Medicine
Dr. Akram
Neurology
“
Diseases of the Spinal Cord
”
Prof. Akram AI-Mahdawi
LECTURE 12
Diseases of the Spinal Cord Prof. Akram Al-Mahdawi
2
Diseases of the Spinal Cord
- Prof Akram Al-Mahdawi
- CABM, MRCP, FRCP, FACP& FAAN
Objectives
To learn some basic anatomy of spinal cord
To have an idea about symptoms and signs of spinal cord
How would you approach a patient with spinal cord diseases?
Come across a common spinal cord diseases
Upper vs. Lower Motor Neuron
Upper motor neuron lesion (UMNL)
Motor cortex internal capsule brainstem spinal cord
Lower motor neuron lesion (LMNL)
Anterior horn cell nerve root plexus peripheral nerve
neuromuscular junction muscle
Basic Features of Spinal Cord Disease
UMN findings below the lesion
- Hyperreflexia and Babinski’s
Sensory and motor involvement that localizes to a spinal cord level
Bowel and Bladder dysfunction common
Remember that the spinal cord ends at about T12- L1
This box was added by the students for those who don’t know what these
abbreviations mean:
CABM:
Certification of Arab Board of Medical Specialization
MRCP& FRCP: Member and Fellow of the Royal College of Physicians
FACP: Fellow of the American College of Physicians
FAAN: Fellow of the American Academy of Nursing
Diseases of the Spinal Cord Prof. Akram Al-Mahdawi
3
History
Onset
- Acute, subacute and chronic
Symptoms
- Pain
- Weakness
- Sensory
- Autonomic
Past history
Family history
Tempo of Spinal Cord Disease
Etiology
Acute
Subacute
Chronic
Trauma
X
Mass lesion
X
