


Benign and Malignant cysts and tumors of the ovary
Dr . Hayder Al Shamma’aobjectives
Refer to your previous knowledge regarding anatomy and embryology of the ovariesrecognize the epidemiology, risk actors and etiology of ovarian cancer
Become familiar with the types of ovarian tumors
Appreciate the danger of ovarian tumors
Understand the effect of hormonally active ovarian tumors
Be able to differentiate ovarian mass from other abdominal and pelvic masses
Able to diagnose the possible complications of ovarian mass
recognize the symptoms and signs suggesting malignant ovarian tumors
Know the principles of treatment, surgery, chemotherapy, radiotherapy
Be able to diagnose ovarian mass early and referral of suspicious cases for further evaluation
Introduction
The ovaries give rise to a wide varieties of tumors and cysts more than any organ in the bodyThis gives number of problems regarding classification, diagnosis and treatment
The picture is more confused by the occurrence of functional and physiological cysts ( difficult to differentiate them from neoplastic cysts
Ovarian cysts and tumors can affect all age groups
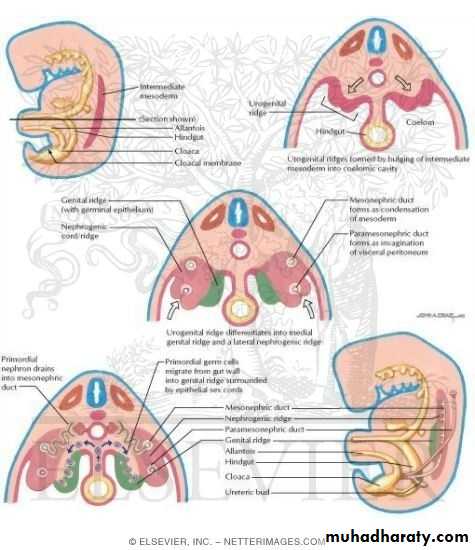
They are often asymptomatic even the malignant tumors (danger of delay diagnosis)Embryology of the ovaries
Classification of ovarian tumors
Many types of classificationsAccording to histopathology
**Can determine prognosis**Type of chemotherapy
**Method of treatment
WHO Classification
1 - Epithelial tumors 75%
a) serous (benign , borderline , malignant )
b) mucinous
c ) endometrioid
d) clear cell
e) Brenner
f) mixed
g) unclassified
2- Sex cord tumors 5-10%
a) granulosa stromal cell tumori- granulosa
ii- thecoma
iii- fibroma
b) androblastoma (Sertoli – Leydig )
c) gynandroblastoma (Sertoli – granulosa)
3-Germ cell tumors 15-20%
a) teratomab) dysgerminoma
c) choriocarcinoma
d) endodermal sinus tumor
e) embryonal carcinoma
f) polyembryoma
g) mixed
4- metastatic tumors 5%
a) Krukenberg tumor
b) lymphoma
5- Others
Serov classificationI : Epithelial
II: Sex cord
III: Lipid cell
IV: Germ cellV: GonadoblastomaVI: Soft tissue tumors non specific to ovaries
VII: Unclassified VIII: Secondary ovarian tumors
IX : Tumor like conditions
Tumor like conditions
• Follicular cyst• Corpus luteum cyst
• Theca-lutein cyst
• Polycystic disease
• Endometriomatous cyst
• Inflamatory
• others
Epithelial tumors serous tumors
40% of all tumors are serous
Benign (serous cystadenoma)
Moderate size single Lucullus smooth outline, lining may contain papilliferous processes , contain clear serous fluid , 50% bilateral
Histopathology:- epithelial lining of single colomnar or cuboidal with cilia ( like Fallopian tube)
Malignant (serous cystadenocarcinoma)
It is the most common type of ovarian cancerMay be cystic or solid or combination (solid with cystic component)
Lined by fine papilliferous processes which may perforate the cyst wall and spread to peritoneal cavity, tubes, uterus
Calcium deposition may occur psammoma bodies
50% bilateral
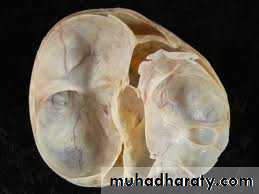
Mucinous cystadenoma
Unilateral ,multilocular cystIt may reach enormous size
Smooth outline
Filled with jelly like mucin
Lined by tall columnar cells with dark nuclei similar to cervical glands
5-10% tendency for malignant ransformattion
