Pregnancy
Lecture 66/3/2014
In Chapters 80 and 81, the sexual functions of the male and female are described to the point of fertilization of the ovum. If the ovum becomes fertilized, a new sequence of events called gestation, or pregnancy, takes place, and the fertilized ovum eventually develops into a full-term fetus. The purpose of this chapter is to discuss the early stages of ovum development after fertilization and then to discuss the physiology of pregnancy.
Maturation and Fertilization of the Ovum
While still in the ovary, the ovum is in the primary oocyte stage. Shortly before it is released from the ovarian follicle, its nucleus divides by meiosis and a first polar body is expelled from the nucleus of the oocyte. The primary oocyte then becomes the secondary oocyte. In this process, each of the 23 pairs of chromosomes loses one of its partners, which becomes incorporated in a polar body that is expelled. This leaves 23 unpaired chromosomes in the secondary oocyte. It is at this time that the ovum, still in the secondary oocyte stage, is ovulated into the abdominal cavity. Then, almost immediately, it enters the fimbriated end of one of the fallopian tubes.
Entry of the Ovum into the Fallopian Tube (Oviduct). When ovulation occurs, the ovum, along with a hundred or more attached granulosa cells that constitute the corona radiata, is expelled directly into the peritoneal cavity and must then enter one of the fallopian tubes to reach the cavity of the uterus. The fimbriated ends of each fallopian tube fall naturally around the ovaries. The inner surfaces of the fimbriated tentacles are lined with ciliated epithelium, and the cilia are activated by estrogen from the ovaries, which causes the cilia to beat toward the opening, or ostium, of the involved fallopian tube. One can actually see a slow fluid current flowing toward the ostium. By this means, the ovum enters one of the fallopian tubes.
It seems likely that many ova might fail to enter the fallopian tubes. However, on the basis of conception studies, it is probable that as many as 98 per cent succeed in this task. Indeed, in some recorded cases, women with one ovary removed and the opposite fallopian tube removed have had several children with relative ease of conception, thus demonstrating that ova can even enter the opposite fallopian tube.
Fertilization of the Ovum. After the male ejaculates semen into the vagina during intercourse, a few sperm are transported within 5 to 10 minutes upward from the vagina and through the uterus and fallopian tubes to the ampullae of the fallopian tubes near the ovarian ends of the tubes. This transport of the sperm is aided by contractions of the uterus and fallopian tubes stimulated by prostaglandins in the male seminal fluid and also by oxytocin released from the posterior pituitary gland of the female during her orgasm. Of the almost half a billion sperm deposited in the vagina, a few thousand succeed in reaching each ampulla.
Fertilization of the ovum normally takes place in the ampulla of one of the fallopian tubes soon after both the sperm and the ovum enter the ampulla. But before a sperm can enter the ovum, it must first penetrate the multiple layers of granulosa cells attached to the outside of the ovum (the corona radiata) and then bind to and penetrate the zona pellucida surrounding the ovum itself.
Once a sperm has entered the ovum (which is still in the secondary oocyte stage of development), the oocyte divides again to form the mature ovum plus a second polar body that is expelled. The mature ovum still carries in its nucleus (now called the female pronucleus) 23 chromosomes. One of these chromosomes is the female chromosome, known as the X chromosome.
In the meantime, the fertilizing sperm has also changed. On entering the ovum, its head swells to form a male pronucleus, shown in Figure 82-1D. Later, the 23 unpaired chromosomes of the male pronucleus and the 23 unpaired chromosomes of the female pronucleus align themselves to re-form a complete complement of 46 chromosomes (23 pairs) in the fertilized ovum (see Figure 82-1E).