X
Infections
X
X
X
Inherited
X
Vascular
X
X
X
Autoimmune
X
X
Nutritional
X
This box was added by the students and it has been explained by Dr. Akram:
Before continuation you have to understand and review the spinal cord pathways (sensory and
motor): dorsal column& spinothalamic-sensory pathways- and corticospinal -motor pathway.
You can find series of 4 videos explaining these pathways on YouTube under the name of
pathways uploaded by Handwritten Tutorials.
Or you can find a summary page from (First Aid for USMLE step 1 version 2015) uploaded in
(Baghdad college of medicine 5
th
grade Neuromedicine
Prof. Akram Al.Mahdawi diseases of the spinal cord)
Diseases of the Spinal Cord Prof. Akram Al-Mahdawi
4
Motor Exam
Upper cervical
- Quadriplegia with impaired respiration
Lower cervical
- Proximal arm strength preserved
- Hand weakness and leg weakness
Thoracic
- Paraplegia
Note: Tone -- Increased distal to the lesion
Sensory Exam
Establish a sensory level
- Dermatomes
Nipples: T4-5
Umbilicus: T8-9
Posterior columns
- Vibration
- Joint position sense (proprioception)
Spinothalamic tracts
- Pain
- Temperature
Autonomic disturbances
Neurogenic bladder
- Urgency, incontinence and retention
Bowel dysfunction
- Constipation more frequent than incontinence
With a high cord lesion, loss of blood pressure control
Alteration in sweating
Diseases of the Spinal Cord Prof. Akram Al-Mahdawi
5
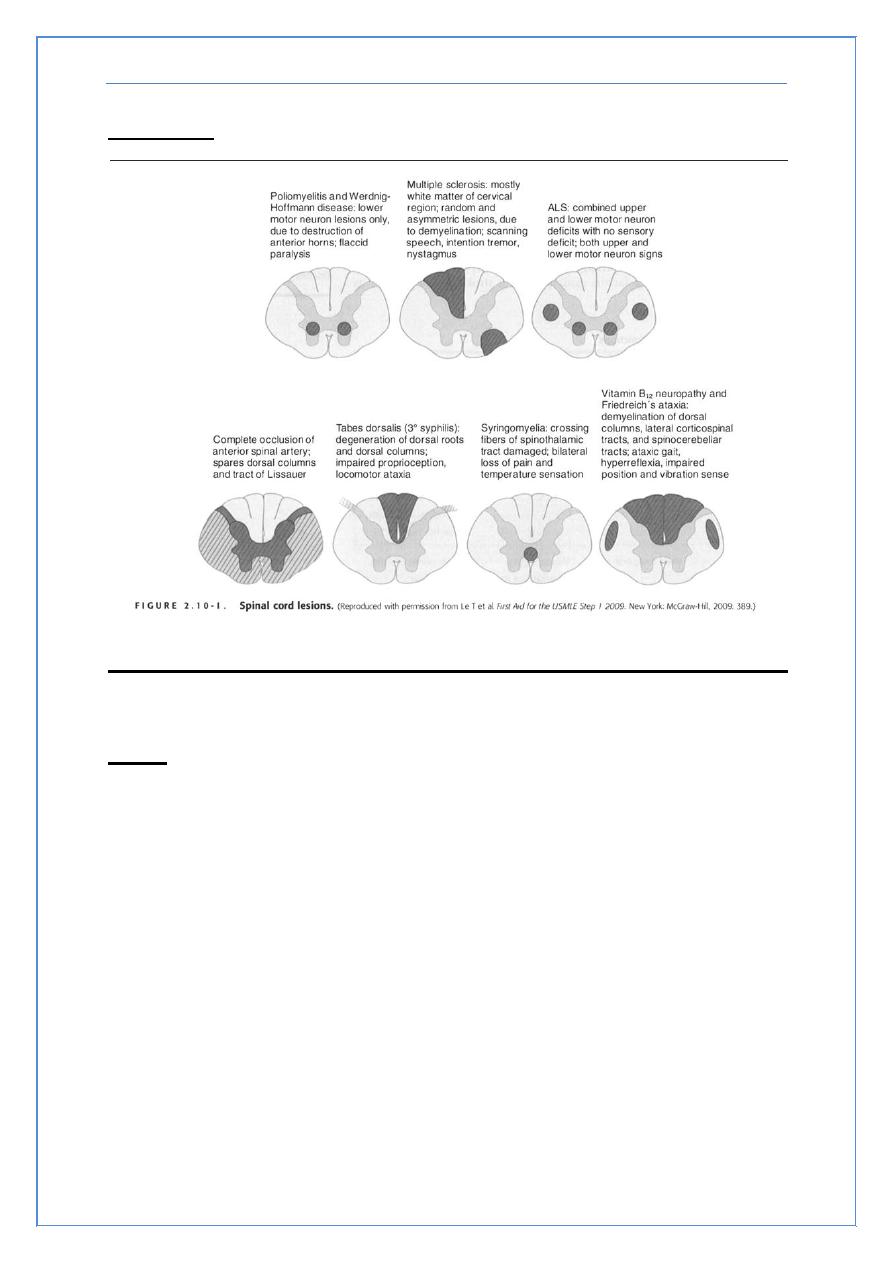
The picture below was added by the students it is not included in the lecture:
Classical spinal cord syndromes
Anterior spinal artery infarct
Brown Sequard syndrome
Syringomyelia
Conus medullaris/caude equina lesions
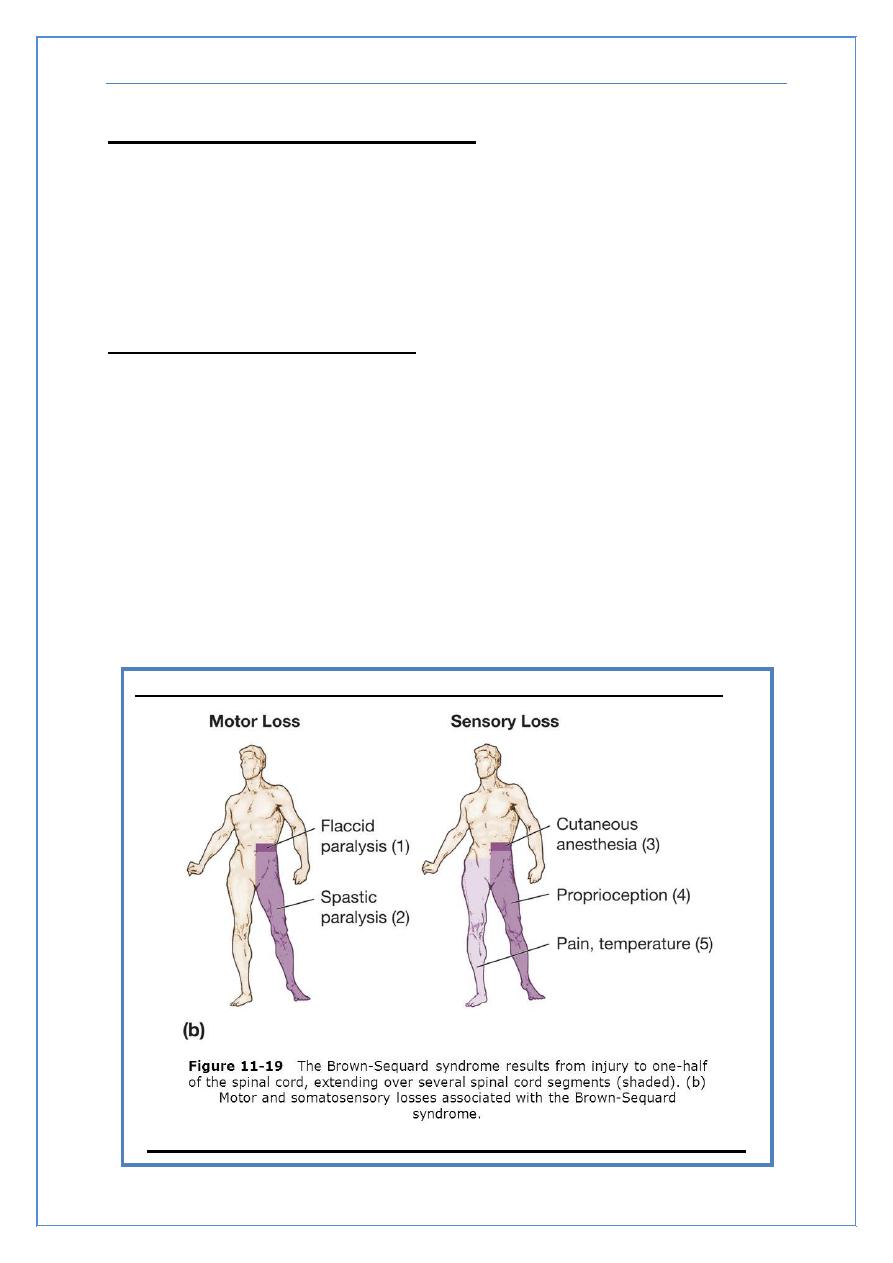
Brown Sequard Syndrome
Cord hemisection
Trauma or tumor
Dissociated sensory loss
- Loss of pain and temperature contralateral to lesion, one or 2
levels below
crossing of spinothalamic tracts 1-2 segments above where they
enter
- Loss of vibration/proprioception ipsilateral to the lesion
these pathways cross at the level of the brainstem
Weakness and UMN findings ipsilateral to lesion
Diseases of the Spinal Cord Prof. Akram Al-Mahdawi
6
Syringomyelia
Fluid filled cavitation in the center of the cord
Cervical cord most common site
- Loss of pain and temperature related to the crossing fibers occurs
early ((cape like sensory loss))
- Weakness of muscles in arms with atrophy and hyporeflexia.
- Ater – corticospinal tract involvement with brisk reflexes in the
legs, spasticity, and weakness
May occur as a late sequelae to trauma
Can see in association with Arnold Chiari malformation
Conus Medullaris vs. Cauda Equina Lesion
Finding
Conus Medullaris
Cauda Equina
Motor
Symmetric
Asymmetric
Sensory loss
Saddle
Saddle
Pain
Uncommon
Common
Reflexes
Increased
Decreased
Bowel/bladder
Common
Uncommon
Investigation of Spinal Cord Disease
Radiographic exams
- Plain films
- Myelography
- CT scan with myelography
- MRI
Spinal tap
- If you suspect: inflammation, MS and rupture of a vascular
malformation.
