Gynaecology
Dr. Nadjma
Lec 25 - Endometriosis
DR. NADGMA - LEC 3

Endometriosis
Definition
Endometriosis is defined as the presence of endometrial surface
epithelium &/ or endometrial glands & stroma outside the uterine
cavity.
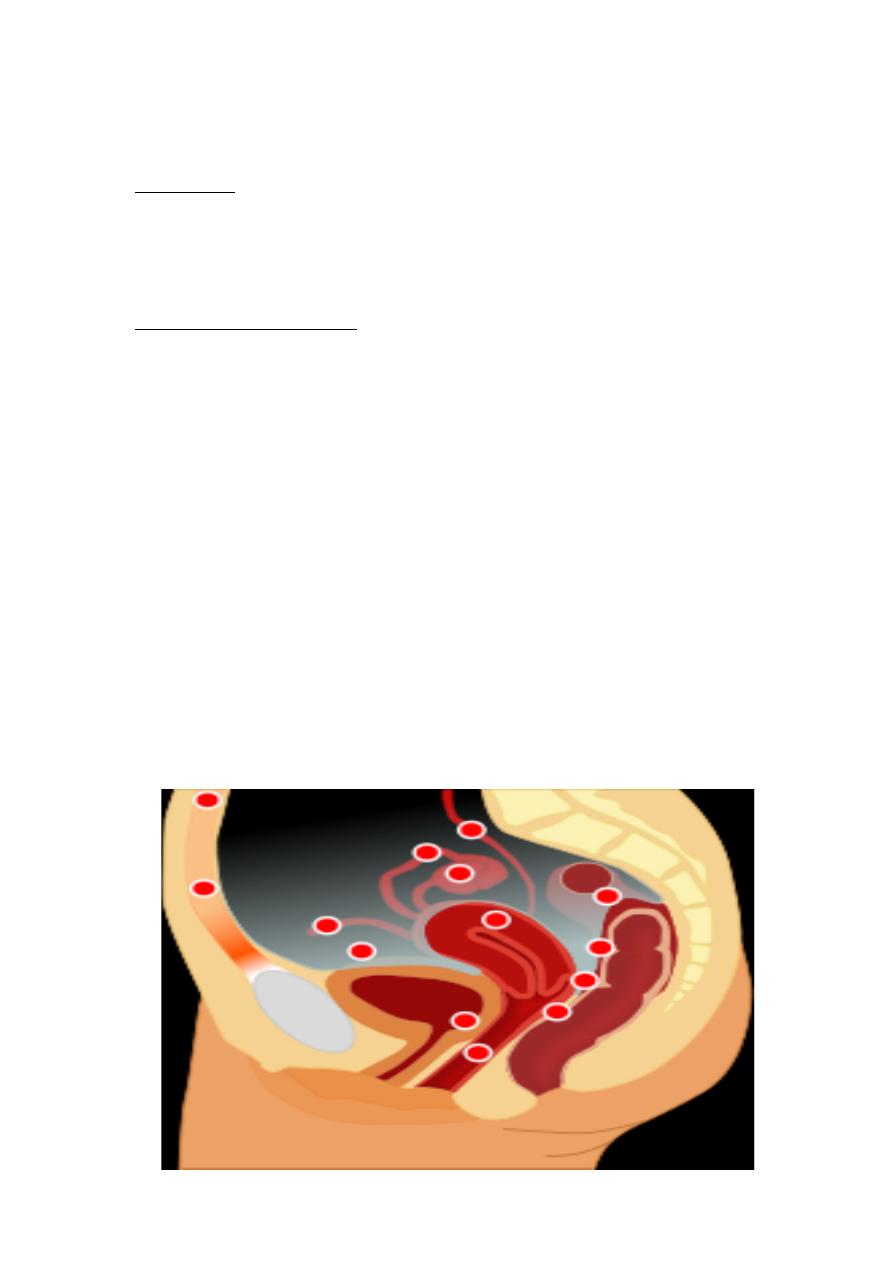
Sites of endometriosis
v
Ovaries
,
called
endometrioma or chocolate cyst
v
Fallopian tubes
v
The back of the uterus
v
Within the myometrium
& is called adenomyosis
v
broad ligament
v
Pelvic peritoneum
v
Intestines, most commonly the rectosigmoid
v
Urinary bladder and ureters.
v
Vulva and vagina
v
Lung
v
Abdominal scars
Etiology &Pathogenesis
1. The implantation theory & menstrual regurgitation.
2. Coelomic metaplasia theory.
3. Lymphatic & vascular dissemination.
4. Genetic & immunological factors.
Pathogenesis
Peritoneal endometriosis
1. Red endometriosis.
2. Black endometriosis.
3. White endometriosis (fibrosed).
Ovarian endometriosis
Endometrioma ( choclate cyst)
Rectovaginal endometriosis
Clinical features
1) Asymptomatic.
