
1
Fifth stage
Radiology
Lec-7
د.محمد
2/3/2016
Chest imaging -2
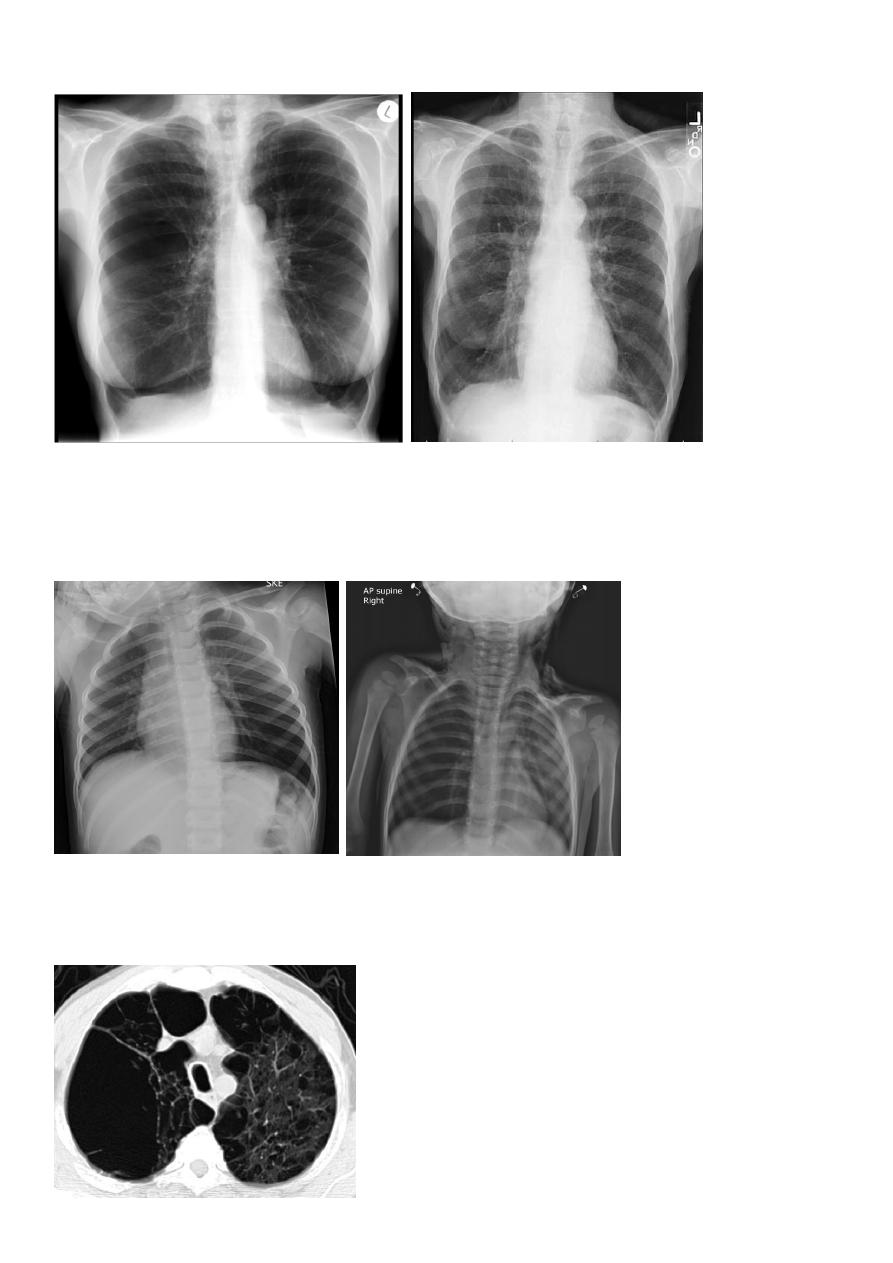
Pulmonary emphysema
Pulmonary emphysema is defined as the "abnormal permanent enlargement of the
airspaces distal to the terminal bronchioles accompanied by destruction of the alveolar wall
and without obvious fibrosis". Emphysema is one of the entities grouped together
as chronic obstructive pulmonary disease
Radiographic features
Plain film
Except in the case of very advanced disease with bulla formation, chest radiography does
not image emphysema directly, but rather infers the diagnosis due to associated features :
hyperinflation:
1.flattened hemidiaphragm(s): most reliable sign
2.ncreased and usually irregular radiolucency of the lungs
3.increased retrosternal airspace
4.increased antero-posterior diameter of chest
5.widely spaced ribs
6.sternal bowing
7.tenting of the diaphragm
9.vascular changes paucity of blood vessels ( absent pulmonary markings in outer 1/3 of the
lung fields )
10 .pulmonary arterial hypertension
pruning of peripheral vessels
increased calibre of central arteries
right ventricular enlargement
2
Emphyzema
Unilateral obstructive emphysema
unilateral emphysema or atelectasis are the most common findings; only uncommonly will
a radio-opaque foreign body be demonstrated ,
Aspirated foreign bodies have a predominance for the right tracheo bronchial tree.