Diseases of the Spinal Cord Prof. Akram Al-Mahdawi
7
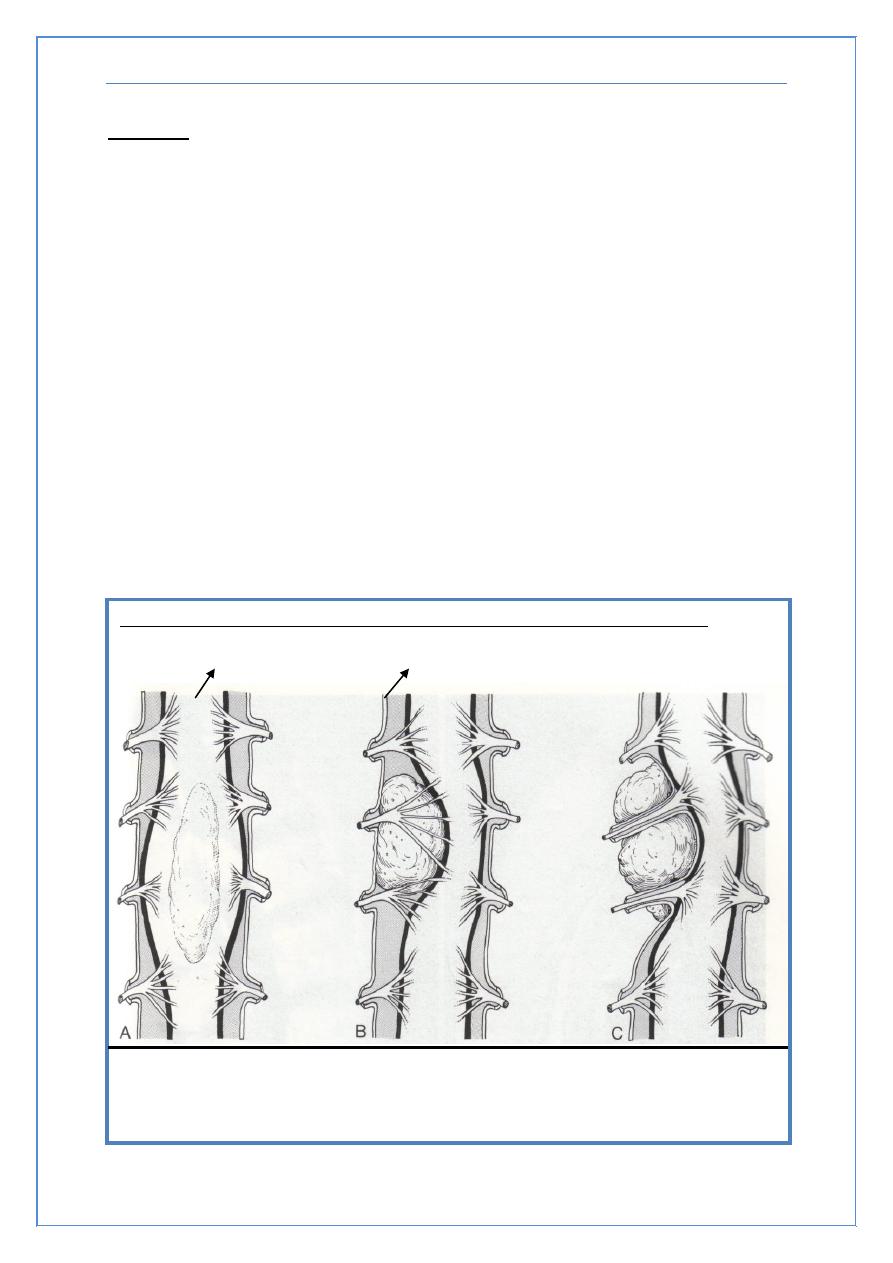
The picture below was added by the students it is not included in the lecture:
Spinal cord
Dura matter
The figure above demonstrates the different locations of spinal cord tumors, (A)
Intramedullary tumors (B) Extramedullary – Intradural tumors (C) Extramedullary –
Extradural tumors
.