Spontaneous perforation may cause seedling of benign or low malignant cells in the peritoneal cavity causing ascitis of gelatinous fluid (pseudomyxoma peritonei) cusing cachexia and then death usually after several laparotomies
Malignant (mucinous cystadenocarcinoma)
Is relatively chemo and radio resistant
Endometrioid tumor
Usually malignant (benign are rare)Solid cystic tumor often contain hemorrhagic area
Lining is similar to proliferative endometrium with glans
Some time associated with endometrial cancer
Brenner tumor
Unilateral , solid 5-15 cmIt is usually borderline malignant
Histopathology :- transitional epithelial cells imbeded in a fibrous tissue stroma
Germ cell tumors
These are tumors derived from totipotent cells (has the potential to differentiate to all types of tissues) ie, can differentiates to embryonal cell line or extra-embryonal cell line (chorionic cells)a) teratoma
• Mature teratoma (dermoid cyst)
• Benign cystic
It is the commonest ovarian cyst seen in young women
It affect 2nd and 3rd decade of life
20% bilateral
It is a smooth unilocular cyst filled with sebum with a hump of tissue at one side called mammillary process
The hump contain variable types of tissues , bone , teeth, cartilage, skin, sebaceous glands , hair which project inside the cavity
The cyst usually lie in the vesicouerine pouch
It contain tissue of endoderm , mesoderm and ectodermIt may contain thyroid tissue causing thyrotoxicosis called stroma ovarii
b) Immature teratoma
Usually solidUnilateral
Usually malignant ( benign solid teratoma is rare)
Affect 2nd decade of life
b) dysgerminoma
Lobulated solid tumor soft in consistancyYellow creamy color
10 – 20 % bilateral
Highly radio and chemosensitve
Histopathology:- large polyhedral cells contain glycogen
c) Choriocarcinoma (non gestational )
Tumor consist of trophoblastic tissue
Secret hCG
Sex cord tumors
a) granulosa cell tumorOccur at any age
Unilateral lobulated solid or partly cystic yellow color
Low grade malignancy (borderline malignant)
Histology:-granulosa cells which sometimes form micro-follicles called Call – Exner bodies
Usually secret estrogen
Rarely secret testosterone
b) theca cell tumor
Firm yellow tumorUsually benign
Usually secret estrogen rarely androgens
C) fibroma
Benign tumor lobulated solid hard white massHighly mobile
Benign tumor
Associated with ascitis and some time pleural effusion
Meig’s syndrome
d) androblastoma
Sertoli and Leidig cells
Form seminephrous tubules like a testis but without spermatozoa
Secret testosterone
Secondary ovarian tumors
Metastasis from other organs uterus, stomach, colon, breastKrukenberg tumor
Bilateral solid masses of adenocarcinoma with signet ring cells contain mucin which push the nucleus to the periphery of the cell
The tumor may become larger than the primary site
Etiology of ovarian tumors
UnknownEnvironmental
high fat diet
low fiber diet , vit A
talcum powder
caffeine ?
asbestos?
radiation ?
viral infection mumps, rubella, influenza ??
Etiology of ovarian tumors
Hormonal effect
pregnancy, breast feeding, OCCP, are protective against ovarian cancer
nulliparity, drugs for ovulation induction, early menarche , late menopause , are risks for ov. Cancer
Tubal ligation, hysterectomy , protective!
