بسم الله الرحمن الرحيم
Fractures of the femoral neck
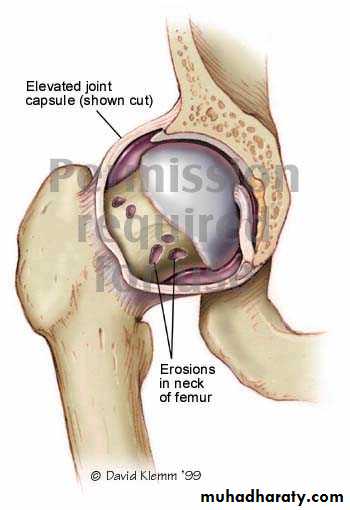
INTRA CAPSULAR FRACTUREfracture neck femur
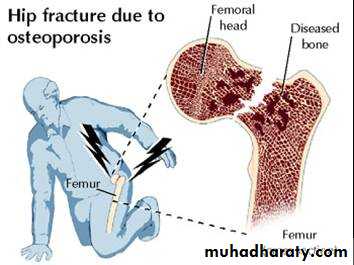
The femoral neck is the commonest site of fractures in the elderly.Mostly occur in women between 70-80 decades.

Risk factors
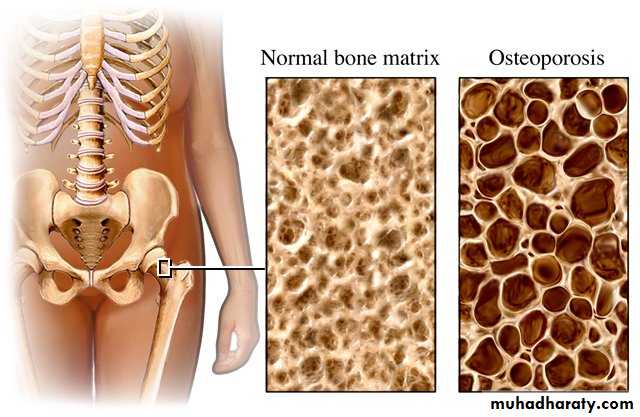
1.Osteoporosis osteomalacia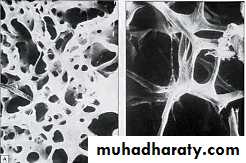
2.Diabetes
3.Stroke

4.Alcoholism
5.Chronic debilitating disease .
6.Weak muscle and poor balance in old people. parkinsonism)Mechanism of injure
In elderlyDirectly Fall on greater trochanter.
Indirectly. Less force with catching toes in carpet with external rotation of the lower limb.In younger individual fall from height or car accident (more sever force).
Pathological anatomy and classificationThe most useful is that of garden which is based on amount of displacement apparent in the pre-reduction x-ray of the neck femur.


