PARTURITION
Lecture 815-3-2016
INCREASED UTERINE EXCITABILITY NEAR TERM
Parturition means birth of the baby. Toward the end of pregnancy, the uterus becomes progressively more excitable, until finally it develops such strong rhythmical contractionsthat the baby is expelled. The exact cause of the increased activity of the uterus is not known, but at least two major categories of effects lead up to the intense contractions responsible for parturition: (1) progressive hormonal changes that cause increased excitability of the uterine musculature and (2) progressive mechanical changes.
Hormonal Factors That Increase Uterine Contractility
1-Increased Ratio of Estrogens to Progesterone. Progesterone inhibits uterine contractility during pregnancy, thereby helping to prevent expulsion of the fetus.Conversely, estrogens have a definite tendency to increase the degree of uterine contractility, partly because estrogens increase the number of gap junctions between the
adjacent uterine smooth muscle cells, but also because of other poorly understood effects. Both progesterone and estrogen are secreted in progressively greater quantities
throughout most of pregnancy, but from the seventh month onward, estrogen secretion continues to increase while progesterone secretion remains constant or perhaps
even decreases slightly. Therefore, it has been postulated that the estrogen-to-progesterone ratio increases sufficiently toward the end of pregnancy to be at least partly
responsible for the increased contractility of the uterus.
2-Oxytocin Causes Contraction of the Uterus. Oxytocin, a hormone secreted by the neurohypophysis, specifically causes uterine contraction. There are four reasons to believe that oxytocin might be important in increasing the contractility of the uterus near term:
1. The uterine muscle increases its oxytocin receptors and therefore increases its responsiveness to a given dose of oxytocin during the latter few months of
pregnancy.
2. The rate of oxytocin secretion by the neurohypophysis is considerably increased at the time of labor.
3. Although hypophysectomized animals can still deliver their young at term, labor is prolonged.
4. Experiments in animals indicate that irritation or stretching of the uterine cervix, as occurs during labor, can cause a neurogenic reflex through the paraventricular and supraoptic nuclei of the hypothalamus that causes the posterior pituitary gland
(the neurohypophysis) to increase its secretion of oxytocin.
3-Effect of Fetal Hormones on the Uterus. The fetus’s pituitary gland secretes increasing quantities of oxytocin, which might play a role in exciting the uterus. Also, the
fetus’s adrenal glands secrete large quantities of cortisol, another possible uterine stimulant. In addition, the fetal membranes release prostaglandins in high concentration
at the time of labor. These prostaglandins, too, can increase the intensity of uterine contractions.
Mechanical Factors That Increase Uterine Contractility
1-Stretch of the Uterine Musculature. Simply stretching smooth muscle organs usually increases their contractility. Further, intermittent stretch, which occurs repeatedly in the uterus because of fetal movements, can also elicit smooth muscle contraction. Note especially that twins are born, on average, 19 days earlier than a single child, whichemphasizes the importance of mechanical stretch in eliciting uterine contractions.
2-Stretch or Irritation of the Cervix. There is reason to believe that stretching or irritating the uterine cervix is particularly important in eliciting uterine contractions.
For instance, obstetricians frequently induce labor by rupturing the membranes so the head of the baby stretches the cervix more forcefully than usual or irritates it in
other ways.
The mechanism by which cervical irritation excites the body of the uterus is not known. It has been suggested that stretching or irritation of nerves in the cervix initiates reflexes to the body of the uterus, but the effect could also result simply from myogenic transmission of signals from the cervix to the body of the uterus.
ONSET OF LABOR—A POSITIVE FEEDBACK MECHANISM FOR ITS INITIATION
During most of the months of pregnancy, the uterus undergoes periodic episodes of weak and slow rhythmical contractions called Braxton Hicks contractions. These contractions become progressively stronger toward the end of pregnancy; then they change suddenly, within hours, to become exceptionally strong contractions that start stretching the cervix and later force the baby through the birth canal, thereby causing parturition. This processis called labor, and the strong contractions that result in final parturition are called labor contractions.
We do not know what suddenly changes the slow, weak rhythmicity of the uterus into strong labor contractions. However, on the basis of experience with other types of
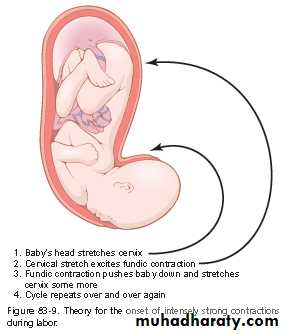
physiological control systems, a theory has been proposed to explain the onset of labor. The positive feedback theory suggests that stretching of the cervix by the fetus’s
head finally becomes great enough to elicit a strong reflex increase in contractility of the uterine body. This pushes the baby forward, which stretches the cervix more and
initiates more positive feedback to the uterine body. Thus, the process repeats until the baby is expelled. This theory is shown in Figure 83-9, and the following observations
support this theory.
First, labor contractions obey all the principles of positive feedback. That is, once the strength of uterine contraction becomes greater than a critical value, each contraction leads to subsequent contractions that become stronger and stronger until maximum effect is achieved. By referring to the discussion in Chapter 1 of positive feedback in control systems, one can see that this is the precise nature of all positive feedback mechanisms
when the feedback gain becomes greater than a critical value.
