnostic x-rays
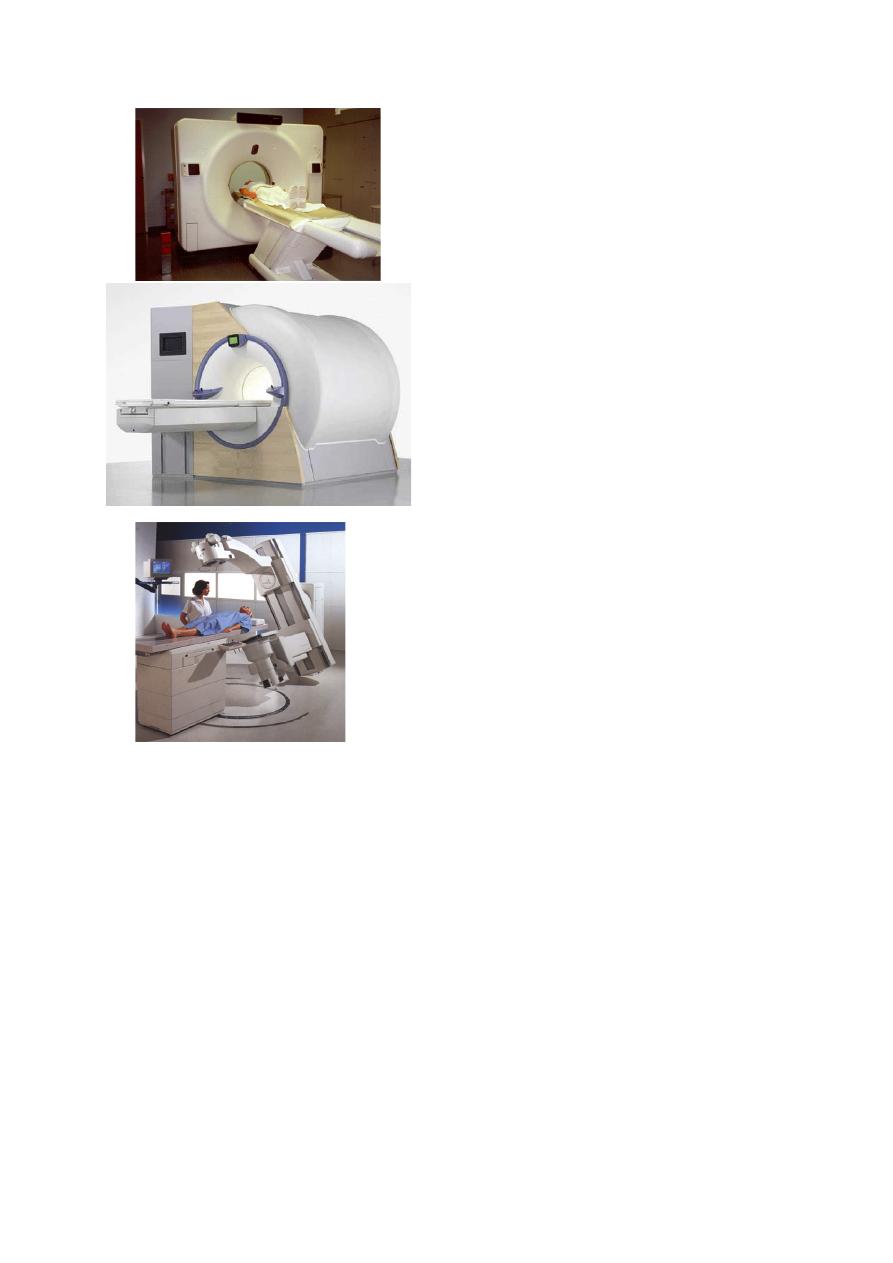
CT (Computerised Tomography
MRI (Magnetic Resonance Imaging)
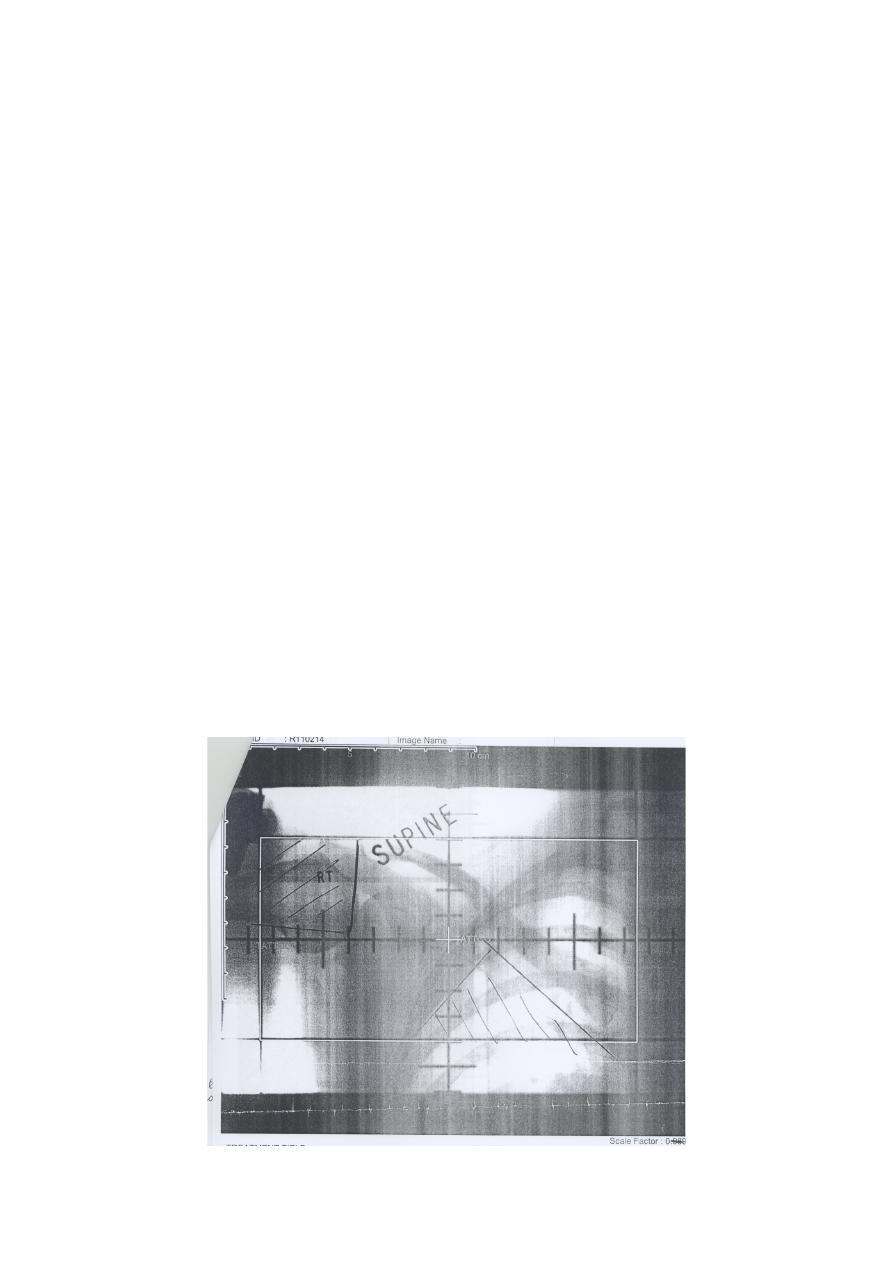
Radiotherapy simulator
it's all about accuracy
•
Need to deliver a high, even dose to the tumour, whilst avoiding
normal and sensitive tissue
•
Localisation of tumour volume is very important
•
Many diagnostic procedures available
•
Images from CT and MR scanners sent directly to planning system
•
Planner designs the treatment plan
ھﻲ ھﯾﺞ اﻟﻣﺣﺎظرة ﯾﻌﻧﻲ ﻣو ﺧﻠل,, ﮫﻌﺟارﻣ ﺎھورﺑﺗﻋا ﮫﻠﯾ ,, ةرﺗ ﺔﯾﻧﺎﺛ ةرﻣ تدﺎﻌﻧا)
:
D
(
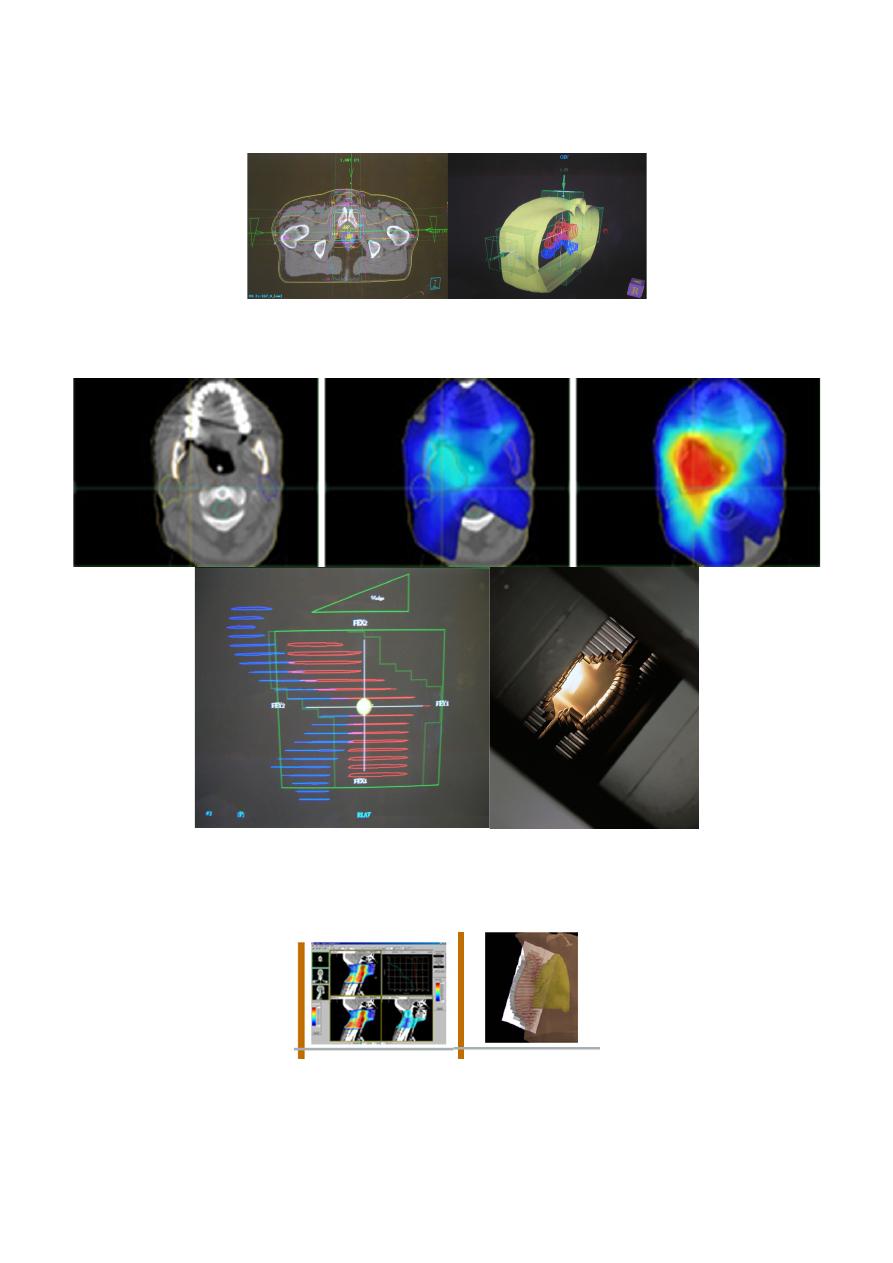