2) Pelvic pain: chronic pelvic pain, congestive dysmenorrhea, deep
dyspareunia ( painful intercourse), dysuria, urinary urgency and
frequency, and sometimes painful voiding and dyschezia (difficulty
in defecation).
3) Infertility.
4) Features of acute abdomen due to rupture or torsion of
endometrioma.
5) Menorrhagia & irregular menses.
6) Abdominal & pelvic mass.
7) Cyclic heamaturia , cyclic rectal bleeding.
8) Cyclical pain & bleeding from umbilicus or surgical scars.
9) Cyclical heamoptysis & hemopneumothorax if involve the lungs.
10) On examination, there is fixed retroverted uterus with hard,
tender nodules or adenxial mass of endometrioma.

Investigations
1. Laparoscopy: it remains the gold standard means of diagnosis. It
may demonstrate:
• white thickened scar of endometriosis
• fixed RV uterus
• burn match stick appearance
• adhesion
• chocolate cyst in the ovaries
• heamatosalpinx
• it allows to take a biopsy from the lesion & gives a benefit
to determine the extent and staging of the disease. Also it
allows concurrent therapy at the time of laparoscopy in the
form of cautery or laser treatment in selected cases.
2. USS: helps in the diagnosis of endometrioma.
3. Ca125 level: this is a glycoprotein expressed by some epithelial
cells of coelomic origin, it increases in cases of endometriosis.
4. MRI: this can detect endometriosis in ovaries, bladder, bowel &
rectovaginal septum.
Endometriosis & Infertility
30 – 40% of patients with endometriosis have infertility & about
15% of pt with infertility have endometriosis. Mechanism by which
endometriosis cause infertility are :
1. Ovarian function: (causes anovulation, luteinized unruptured
follicle)
2. Tubal function: (causes adhesions which are further complicated
by kinking or obstruction of the tubes)
3. Coital function: (causes dyspareunia and thus decrease frequency
of intercourse)
4. Sperm function: (Increase macrophage that engulf sperms)
5. Early pregnancy failure: (because the uterus is retroverted. when
enlarged may also result in incarcerated uterus)
6. Adhesions
# The pervious sentences between brackets are added by a student
Treatment
o
Medical treatment
a) Combined oral contraceptive pills (used continuously for 6
- 9 months)
b) (Androgen derivatives ) Danazole & gestrinone.
c) Progestogens (used for 6 - 9 months).
d) LHRH analogues (zoladex or decapeptyl subcutaneous or
intramuscular injection given every 28 days for up to 6
months because of risk of osteoporosis) .
e) NSAID.
# sentences between brackets are added by a student
o Surgical treatment
a) Conservative surgery by using laparoscopy.
b) Radical surgery by total abdominal hysterectomy &Bilateral
salpingo - oophrectomy in old patients who have completed
their family. Postoperative HRT can be used especially in
young women but it is preferred to be delayed for 6
months or more to minimize the risk of recurrence.
Adenomyosis
Causes:
v
Repeated pregnancies.
v
Vigorous curettage.
v
Endometrial hyperplasia.
Pathology:
The uterus is symmetrically enlarged. The lesion could be
localized or diffused throughout the uterine wall. Cystic space filled with
blood within myometrium is shown on Histopathological examination.
Clinical features:
1)
Menorrhagia
2)
Secondary dysmenorrhea
3)
Pelvic discomfort & dyspareunia
4)
On examination there is a bulky symmetrically enlarged tender
uterus with regular outline.
Diagnosis:
1.
Ultrasound
2.
MRI
3.
Biopsy and HP examination
Treatment
a) Medical treatment: same as endometriosis (danazole, gestrinone,
and GnRH agonist).
b) Surgical treatment: hysterectomy.