Second, two known types of positive feedback increase uterine contractions during labor: (1) Stretching of the cervix causes the entire body of the uterus to contract, and this contraction stretches the cervix even more because of the downward thrust of the baby’s head, and (2) cervical stretching also causes the pituitary gland to secrete oxytocin, which is another means for increasing uterine contractility.
To summarize, we can assume that multiple factors increase the contractility of the uterus toward the end of pregnancy. Eventually a uterine contraction becomes strong enough to irritate the uterus, especially at the cervix, and this irritation increases uterine contractility still more because of positive feedback, resulting in a second uterine contraction stronger than the first, a third stronger than the second, and so forth. Once these contractions become strong enough to cause this type of feedback, with each succeeding contraction greater than the preceding one, the process proceeds to completion. One might ask about the many instances of false labor, in which the contractions become stronger and
stronger and then fade away. Remember that for a positive feedback to continue, each new cycle of the positive feedback must be stronger than the previous one. If at any
time after labor starts some contractions fail to re-excite the uterus sufficiently, the positive feedback could go into a retrograde decline and the labor contractions would
fade away.
ABDOMINAL MUSCLE CONTRACTIONS DURING LABOR
Once uterine contractions become strong during labor, pain signals originate both from the uterus and from the birth canal. These signals, in addition to causing suffering,elicit neurogenic reflexes in the spinal cord to the abdominal muscles, causing intense contractions of these muscles. The abdominal contractions add greatly to the force that
causes expulsion of the baby.
Mechanics of Parturition
The uterine contractions during labor begin mainly at the top of the uterine fundus and spread downward over the body of the uterus. Also, the intensity of contraction is great in the top and body of the uterus but weak in the lower segment of the uterus adjacent to the cervix.
Therefore, each uterine contraction tends to force the baby downward toward the cervix.
In the early part of labor, the contractions might occur only once every 30 minutes. As labor progresses, the contractions finally appear as often as once every 1 to 3 minutes and the intensity of contraction increases greatly, with only a short period of relaxation between contractions. The
combined contractions of the uterine and abdominal musculature during delivery of the baby cause a downward force on the fetus of about 25 pounds during each strong contraction.
It is fortunate that the contractions of labor occur intermittently, because strong contractions impede or sometimes even stop blood flow through the placenta and would cause death of the fetus if the contractions were continuous. Indeed, overuse of various uterine stimulants, such as
oxytocin, can cause uterine spasm rather than rhythmical contractions and can lead to death of the fetus.
In more than 95 percent of births, the head is the first part of the baby to be expelled, and in most of the remaining instances, the buttocks are presented first. Entering the birth canal with the buttocks or feet first is called a breech presentation.
The head acts as a wedge to open the structures of the birth canal as the fetus is forced downward. The first major obstruction to expulsion of the fetus is the uterine cervix. Toward the end of pregnancy, the cervix becomes soft, which allows it to stretch when labor contractions begin in the uterus. The so-called first stage of labor is a period of progressive cervical dilation,
lasting until the cervical opening is as large as the head of the fetus. This stage usually lasts for 8 to 24 hours in the first pregnancy but often only a few minutes after many pregnancies.
Once the cervix has dilated fully, the fetal membranes usually rupture and the amniotic fluid is lost suddenly through the vagina. Then the head of the fetus moves rapidly into the birth canal, and with additional force from above, it continues to wedge its way through the canal until
delivery occurs. This is called the second stage of labor, and it may last from as little as 1 minute after many pregnancies to 30 minutes or more in the first pregnancy.
Separation and Delivery of the Placenta
For 10 to 45 minutes after birth of the baby, the uterus continues to contract to a smaller and smaller size, which causes a shearing effect between the walls of the uterus and the placenta, thus separating the placenta from its implantation site. Separation of the placenta opens the placental sinuses and causes bleeding. The amount of bleeding is limited to an average of 350 milliliters by the following mechanism: The smooth muscle fibers of the uterine musculature
are arranged in figures of eight around the blood vessels as the vessels pass through the uterine wall. Therefore, contraction of the uterus after delivery of the baby constricts the vessels that had previously supplied blood to the placenta. In addition, it is believed that vasoconstrictor
prostaglandins formed at the placental separation site cause additional blood vessel spasm.
Labor Pains
With each uterine contraction, the mother experiences considerable pain. The cramping pain in early labor is probably caused mainly by hypoxia of the uterine muscle resulting from compression of the blood vessels in the uterus. This pain is not felt when the visceral sensory hypogastric nerves, which carry the visceral sensory fibers leading from the uterus, have been sectioned.During the second stage of labor, when the fetus is being expelled through the birth canal, much more severe pain is caused by cervical stretching, perineal stretching, and stretching or tearing of structures in the vaginal canal itself. This pain is conducted to the mother’s spinal cord and
brain by somatic nerves instead of by the visceral sensory nerves.
Involution of the Uterus After Parturition
During the first 4 to 5 weeks after parturition, the uterus involutes. Its weight becomes less than half its immediate postpartum weight within 1 week, and in 4 weeks, if the mother lactates, the uterus may become as small as it was before pregnancy. This effect of lactation results fromthe suppression of pituitary gonadotropin and ovarian hormone secretion during the first few months of lactation, as discussed later. During early involution of the uterus, the placental site on the endometrial surface autolyzes, causing a vaginal discharge known as lochia, which is first
bloody and then serous in nature and continues for a total of about 10 days. After this time, the endometrial surface becomes re-epithelialized and ready for normal, nongravid sex life again.