4th stage
MedicineLec-
Dr.Jasim
23/2/2016
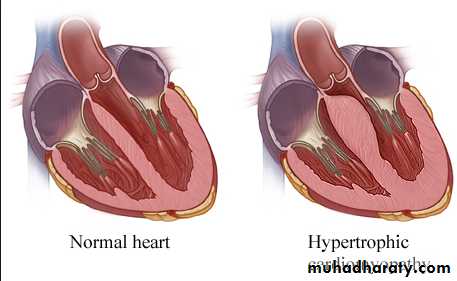
Hypertrophic cardiomyopathyThis is the most common form of cardiomyopathyGenetic disorder, usually with autosomal dominant transmission
Types :
Obstructive 25 %Non obstructive
The hypertrophy may be generalised or confined largely to the interventricular septum (asymmetric septal hypertrophy) or other regions (e.g. apical hypertrophic cardiomyopathy)
Microscopically :
HCM is characterized by myocyte disarray in which there is loss of the normal parallel arrangement of cardiomyocytes, cells instead forming circles or whorls around foci of connective tissue. The myofibrillar architecture within cells is also disrupted (myofibrillar disarray).Pathophysiology :
Dynamic LV outflow tract obstruction ( atleast >30 mm, usually > 50mm Hg)
Diastolic dysfunction
Myocardial ischemia
Mitral regurgitation
Arrhythmias
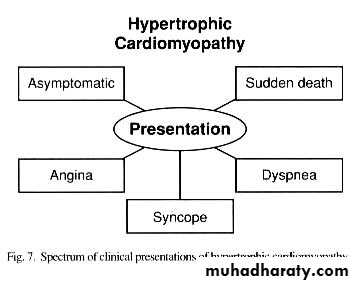
Signs :
Apex localized, sustainedDouble apex beat
Palpable S4
Prominent “a” wave
Rapid upstroke carotid pulse, “jerky” bifid (spike-and-dome pulse)
Harsh systolic ejection murmur at base
MR: systolic murmur
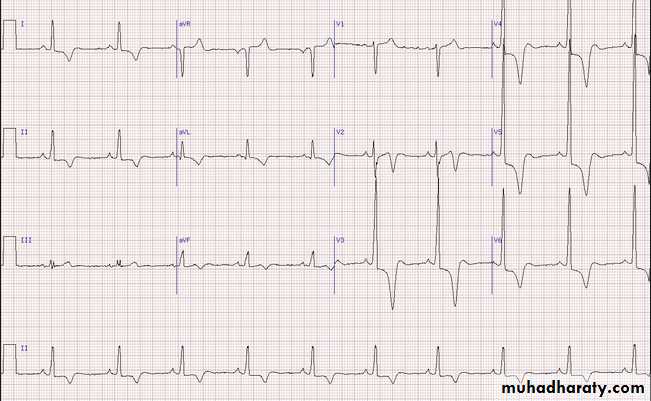
ECG :
LA enlargementPathologic Q waves, most commonly in the inferolateral leads.
Voltage criteria for LVH
ECG 1
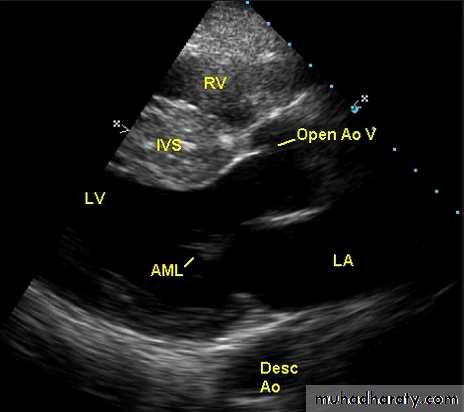
ECHO Echocardiography is diagnostic

Treatment :
All first degree relatives: screening…echocardiography/genetic counseling
Avoid competitive athletics
Symptomatic : Beta blockers or calcium channel blockers
Antiarrythmic drugs : Disopyramide or amoidarone
Invasive treatment :
High risk or non responders to medical treatmentICD ( high risk patients)
DDD pacemaker
Alcohol septal ablation
Surgery Myectomy
Restrictive Cardiomyopathy (RCMP)
Definition:
Restrictive cardiomyopathy is characterized by decreased ventricular compliance(stiff ventricles), usually secondary to infiltration of the myocardium.
These patients have impaired ventricular filling and reduced diastolic volume, normal systolic function, and normal or near-normal myocardial thickness.
Amyloidosis is the most common cause in the UK
although other forms of infiltration (e.g. glycogen storage diseases) and a familial form of restrictive cardiomyopathy do occur.Diagnosis can be very difficult and requires complex Doppler echocardiography, CT or MRI, and endomyocardial biopsy.
Treatment is symptomatic but the prognosis is usually poor and transplantation may be indicated.
Arrhythmogenic right ventricular
cardiomyopathyIn this condition, patches of the right ventricular myocardium are replaced with fibrous and fatty tissue .
It is inherited as an autosomal dominant trait .
The dominant clinical problems are ventricular arrhythmias, sudden death and right-sided cardiac failure.The ECG typically shows a slightly broadened QRS complex and inverted T waves in the right precordial leads.
MRI is a useful diagnostic tool and is often used to screen the first-degree relatives of affected individuals.
Patients at high risk of sudden death can be offered an ICD.