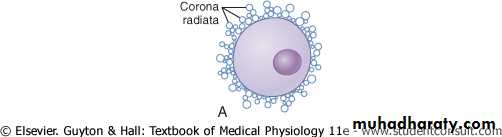
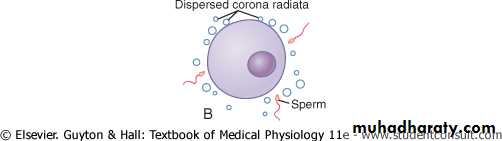
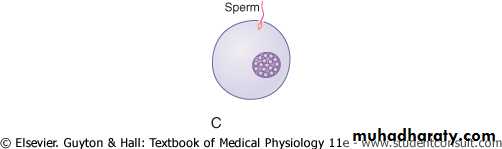
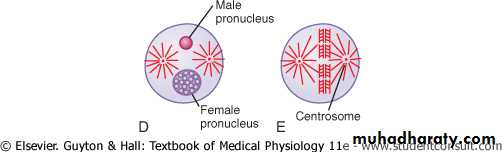
Figure 82-1 Fertilization of the ovum. A, The mature ovum surrounded by the corona radiata. B, Dispersal of the corona radiata. C, Entry of the sperm. D, Formation of the male and female pronuclei. E, Reorganization of a full complement of chromosomes and beginning division of the ovum.
What Determines the Sex of the Fetus That Is Created? After formation of the mature sperm, half of these carry in their genome an X chromosome (the female chromosome) and half carry a Y chromosome (the male chromosome). Therefore, if an X chromosome from a sperm combines with an X chromosome from an ovum, giving an XX combination, a female child will be born. But if a Y chromosome from a sperm is paired with an X chromosome from an ovum, giving an XY combination, a male child will be born.
Transport of the Fertilized Ovum in the Fallopian Tube
After fertilization has occurred, an additional 3 to 5 days is normally required for transport of the fertilized ovum through the remainder of the fallopian tube into the cavity of the uterus (Figure 82-2). This transport is effected mainly by a feeble fluid current in the tube resulting from epithelial secretion plus action of the ciliated epithelium that lines the tube; the cilia always beat toward the uterus. Weak contractions of the fallopian tube may also aid the ovum passage.The fallopian tubes are lined with a rugged, cryptoid surface that impedes passage of the ovum despite the fluid current. Also, the isthmus of the fallopian tube (the last 2 centimeters before the tube enters the uterus) remains spastically contracted for about the first 3 days after ovulation. After this time, the rapidly increasing progesterone secreted by the ovarian corpus luteum first promotes increasing progesterone receptors on the fallopian tube smooth muscle cells; then the progesterone activates the receptors, exerting a tubular relaxing effect that allows entry of the ovum into the uterus.
This delayed transport of the fertilized ovum through the fallopian tube allows several stages of cell division to occur before the dividing ovum-now called a blastocyst, with about 100 cells-enters the uterus. During this time, the fallopian tube secretory cells produce large quantities of secretions used for the nutrition of the developing blastocyst.
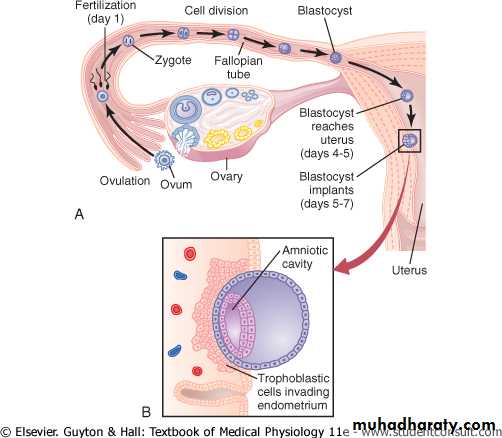
Figure 82-2 A, Ovulation, fertilization of the ovum in the fallopian tube, and implantation of the blastocyst in the uterus. B, Action of trophoblast cells in implantation of the blastocyst in the uterine endometrium.
Implantation of the Blastocyst in the Uterus
After reaching the uterus, the developing blastocyst usually remains in the uterine cavity an additional 1 to 3 days before it implants in the endometrium; thus, implantation ordinarily occurs on about the fifth to seventh day after ovulation. Before implantation, the blastocyst obtains its nutrition from the uterine endometrial secretions, called "uterine milk."