Pulmonary bullae are focal regions of emphysema with no discenible wall which measure
more than 1cm in diameter

3
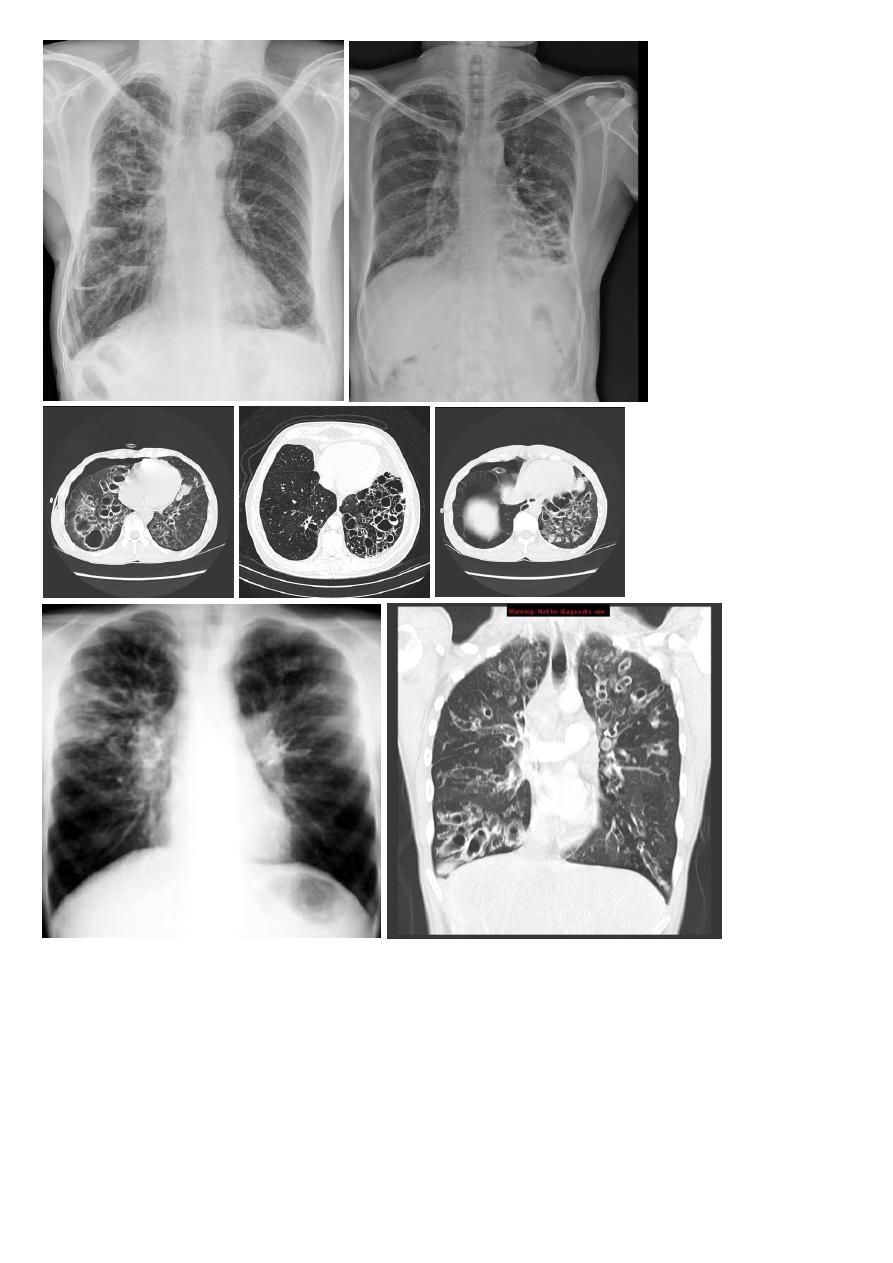
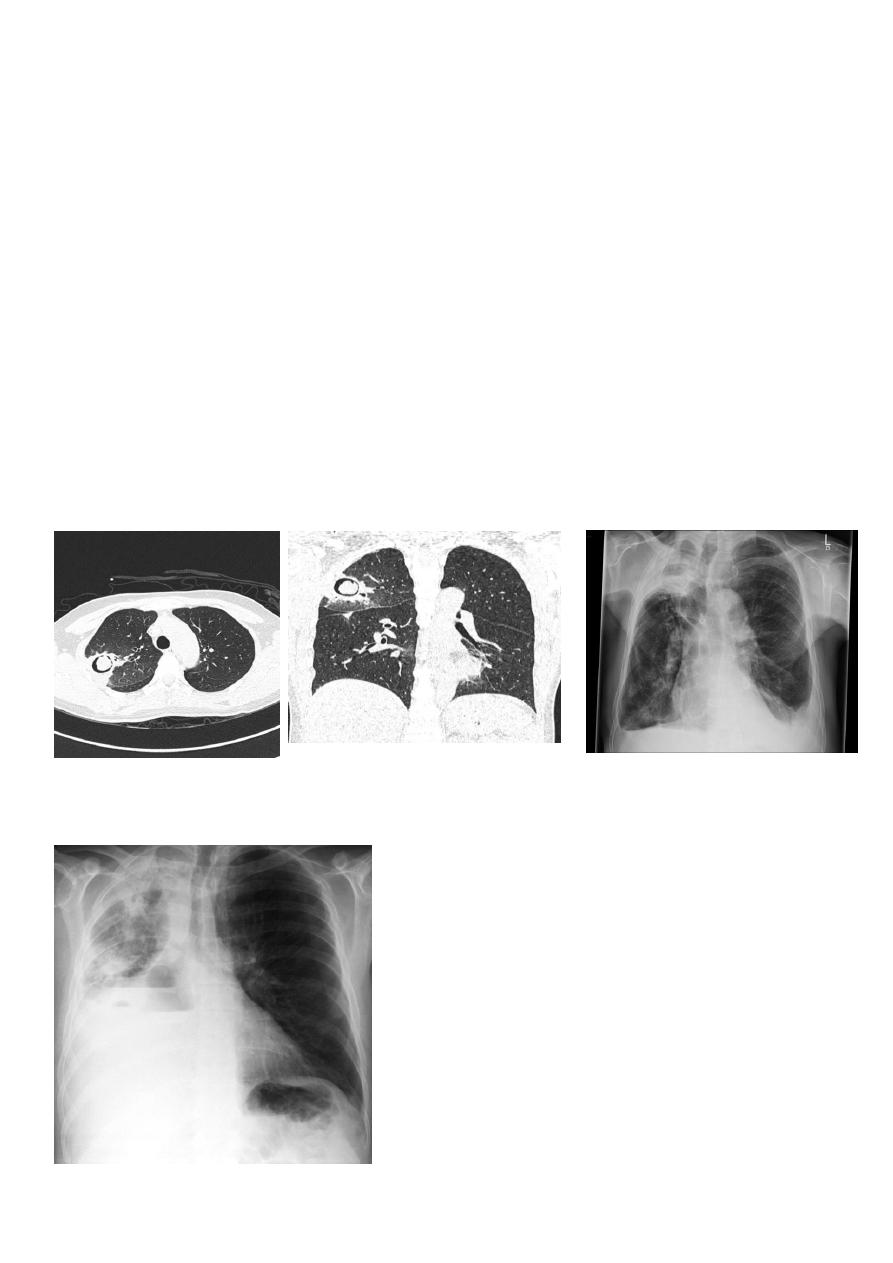
Bronchiactasis
Bronchiectasis refers to abnormal dilatation of the
clinical settings. CT is the most accurate modality for diagnosis. It is largely considered
irreversible
Causes of bronchiactasias:
very important to consider
post-infective (most common)
necrotising bacterial pneumonia, e.g Staph. aureus, Klebsiella, B. pertussis
granulomatous disease, e.g tuberculosis, MAIC, histoplasmosis
allergic bronchopulmonary aspergillosis (ABPA)
congenital
congenital cystic bronchiectasis
ciliary dysfunction syndromes, e.g. Kartagener syndrome
bronchial obstruction
malignancy, e.g. bronchogenic carcinoma
chronic aspiration lung changes
Plain radiograph
Chest x-rays are usually abnormal
are seen in cylindrical bronchiectasis, and
may be seen in cystic bronchiectasis.