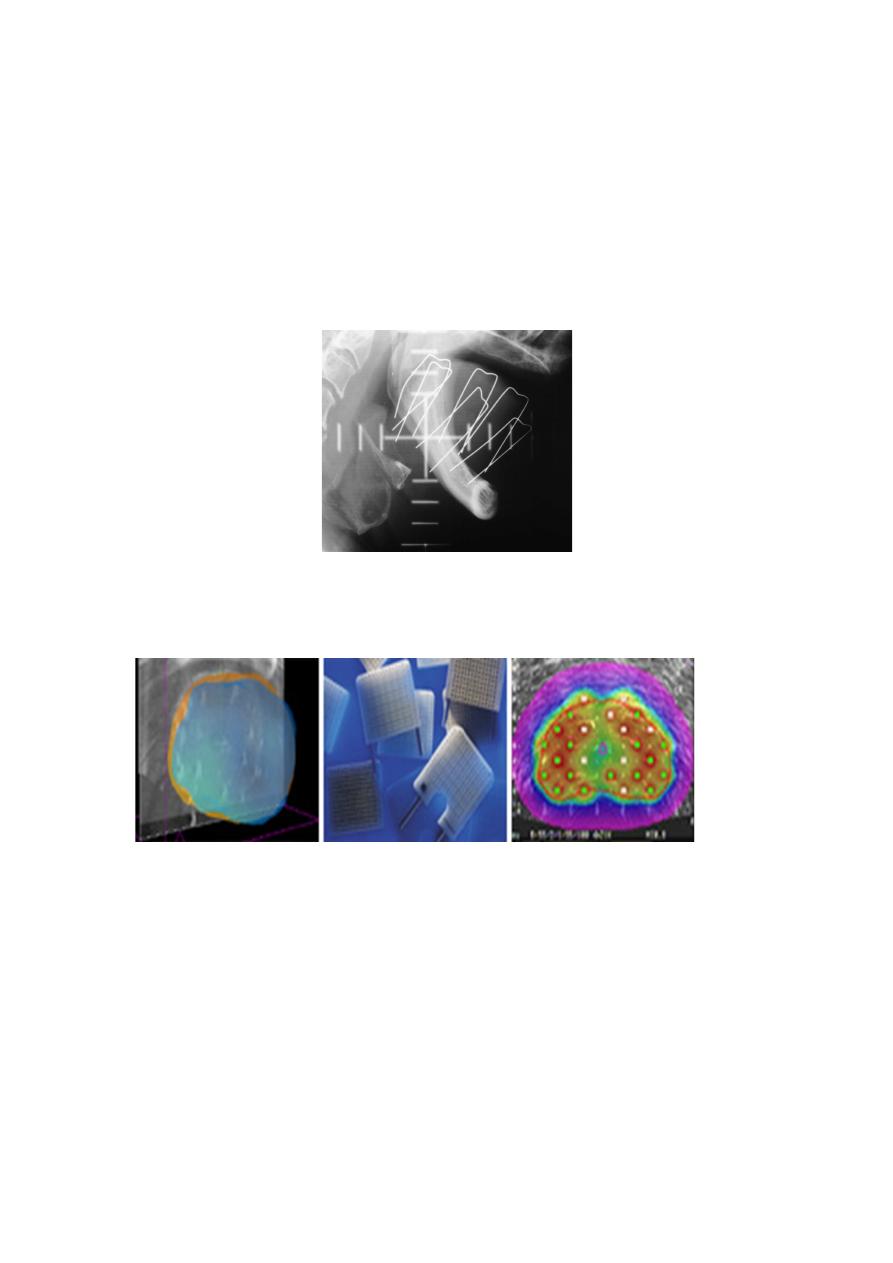
3D Conformal prostate plan with MLC
Multileaf collimator (MLC) array
The future – IMRT, IGRT
Side effects of radiotherapy
•
Toxicity divided into early or acute (during treatment) and late or
chronic (months or years after treatment)
•
Early effects include skin erythema, diarrhoea, hair loss, sickness
•
Late effects include fibrosis (lung, skin, bladder), perforation and
fistula, myelitis causing paraplegia, induced cancer
Brachytherapy
•
The use of sealed radioactive sources placed on or within tissue
•
Sealed source – the isotope is encapsulated and secure under high