Stage 1
impacted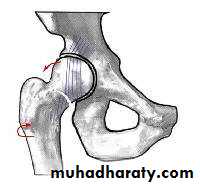

Stage 2
complete fracture Undisplaced
Stage 3
complete with moderate displacement.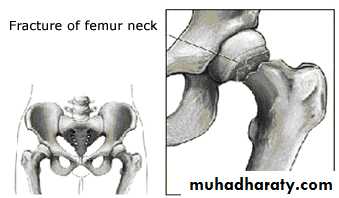
Stage 4
severely displaced fracture.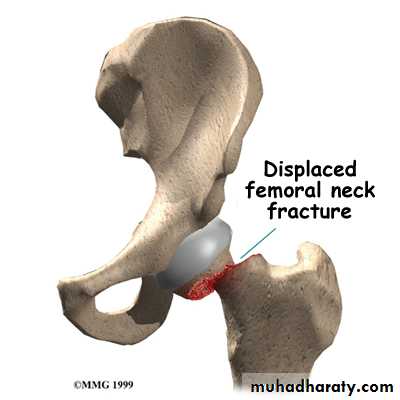
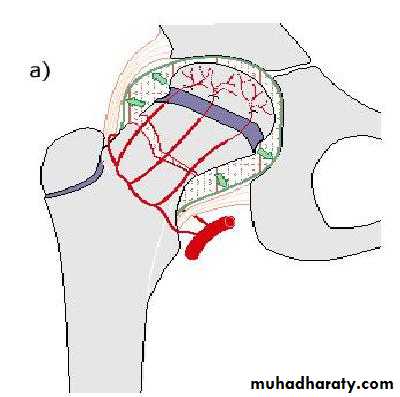
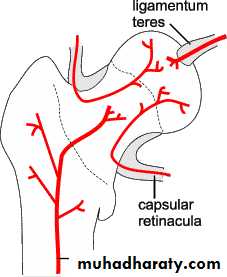
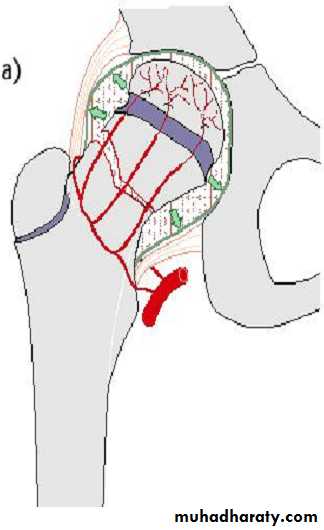
Fracture neck femur has poor capacity for healing
Why???
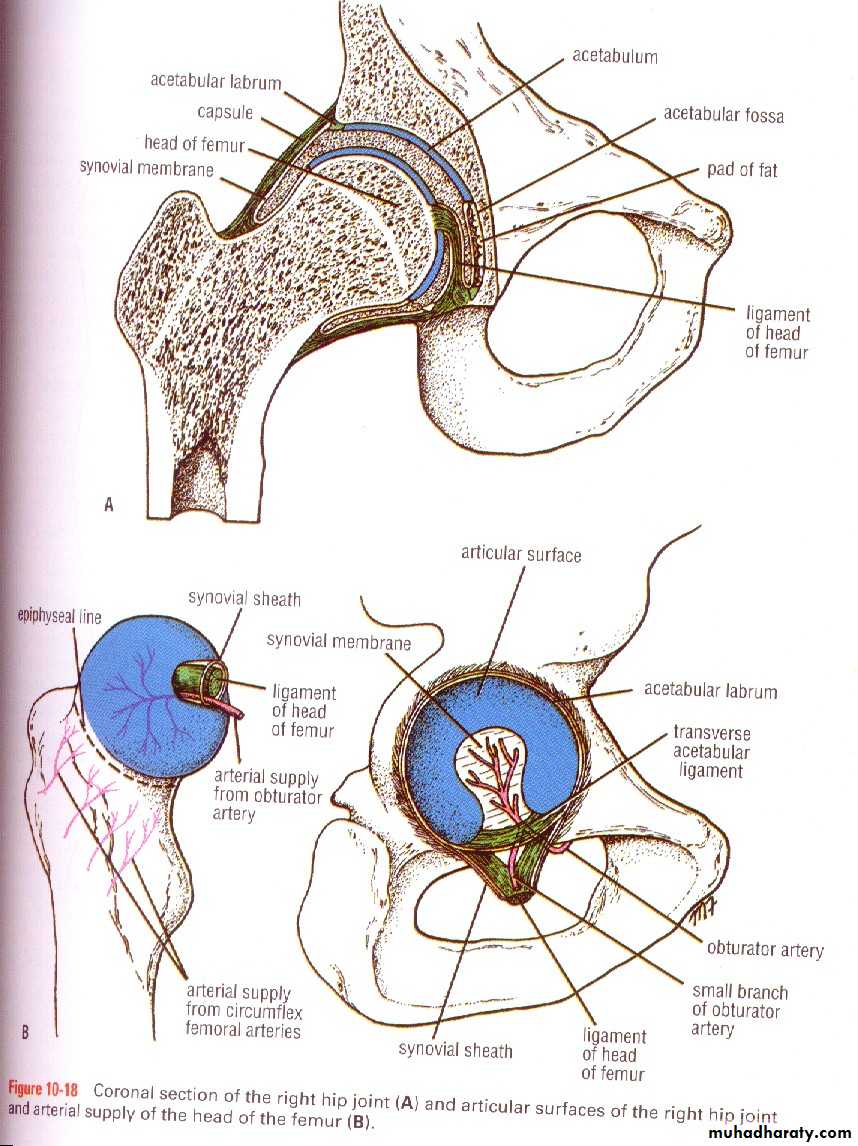
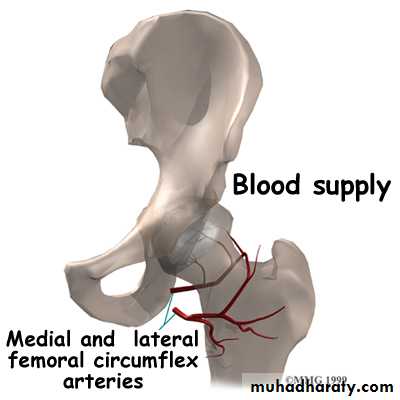
Tearing the capsule vessels.
Intra-articular bone has flimsy periostumNo contact with soft tissue.
Synovial fluid wash.
Clinically:
History of fallen on the ground.Pain in the hip.
O\E
Limb lies laterally rotation and looks ,Short (displaced fracture).
In impacted patient might walk.