endometriosis increase risks
Etiology of ovarian tumors
• Site specific ovarian cancer (autosomal dominant)• Hereditary breast-ovarian cancer syndrome
• Lynch syndrome II hereditary non polyposis colonic cancer (HNPCC)
Epidemiology
More in industrialized countries35% of genital tract malignancy
More than 50% mortality
Most epithelial cancer in postmenopausal women
The disease usually asymptomatic and at presentation it is usually extended beyond the ovaries and involve adjacent organs
Spread of ovarian tumors
• Local infiltration to near organs by perforating the capsule and gain attachment to the omentum, broad ligament, bowel, uterus, etc….• Transperitonial spread through seedling
• Lymphatic spread to para-aortic lymph nodes to thoracic duct to left supraclavicular
• Hematological spread (uncommon)
staging
Is the determination of the extent of the disease on preoperative clinical exam, investigation . But the final staging is surgical
FIGO staging
• Stage I ( limited to the ovaries )
• Stage II ( pelvic extension )
• Stage III (intraperitonial metastasis )
• Stage IV ( distant metastasis )
Clinical features of ovarian tumors
Age incidence :- with exception of germ cell and sex cord tumors , most ovarian tumor occurs at age 40-60 years.Symptoms of ovarian cysts and tumors
• Asymptomatic:-many ovarian masses discovered accidentally during routine antenatal care or during routine exam at medical or surgical clinics2. Pain:- pain is unusual symptom of uncomplicated neoplasm but it could occur in the following situation
• Metastasis to sacral plexus cause sacral root pain and dull aching back pain
• In cases of complicated cyst ( rupture, hemorrhage, twist, impaction and infection) cause acute abdominal pain (acute abdomen)
3. Abdominal enlargement
4. Pressure symptoms
a) bowel :- indigestion, loss of appetite, vomiting ,constipation
b) bladder:- frequency , retention of urine
c) venous plexus :- varicose veins of the vulva , lower limbs , hemorrhoids
5. Menstrual cycle :-
neither benign nor malignant tumor affect the menstrual cycle and the cycle usually remain regular even in the presence of malignant tumor , …except when the tumor is hormonally active (rare)Tumors secrete estrogen
child → precocious pubertyadult → menstrual irregularity
old → post menopausal bleeding
Tumors secrete androgens
child → heterosexual precocious pubertyadult → defeminization (breast atrophy, amenorrhea ) then → musculinization (deep voice, hirsutism, enlarged clitoris, muscular )
Physical signs of ovarian tumor/cyst
• Small pelvic ovarian tumor:-• Lying in the pelvis , not palpable abdominally and only palpable by vaginal examination
• It felt as a smooth mobile mass behind the uterus and to the side , the uterus can be separated from the mass
• Some time the mass may be felt anterior to the uterus suggest dermoid cyst or torsion