degree of physical or chemical stress
•
High dose rates near source with rapid fall-off at distance
•
Interstitial, intracavitary, surface application
Interstitial treatments
•
192
Ir (Iridium)
Breast, anal and vaginal implants using iridium wire in steel needles
Tongue implants using hairpins
•
198
Au (Gold) and
125
I (Iodine)
Seeds, for tongue and prostate. Permanent implant
Intracavitary treatments
•
137
Cs (Ceasium)
Cervix & vagina using afterloaded source trains in plastic applicators.
•
192
Ir (Iridium)
The Microselectron - small, active source driven into applicators
Surface applicators
•
Use of surface applicators (or moulds) has diminished with the
onset of electron treatments
•
90
Sr (Stontium) still used in some centres for low-energy beta
treatment of opthalmic corneal vasularization.
Unsealed sources
•
Isotope administered in liquid or colloid form
•
Mainly beta emitters
•
Systemic or targetted - relies on the chemical preference of target
organ in uptake
131
I (Iodine) in saline for thyroid tumours
89
Sr (Strontium) as a chloride for bone deposits
32
P (Phosphate) for polycythaemia vera
Radiation synovectomy, radiolabelled antibodies
Does it work?
The End
Done by :Hussein Sadun Al-Nuaimy
7\3\2016