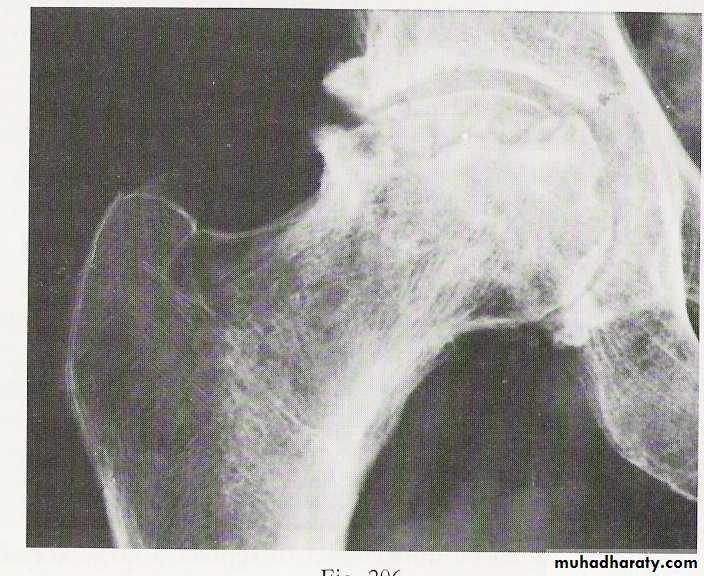
Radiological examination
two questions must be answered.Is there a fracture?
Is it displaced ?:Radiological classification
GRADE 1
:the femoral head is in its normal position or tilted into valgus and impacted on the femoral stump.GRADE 2
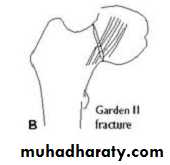
The femoral head is normally placed and the fracture line may be difficult to diagnosed

GRADE 3
The femoral head tilted out of position and the trabecular marking are not in line with those of innominate bone.
GRADE 4
The femoral head trabeculae are normally aligned with those of innominate bone.
D.D:Stress fracture.
Undisplaced fracture.
Painless fracture.
Multiple fractures as with femoral fracture may have neck fracture and missed.
Treatment:
Surgery mandatory to overcome complications.Initial treatment
1.General measure as pain killer.2.Temporary limb splintage ( skin traction).

Full investigation
Chest x rayECG.
F B S.
B urea.
Blood group
Blood preparation for
transfusion.
Screw.
3.Treatment depend on the type and age of the patient
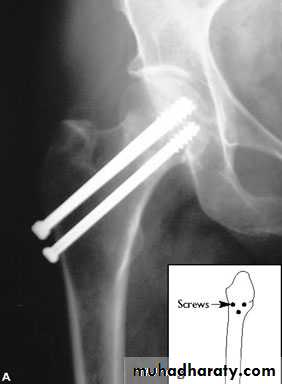
YOUNGER.


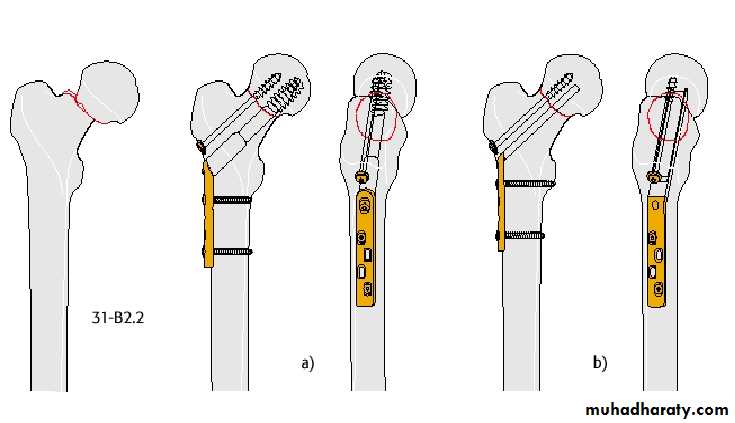
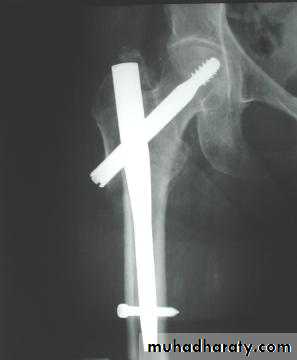
4.DHS.