2. Big ovarian tumor:- rise up from the pelvis
To the abdomen, it has a tendency to lie in the midline just under the abdominal wall pushing the bowl up and to the side
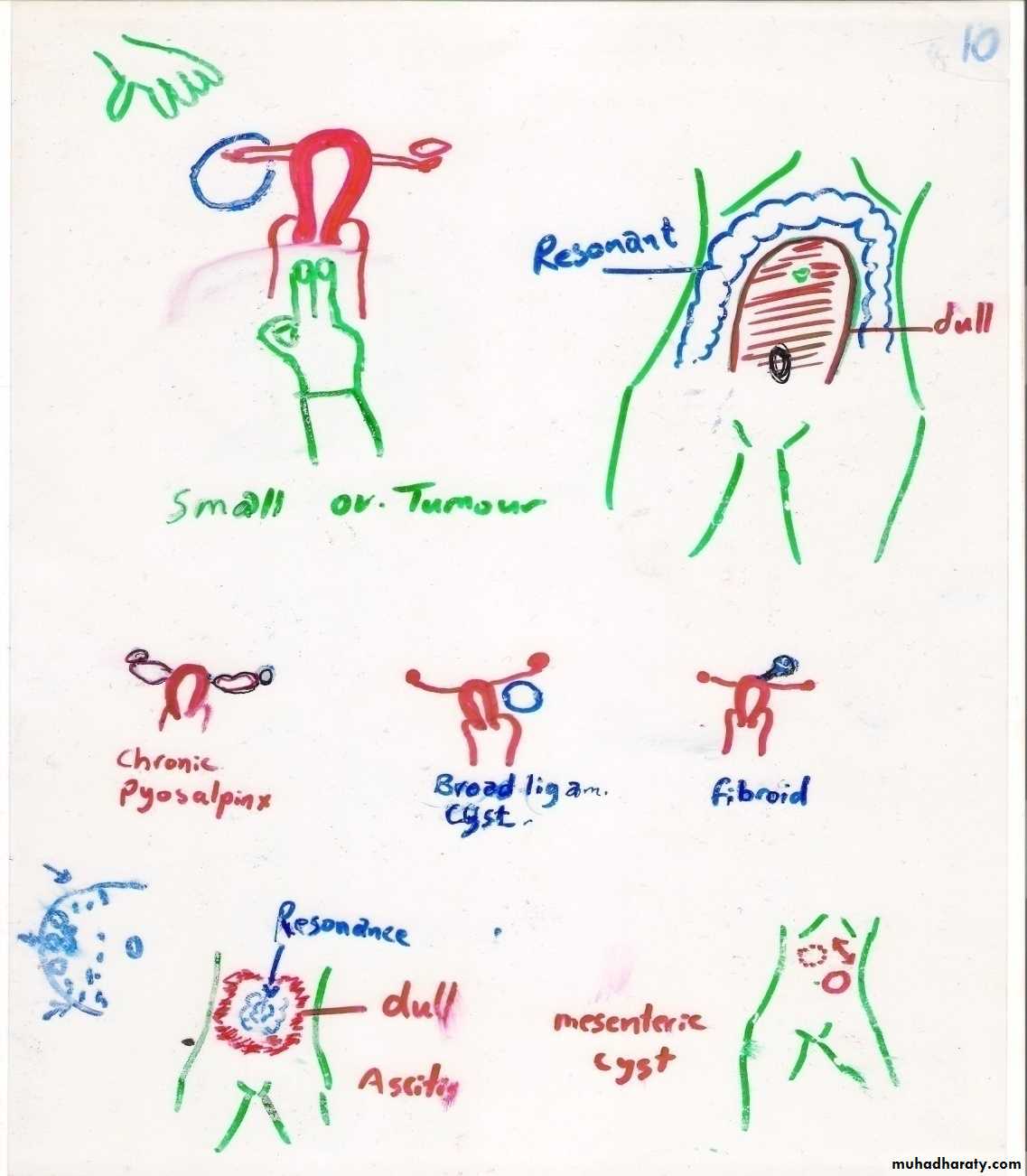
Differential diagnosis of small pelvic ovarian tumor
• tubo-ovarian abscess (bilateral, fixed, pyrexia, painful ).• Broad ligament cyst(unilateral , pushing the uterus to the other side, painless, fixed
• Pedunculated fibroid (difficult to differentiate)
• Chronic ectopic
• Pelvic kidney (posterior fixed mass, ivp is diagnostic )
Differential diagnosis of large ovarian tumor
• Full bladder ( voiding or catheterization → disappear)• Fecal mass ( elongated, indentation, defecation change shape and site)
• Ascitis ( resonant at the center dull at the periphery )
• Fibroid (firm, move with the uterus, if pedunculated difficult to differentiate)
• Pregnancy (central mass, characteristic consistency , fetal parts and fetal heart auscultation )
• Gross obesity ( distended abdomen , no mss can be felt )
• Large hydrosalpinx
• Enlarged spleen
• Flatulence
• Mesenteric cyst (feel whole cyst , move only in one plane perpendicular to the root of mesentery )
Complication of ovarian cyst/tumor
• Torsion:- twist of the cyst with the ovary on its pedicle obstructing venous blood flow causing congestion, hemorrhage inside the cyst , pain, then obstruction of arterial blood causing necrosisOccur in moderate size cyst, when there is no adhesions
Large cysts , presence of adhesions are unlikely to twist
Diagnosis :- colicky abdominal pain intermittent then continuous vomiting, tender adnexial mass
Treatment emergency laparotomy/laparoscopy
• 2.Rupture :- either spontaneous or traumaticSpontaneous in large tumor rapidly growing with necrosis of the wall
Traumatic during pv exam or blow to the abdomen
The symptoms and signs depend on the content of the cyst
If clear non irritant material →no symptoms (only diagnosed when sudden disappearance of cyst on u/s follow up
if irritant as blood or sebum →acute abdomen
Treatment :- laparotomy/laparoscopy
3. Hemorrhage:-may occur inside a cyst causing rapid enlargement and acute abdominal pain
Treatment :- laparotomy/laparoscopy
4. Impaction:- the cyst grow and remain in the pelvis and press on the bladder neck and rectum causing abdominal pain , retention of urine , constipation
Treatment :- laparotomy/laparoscopy
5. Infection :- from nearby structure like appendix, diverticulum, cause pelvic abscess
Treatment:- laparotomy/laparoscopyInvestigation of ovarian cyst/tumor
• Ultrasound +Doppler ( is the main investigation )• 2. radiology:- a) may show calcifications, teeth,
• b) CXR preoperative investigation
• c) IVP
• d) CT scan MRI
• 3. Paracentesis cytology of ascitis (do not puncture the cyst)
• 4. OGD , colonoscopy
• 5. Tumor markers ( CA125 for ep. Cancer and hCG, CEA , AFP, for germ cell tumors)