Early Nutrition of the Embryo
In Chapter 81, we pointed out that the progesterone secreted by the ovarian corpus luteum during the latter half of each monthly sexual cycle has an effect on the uterine endometrium, converting the endometrial stromal cells into large swollen cells containing extra quantities of glycogen, proteins, lipids, and even some minerals necessary for development of the conceptus. Then, when the conceptus implants in the endometrium, the continued secretion of progesterone causes the endometrial cells to swell further and to store even more nutrients. These cells are now called decidual cells, and the total mass of cells is called the decidua.As the trophoblast cells invade the decidua, digesting and imbibing it, the stored nutrients in the decidua are used by the embryo for growth and development. During the first week after implantation, this is the only means by which the embryo can obtain nutrients; the embryo continues to obtain at least some of its nutrition in this way for up to 8 weeks, although the placenta also begins to provide nutrition after about the 16th day beyond fertilization (a little more than 1 week after implantation). Figure 82-4 shows this trophoblastic period of nutrition, which gradually gives way to placental nutrition.
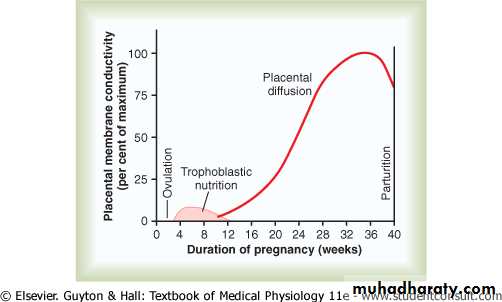
Figure 82-4 Nutrition of the fetus. Most of the early nutrition is due to trophoblastic digestion and absorption of nutrients from the endometrial decidua, and essentially all the later nutrition results from diffusion through the placental membrane.
Function of the Placenta
Developmental and Physiologic Anatomy of the PlacentaWhile the trophoblastic cords from the blastocyst are attaching to the uterus, blood capillaries grow into the cords from the vascular system of the newly forming embryo. By the 16th day after fertilization, blood also begins to be pumped by the heart of the embryo itself. Simultaneously, blood sinuses supplied with blood from the mother develop around the outsides of the trophoblastic cords. The trophoblast cells send out more and more projections, which become placental villi into which fetal capillaries grow. Thus, the villi, carrying fetal blood, are surrounded by sinuses that contain maternal blood.
The final structure of the placenta is shown in Figure 82-5. Note that the fetus's blood flows through two umbilical arteries, then into the capillaries of the villi, and finally back through a single umbilical vein into the fetus. At the same time, the mother's blood flows from her uterine arteries into large maternal sinuses that surround the villi and then back into the uterine veins of the mother. The lower part of Figure 82-5 shows the relation between the fetal blood of each fetal placental villus and the blood of the mother surrounding the outsides of the villus in the fully developed placenta.
The total surface area of all the villi of the mature placenta is only a few square meters-many times less than the area of the pulmonary membrane in the lungs. Nevertheless, nutrients and other substances pass through this placental membrane mainly by diffusion in much the same manner that diffusion occurs through the alveolar membranes of the lungs and the capillary membranes elsewhere in the body.
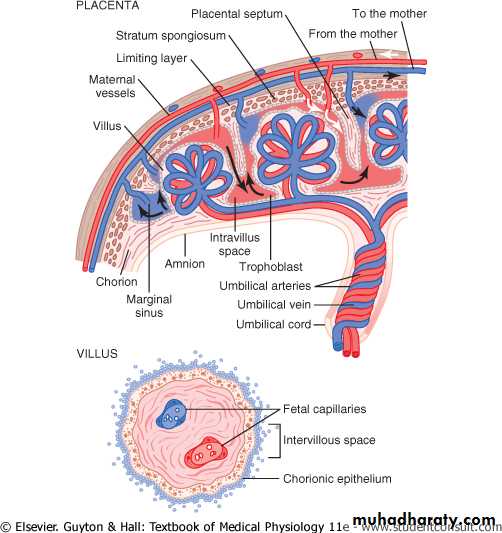
Figure 82-5 Above, Organization of the mature placenta. Below, Relation of the fetal blood in the villus capillaries to the mother's blood in the intervillous spaces.