ELDERLY PEOPLE
5.Austen Moore.
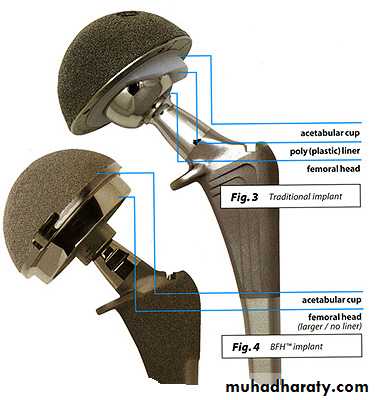
6.Total hip replacement.

Complications:
GeneralDVT


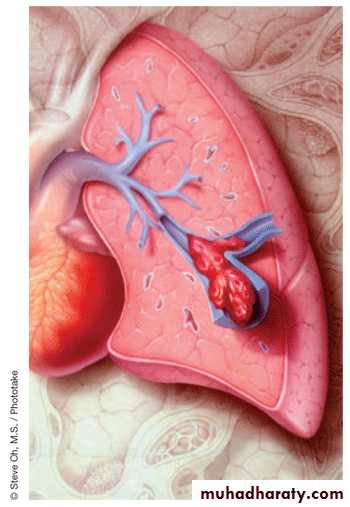
Pulmonary embolism.
Pneumonia.

Bed sore.


Local:
A.N. 30% in displaced fracture, 10% in Undisplaced fracture.Non union
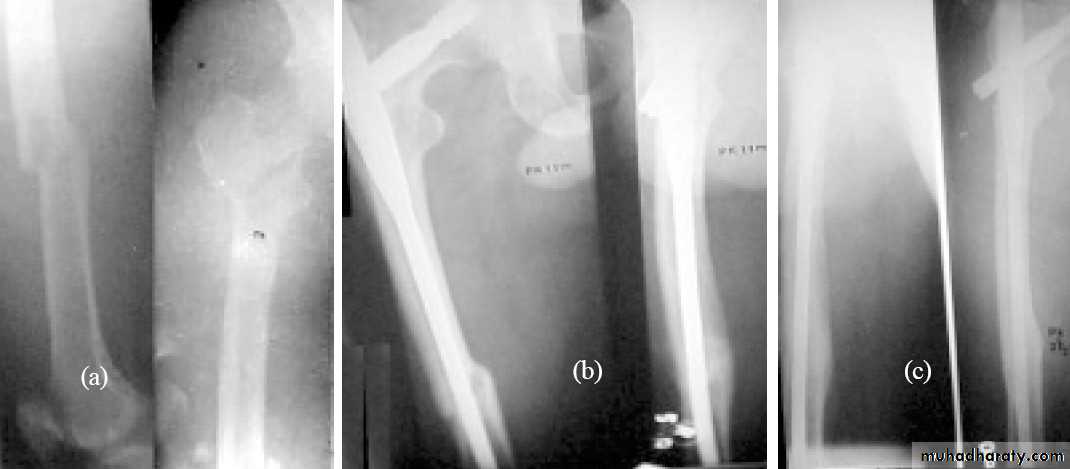
> 30% femoral fracture fails to unite particularly those with sever displacement. .
Osteoarthritis ,a vascular necrosis or femoral head collapse may lead after several years to secondary osteoarthritis.
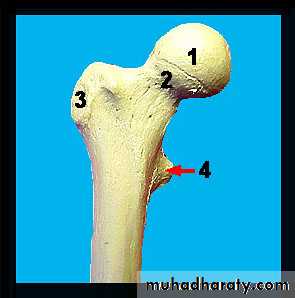
Inter-trochanteric fractures (extracapsular fracture)
.It is extra capsular fracture occurs in elderly..Unite quite easily and seldom cause a vascular necrosis.
Mechanism of injury:
Directly on trochanter.Twisting force indirectly.
The crack runs up between the lesser and greater trochanter.
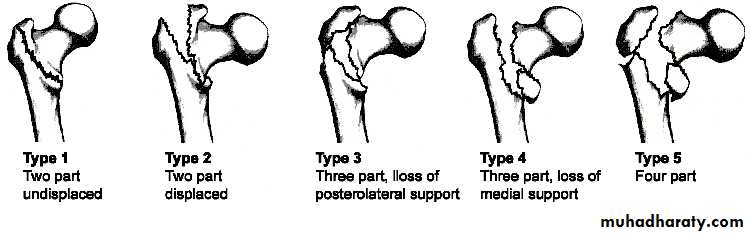
Pathological anatomy divided into:
Stable: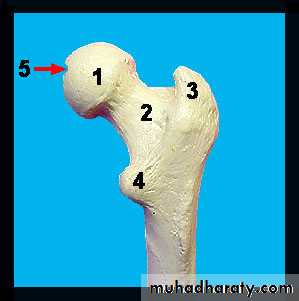
Unstable are those where
a. posteriomedial cortex is shattered.b. poor contact between fracture segment.
Clinically:
Old and unfitHistory of trauma .
Unable to stand with pain.
EXAMINATION
The leg is shorter and more externally rotated than intracapsular fracture.
Ecchymosis