Honey comb shadow
3.Overall there appears to be an increase in bronchovascular markings, and bronchi seen
end on may appear as ring shadows .
4.Pulmonary vasculature appears ill-defined, thought to represent peri bronchovascular
fibrosis .
4
TB of the lung
Tuberculosis encompasses an enormously wide disease spectrum affecting multiple organs
and body systems predominantly caused by the organism
Pulmonary manifestations of tuberculosis are varied and depend in part whether the
infection is primary or post-primary. The lungs are the most common site of primary
infection by
and are a major source of spread of the disease .
5
Have 2 categories
Primary
Post primary TB
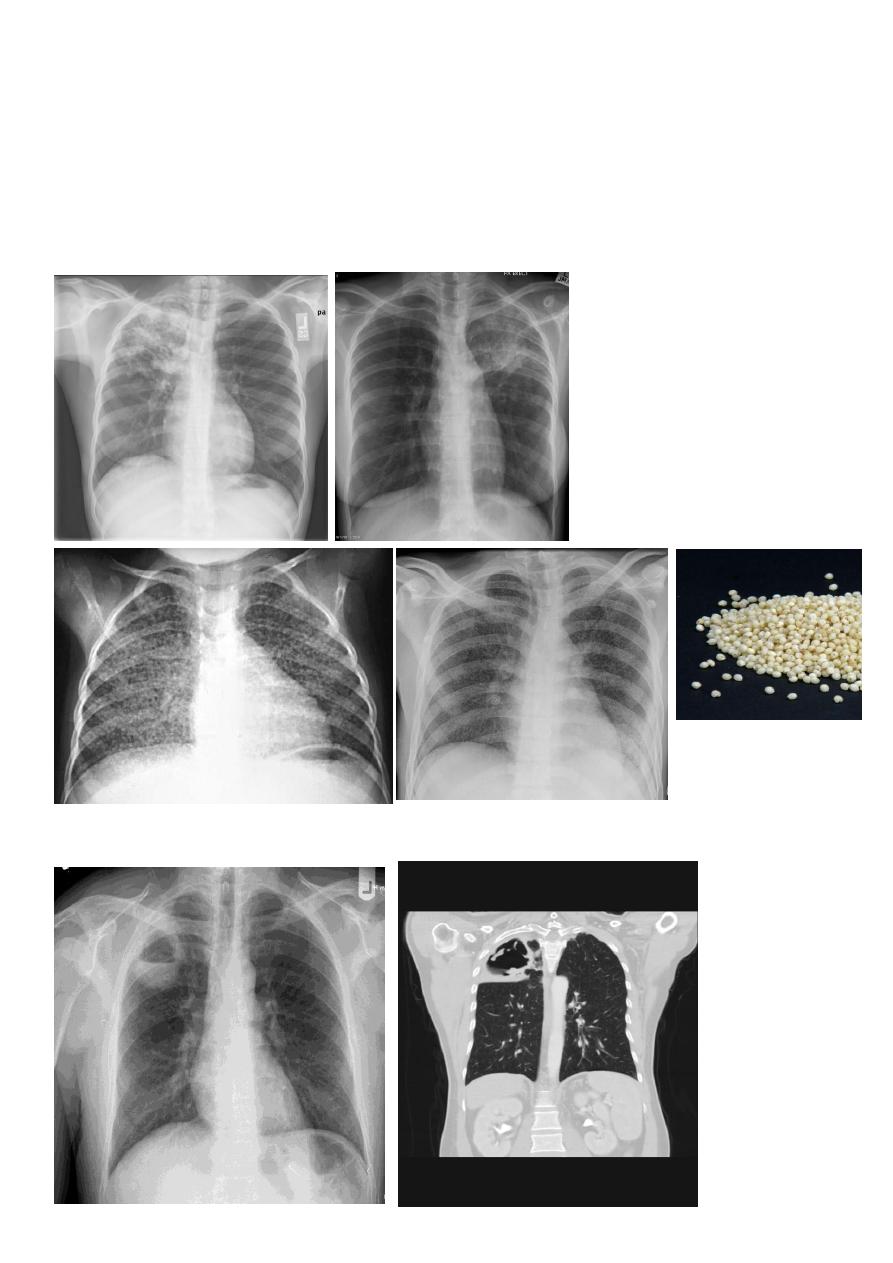
Primary pulmonary TB
Radiographic features
primary pulmonary tuberculosis
1.the initial focus of infection can be located anywhere within the lung and has non-specific
appearances ranging from too small to be detectable, to patchy areas or consolidation or
even lobar consolidation in RT upper or RT middle lobe . Radiographic evidence of
parenchymal infection is seen in 70% of children and 90% of adults called Ghon lesion , +/-
ipsilateral hilar or paratracheal Lymph adenopathy usually right sided
( Ghon focus + LAP ) called primary complex.