Tumors
Metastatic or primary
- Extramedullary
Extradural (most common)
Bony, breast or prostate
Intradural (very rare)
Meninges - meningioma
Nerve root - schwannoma
- Intramedullary (very rare)
Metastatic
Primary - astrocytoma or ependymoma
Diseases of the Spinal Cord Prof. Akram Al-Mahdawi
8
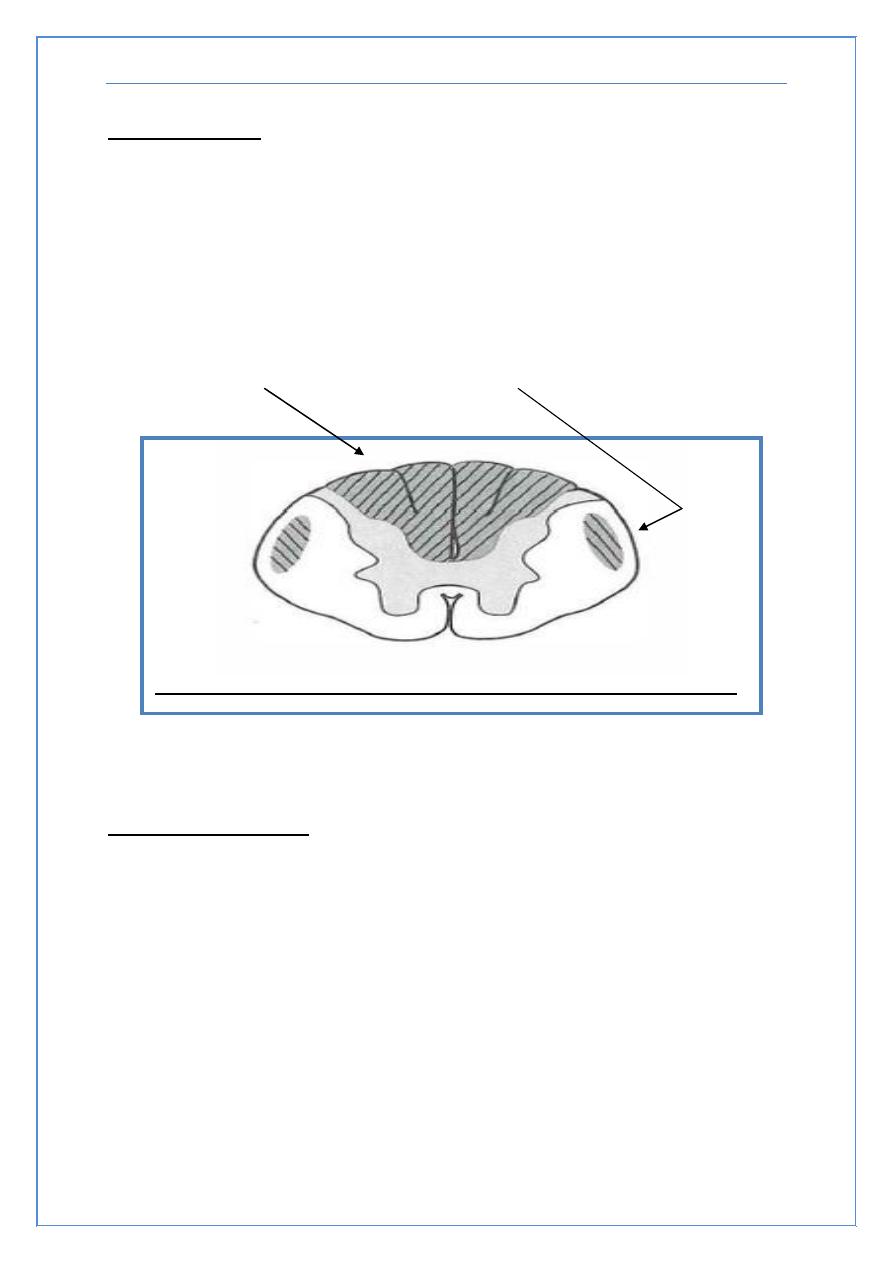
B12 Deficiency
Subacute combined degeneration of the cord
B12 deficiency
- Malabsorption of B12 secondary to pernicious anemia or
surgery
- Insufficient dietary intake - vegan
Posterior columns and corticospinal tract involvement with a
superimposed peripheral neuropathy
Transverse myelitis
Inflammation of the spinal cord
- Post- infectious
- Post- vaccinial
- Multiple sclerosis
Pain at level of lesion may precede onset of weakness/sensory
change/bladder and bowel disturbances.