Radiological examination
2 typesStable.

Unstable.


Treatment:
Same previous principle almost always treated by early internal fixation.(to overcome) the possible complications associated with prolonged recumbency.
To get the patient up and walking as soon as possible.
1.Sliding nail
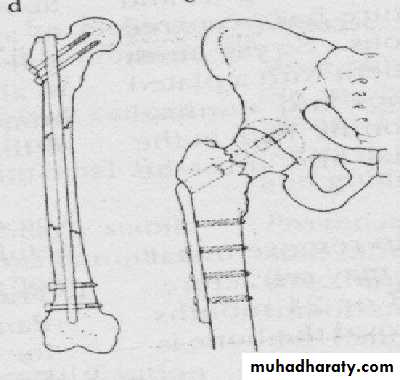

2.L-plate

3.External fixation


Gamma nail
Postoperative exercise is started as early as possible on the
( day after operation ).Patient is allowed up and partial weight bearing as soon as possible.
PHYSIOTHERAPY


Complications:
Early:
general complications.
Late:
1.failed fixation.2.malunion.
3.rarely nonunion.
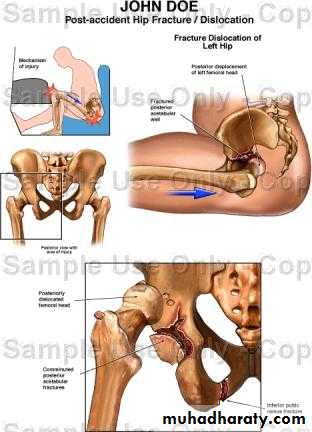
HIP DISLOCATION