2.Later In most cases, the infection becomes localized and a caseating granuloma resolve
eventually calcifies with or without calcification of the regional LN , Calcification of nodes is
seen in 35% of cases . When a calcified node and a calcified Ghon lesion are present, the
combination is known as a Ranke complex.
3. Pleural effusions are more frequent in adults .
Post primary TB radiographic appearance
Post-primary pulmonary tuberculosis, also known as reactivation tuberculosis or secondary
tuberculosis occurs years later, frequently in the setting of a decreased immune status. In
the majority of cases, post-primary TB within the lungs develops in either :
* posterior segments of the upper lobes
*superior segments of the lower lobes
Typical appearance of post-primary TB
1.patchy consolidation or poorly defined linear and nodular opacities in both apices , upper
zone in one lung , & lower zone in other lung ( ulternating lesion ) .
2. Post-primary infections are far more likely to cavitate with multiple abscess formation &
air fluid level more develop in the posterior segments of the upper lobes.
6
3. Tuberculomas seen in post-primary TB and appear as a well defined rounded mass
typically located in the upper lobes .
4. Miliary tuberculosis is uncommon but carries a poor prognosis. It represents
haematogenous dissemination of an uncontrolled tuberculous infection. It is seen both in
primary and post-primary tuberculosis. Although implants are seen throughout the body,
the lungs are usually the easiest location to the image. Miliary deposits appear as 1-3 mm
diameter nodules . are uniform in size and uniformly distributed
TB abscess
7
Complications
Recognized complications include:
1.colonisation of cavities by fungus, e.g. aspergilloma
3.arterial pseudoaneurysms
bronchial artery pseudo aneurysm