Clinical features suggesting malignancy
• Age :- childhood tumors are usually malignant, in adults chance of malignancy increase with increasing age• Pain :- dull aching pain and sacral root pain suggest malignancy
• Rapid growth
• Solid or solid/cystic
• Bilateral
• Ascitis
• Leg edema
• Fixation
• Vulvar varices
• Metastasis *** indicates malignancy
Treatment of ovarian cyst/tumor
Determine whether functional or neoplastic , and if neoplastic whether benign or malignant
Calculate the Risk of Malignancy Index ( RMI )
By measure CA 125 u/ml x US score x menopausal score
US score = (0 ,1, 3 )
for each of the following feature , one point
multilocular, bilateral, solid area, metastasis, ascitis
(0 for no US score, 1 for one US finding , 3 for 2 or more points)
Premenopause 1 , postmenopause 3
Example :- 25 years old , bilateral simple ovarian cyst, CA 125 = 20 u/ml
RMI = 20 x 1 x 1 = 20 → low risk ( cutoff value 200 )Example 55 years , solid bilateral tumor , CA 125 = 90 u/ml
RMI = 90 x 3 x 3 = 810 high risk malignancyTreatment of functional cyst
Functional cyst in asymptomatic woman ,(unilateral, simple cyst, thin wall, no ascitis less than 7 cm ) follow up for 6 weeksFunctional cyst will disappear
Treatment of ovarian neoplasm
Mainly surgicalLaparoscopy for benign ( low risk )
Laparotomy for malignant (high risk )
Treatment of benign ovarian cyst
Below age of 45 years
treated by cystectomy for small cyst
oopherectomy for large cysts
Above age 45 years
TAH + BSO
Treatment of malignant ovarian tumor
Staging +treatmentStage I and II
TAH + BSO + omentectomy + para aortic lymphadenectomy + biopsy from diaphragm
For stage III and IV surgical staging + cytoreduction + chemo/radio therapy
Terminal careAscitis :- repeated aspiration, some times local chemotherapy
Intestinal obstruction:- subacute obstruction treated conservatively , surgical treatment indicated if the disease limited to a small segment of the bowel
Pain :- pain relief is an essential part of care and it is the least thing to do to the patient
Tumor like conditions
• Follicular cyst :- very commonWhen small not regarded as abnormal
Thin walled cyst lined by granulosa cells
Contain clear fluid
Rarely exceeds 5 cm
Asymptomatic secret estrogen
May cause endometrial hyperplasia
Occur when Graafian folicle not ovulate
Corpus luteum cyst:-
Bleeding inside corpus luteum
Increase it’s life span
Secret progesterone
Delay menstruation
Some time painful
Misdiagnosed as ectopic
Theca lutein – graulosa lutein cysts
BilateralOccur when excessive stimulation of the ovaries by gonadotrophins
From H- mole secret hCG
From Clomiphene treatment or FSH
Disappear when gonadotrophins stoped
Ovarian tumors in pregnancy
Occur in 1/1000 pregnancy5% malignant
10% functional
85% benign , dermoid and cystadenoma
Management
Malignant → treat irrespective to pregnancy
Benign → treat in 2nd trimester