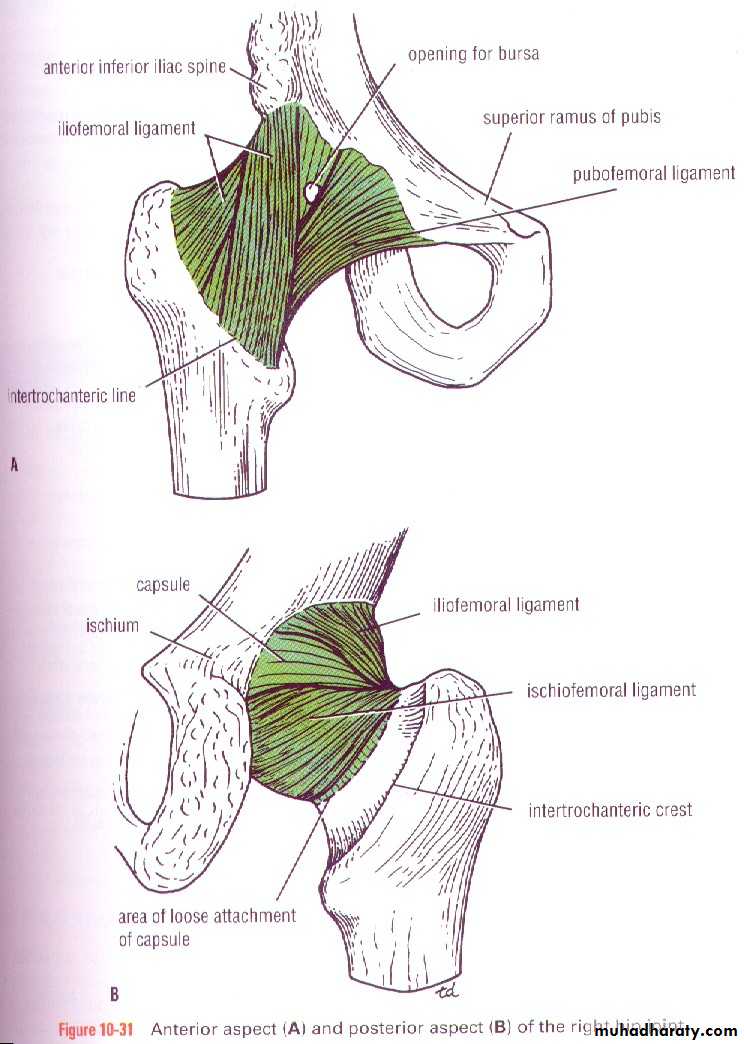
anatomy
Injuries of the hip and femurThe magnitude of force needed to dislocate the hip joint particularly well-contained by virtue of its bony and soft-tissue anatomy.
is so great that the dislocation is often associated with fractures - either around the joint or elsewhere in the same limb.
Hip dislocations are classified according to
the direction
of the femoral head displacement:
Traumatic Dislocations of the hip.
Posterior.Anterior.
Central.
Posterior dislocation:
Mechanism of injure:4 out of 5 traumatic hip dislocations are posterior.
Usually occur in road traffic accident when the knee striking the dashboard
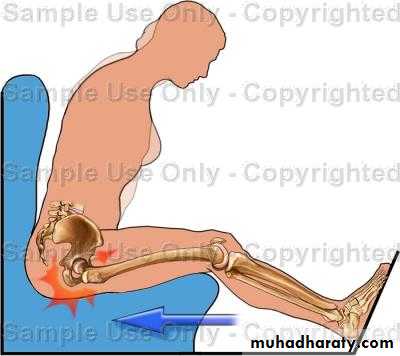
the femoral head is forced out of its socket sometimes associated with fracture.

Clinically:
In a straight forward case the diagnosis is easy.O\E
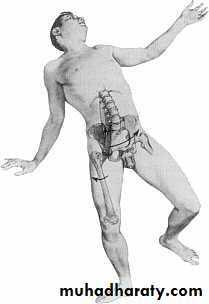
Leg is short, internally rotated, adducted ,
and slightly flexed hip.


Some times fracture femur associated with, and clinically missed.
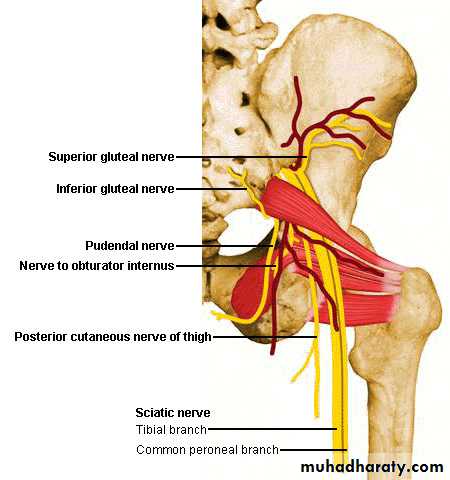
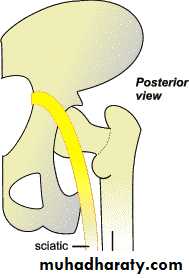
Sciatic nerve examination distally is important.