pulmonary artery pseudo aneurysm / Rasmussen aneurysm
Aspergiloma
Broncho pleural fistula

8
Lung tumor
Lung cancer, or frequently, if somewhat incorrectly, known as bronchogenic carcinoma, is
the most common cause of cancer in men, and the 6th most frequent cancer in women
worldwide. It is the leading cause of cancer mortality worldwide in both men and women
and accounts for approximately 20% of all cancer deaths
subtype has a different radiographic appearance, demographic, and prognosis:
squamous cell carcinoma of the lung
large cell carcinoma of the lung
small cell carcinoma of the lung
Other malignant pulmonary neoplasms include lymphoma
Associations
Various paraneoplastic syndromes can arise in the setting of lung cancer
Sequamous cell CAmost common primary lung malignancy to cause paraneoplastic
syndromes and SVC obstruction
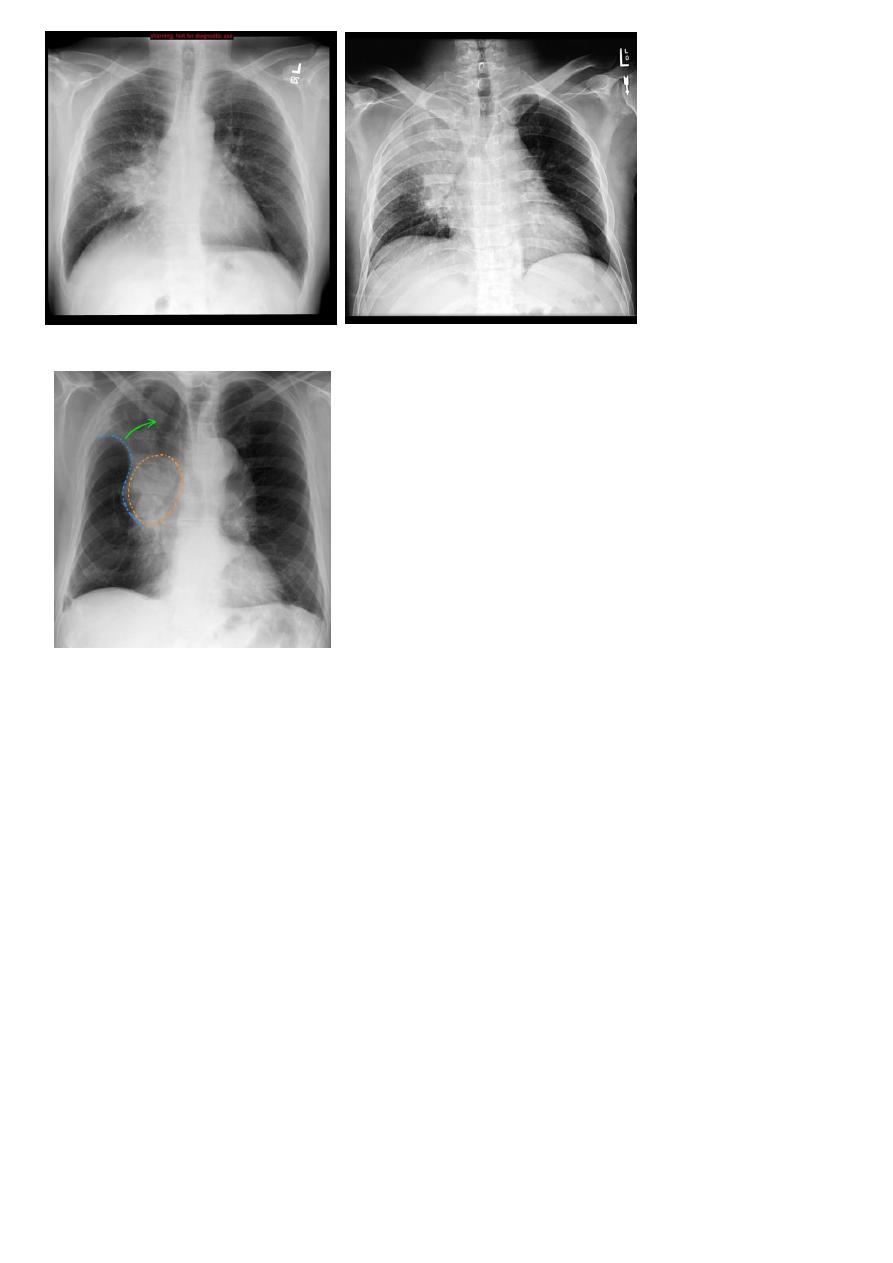
Radiology of BGCA
The appearance depends on the location of the lesion.
1.The more central lesions may merely appear as a bulky hilum, representing the tumor and
local nodal involvement the lesion is irregular in outline have spiky or sun ray spiculation .
2.Lobar collapse may be seen due to obstruction of a bronchus. When the right upper lobe
is collapsed and a hilar mass is present, this is known as the Golden S sign.
3.A more peripheral location may appear as a rounded or spiculated mass. Cavitation may
be seen as an air-fluid level , more to be large cell CA .
4.Chest wall invasion is difficult to identify on plain films unless there is destruction of the
adjacent rib or evidence of soft tissue growing into the soft tissues superficial to the ribs.
5.A pleural effusion may also be seen, and although it is associated with a poor prognosis,
not all effusions are due to malignant involvement of the pleural space.