The picture above was added by the students it is not included in the lecture
Diseases of the Spinal Cord Prof. Akram Al-Mahdawi
9
Infections Involving the Spinal Cord
Polio
- Only the anterior horn cells are infected
Tabes dorsalis
- Dorsal root ganglia and dorsal columns are involved
- Tertiary syphilis
- Sensory ataxia, “lightening pains”
HIV myelopathy
- Mimics B12 deficiency (Subacute combined degeneration of the
cord)
HTLV-1 myelopathy
- Tropical spastic paraparesis
Multiple Sclerosis
Demyelination is the underlying pathology
Cord disease can be presenting feature of MS or occur at any time
during the course of the disease
Lesion can be at any level of the cord
- Patchy
- Transverse
Devic’s syndrome or myelitis optica
- Transverse myelitis with optic neuritis
Diseases of the Spinal Cord Prof. Akram Al-Mahdawi
10
Vascular Diseases of the Spinal Cord
Infarcts
Anterior spinal artery
- From atherosclerosis, during surgery in which the aorta is
clamped, dissecting aortic aneurysm
less often, chronic meningitis or following trauma
- posterior columns preserved (joint position sensation and
vibration)
- weakness (corticospinal tracts) and pain/temperature loss
(spinothalamic tracts)
Artery of Adamkiewicz at T10-11
Watershed area
- upper thoracic
Arteriovenous malformation (AVM) and venous angiomas
Both occur in primarily the thoracic cord
May present either acutely, sub acutely or chronically (act as a
compressive lesion)
Can cause recurrent symptoms
If they bleed:
- Associated with pain and bloody CSF
Notoriously difficult to diagnose
Hematoma - trauma, occasionally tumor
Other Disease of the Spinal Cord
Hereditary spastic paraparesis
- Usually autosomal dominant
Infectious process of the vertebrae
- TB, bacterial
Herniated disc with cord compression
- Most herniated discs are lateral and only compress a nerve root
Degenerative disease of the vertebrae
- Cervical spondylosis with a myelopathy
- Spinal stenosis
End
Diseases of the Spinal Cord Prof. Akram Al-Mahdawi
11
Appendix
(added by the students not included in the lecture):
The picture above summarizes the different locations of the spinal cord lesions.
Cases
Case (1)
A 19-year-old man is brought in to the emergency department after being stabbed in the back.
He has no past medical history and takes no medications. Muscle strength is absent and tone
is decreased in the right leg. The right patellar and Achilles reflexes are absent. Babinski
sign is present on the right. There is a loss of vibratory sense and toe joint position on the
right. There is a loss of pain and temperature sensation below T12 on the left. Which of the
following will cause a loss of pain and temperature sensation on the left side, beginning at T12?
A. Damage to left-sided lateral spinothalamic tracts at T10
B. Damage to left-sided lateral spinothalamic tracts at T12
C. Damage to left-sided lateral spinothalamic tracts at L1
D. Damage to right-sided lateral spinothalamic tracts at T10
E. Damage to right-sided lateral spinothalamic tracts at T12
Diseases of the Spinal Cord Prof. Akram Al-Mahdawi
12
Explanation:
The Brown-Sequard syndrome is associated with damage to the lateral spinothalamic tracts
causing contralateral loss of pain and temperature sensation beginning two levels below the
level of the lesion (remember that the spinothalamic tracts cross very early on in the
spinal cord). Therefore, a lesion of the right-sided lateral spinothalamic tracts at T10 will result in
a left-sided loss of pain and temperature sensation beginning at T12
So the answer is D
Case (2)
A 33-year-old white female comes to the office for the evaluation of weakness in her upper
extremities. She thinks she is unable to feel pain or heat, because she recently noted some
burn wounds on her fingertips, and does not know how she got them. She denies weakness in
her lower limbs, as well as any history of trauma, headache, bowel or bladder problems, neck
pain or facial pain. Examination reveals absent reflexes in her upper limbs. There is absent
pain and temperature sensation on the nape of neck, shoulders and upper arms in a 'cape'
distribution. Vibration and position sensations are preserved. Which of the following is the
most likely pathology of the patient's condition?
A. Caudal displacement of the cerebellar tonsils and vermis
B. Caudal displacement of the fourth ventricle
C. Cord cavitation
D. Focal cord enlargement
E. Disc herniation and cord compression
Explanation:
The above patient is most likely suffering from syringomyelia. Areflexic weakness in the upper
extremities and dissociated anesthesia (loss of pain and temperature with preserved position and
vibration) in a "cape" distribution are classic findings of this condition. The pathology involves
cavitary expansion of the spinal cord, which may produce myelopathy. There is destruction of the
gray and white matter adjacent to the central canal. The most characteristic feature is the
presence of a cord cavity, which usually communicates with the central canal of the spinal cord.
The most frequent site of involvement is the lower cervical or upper thoracic region. When the
syringes occur in the upper cervical cord and extend proximally to involve the medulla oblongata,
the condition is called syringobulbia. Acquired causes of syringomyelia include trauma,
inflammatory spinal cord disorders or spinal cord tumors. Occasionally, syringomyelia is
idiopathic.
So the answer is C