The golden role is to x ray the pelvis in every case of sever injure
and with femoral fracture to include both the hip and knee.Radiological examinations
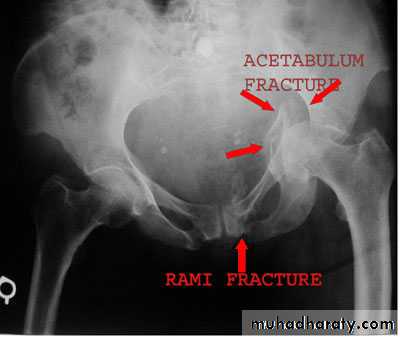
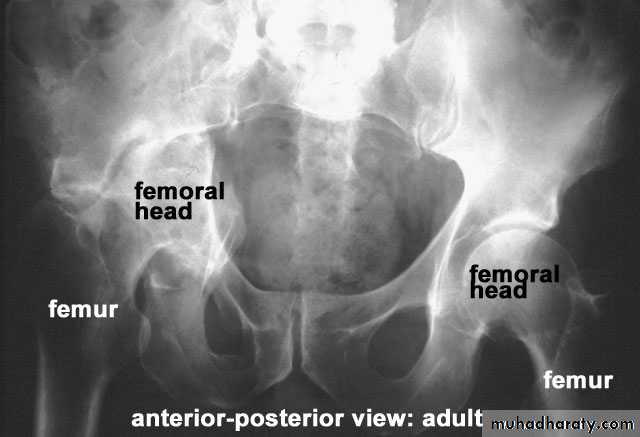
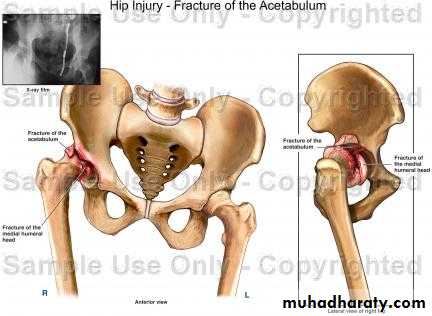
X-R AP view we can see the dislocation with or without associated fracture posterior wall of the acetabulum,or fracture head of the femur,
And neck of femur.

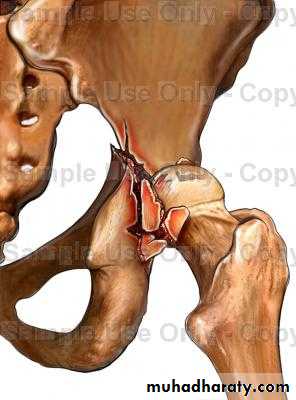



CT scan
is the best way of demonstrating acetabuluar fracture or any bony fragment.
The dislocation must be reduced as soon as possible under general anesthesia. In the vast majority of cases this is done with closed reduction
Treatment:
U\A on the ground.Pelvic support.
In line of the lower limb traction.
Then gradually flexion of the patients hip and knee in 90 degree.
At 90 hip flexion traction is increased and some times little rotation is increased (both internal and external) to accomplish reduction.
Satisfying clunk terminate the procedure.


Skin traction 3-6 weeks.
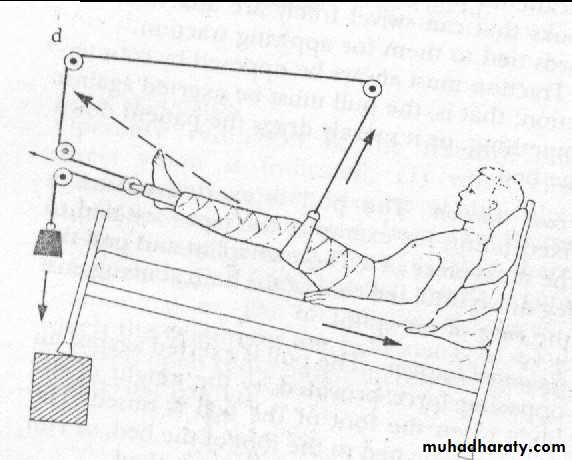
Physiotherapy during and after that.
In complicated dislocation
(surgeryis indicated) .

Complications:
Early.Sciatic nerve injures when there is fracture lead to foot drop in 10%.
So nerve function must be tested and documented before reduction.
Vascular injure
mainly for the superior gluteal artery.Associated fractured femoral shaft.
So as a rule the buttock and the greater trochanter should be palpated.Late:
A vascular necrosis
By x ray appeared between 6weeks- 2 years.
It occur in 10% and raised to 40% if neglected more than 12 hours

Myositis ossificans.


Osteoarthritis due to fracture acetabulum or femoral head, or a vascular necrosis
Traumatic anterior hip dislocation:Mechanism :
Road traffic accident ,miner, building laborer who is leg wide .
knees straight .
Back bent forward.
Clinically:
O\ELeg external rotation.
Abducted and slightly flexed.
Bulging head seen laterally and also feel.
Hip movement impossible.
Neurovascular examination necessary.
Radiological examination:
Hip dislocated either superior, inferior in relation to the acetabulum.
Treatment:
Same principle as posteriorWhile traction of the leg keeping adducted till reduced.

Central fracture -dislocation