9
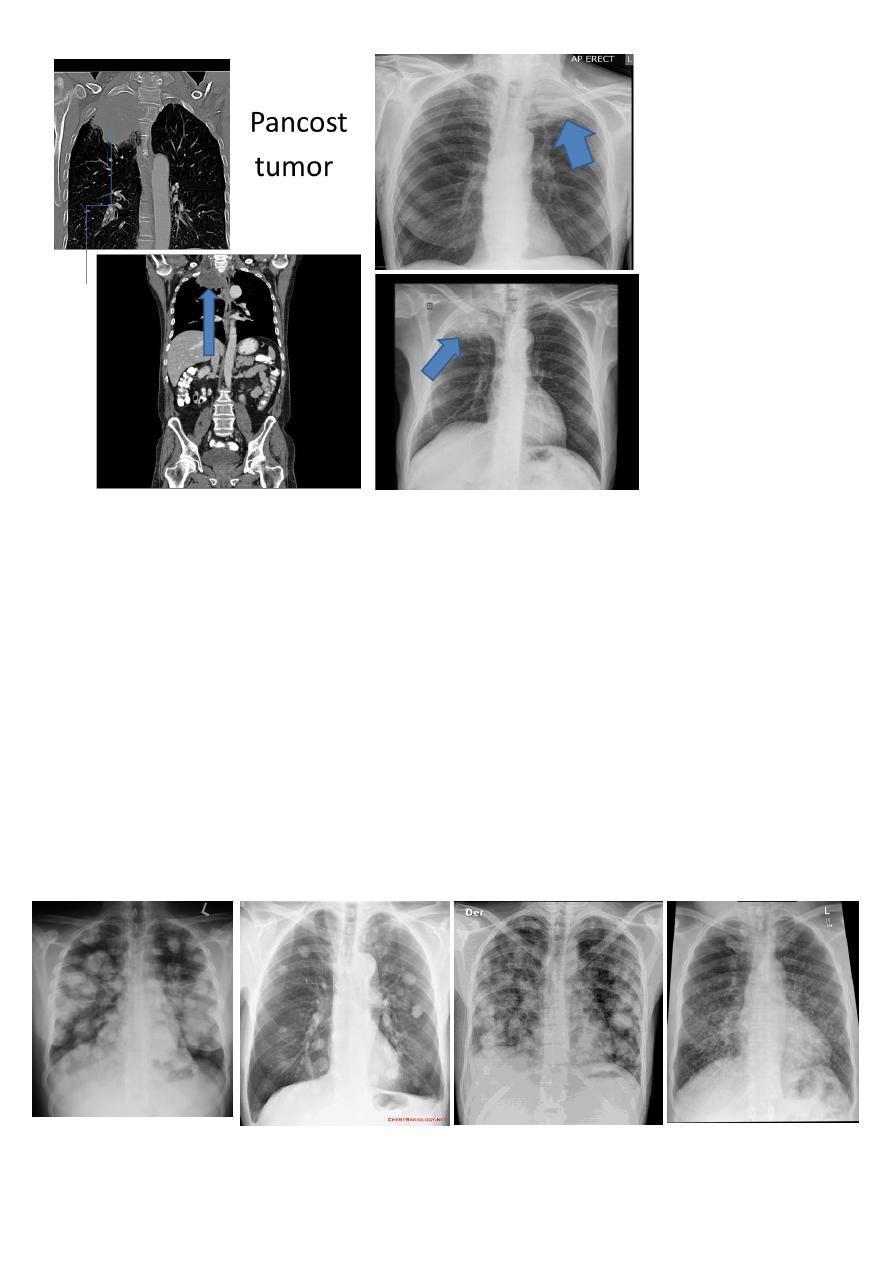
Pancosts tumor
A Pancoast tumour, otherwise known as superior sulcus tumour, refers to a relatively
uncommon situation where a primary bronchogenic carcinoma arises in the lung apex and
invades the surrounding soft tissues , adeno CA being the most frequent type ,
Plain film
Plain films demonstrate a soft tissue opacity at the apex of the lung. Occasionally with rib
involvement with extension into the supraclavicular fossa may be evident with surrounded
bony destruction . Lordotic views may be helpful .
Must important complication is involvement of the sympathetic chain >>>>
* Ptosis
* Meiosis
* unhydrosis
10
Secondary lung tumor
Pulmonary metastases are common and the result of metastatic spread to the lungs from a
variety of tumors and can spread via blood or lymphatics.
1.Cannonball metastases refer to large well circumscribed, round multiple opacities like
cannonballs
2.lymphangitis carcinomatosis , is the term given to tumor spread through the lymphatics
of the lung , and is most commonly seen secondary to adenocarcinoma Unfortunately up to
a quarter of patients with subsequently established lymphangitic carcinomatosis have
normal chest x-rays . When abnormal the most common finding is of a reticulonodular
pattern, with thickening of the interlobular septae which may resemble Kerley B lines + /-
pleural effusion .
3.innumerable small metastases (miliary pattern).