ALS & Dementia
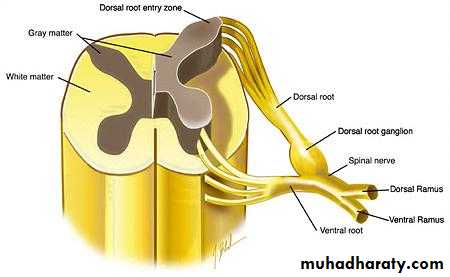
Anterior horn cell diseasesMany motor nerve diseases principally affect the anterior horn cell body; these are usually neurodegenerative (e.g. motor neuron disease) or hereditary (e.g. spinal muscular atrophy) or infection like polio.
(MND) Motor neuron disease
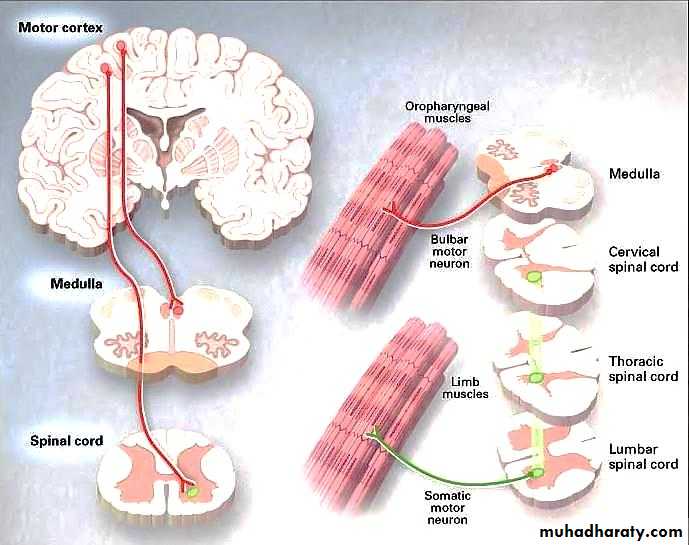
Motor neuron disease e.g.(amyotrophic lateral sclerosis) is a progressive neuronal degenerative disease that leads to severe disability and death begins between the ages of 30 and 60 years , It is characterized by degeneration of anterior horn cells in the spinal cord, motor nuclei of the lower cranial nerves in the brainstem, and corticospinal and corticobulbar pathways. So there is features of combination of upper motor and lower motor type (characterized clinically by wasting, weakness and fasciculation of the affected muscles with hyperreflexia. without accompanying sensory, cerebellar, sphincter or ocular muscles involvements.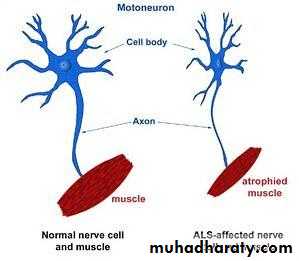
Investigation:
EMG, TFT, Cervicomedullary MRI.Treatment:
Supportive measures no treatment till now.
Dementia
It is defined as an acquired deterioration in cognitive abilities that impairs the successful performance of activities of daily living. Memory is the most common cognitive ability lost with dementia.
Causes of Dementia
The classification of dementing illnesses into reversible and irreversible disorders is a useful approach to differential diagnosis.
Reversible Causes
Hypothyroidism
Thiamine deficiency
Vitamin B12 deficiency
Subdural hematoma
Chronic infection
Brain tumor
Irreversible/Degenerative Dementias
Alzheimer's
Huntington's
Vascular dementia
Alzheimer's disease
Approximately 10% of all persons over the age of 70 have significant memory loss, and in more than half the cause is AD.
Clinical Manifestations
The most common complaint, often made by a career, spouse or other family member rather than by the patient, is of problems with memory. Patients become repetitive in questioning, forgetting that they asked the same question recently, the patient is unable to work, is easily lost and confused, Language becomes impaired—first naming, then comprehension, and finally fluency. In the late stages of the disease, some persons remain ambulatory but wander aimlessly. Loss of judgment and reasoning is inevitable.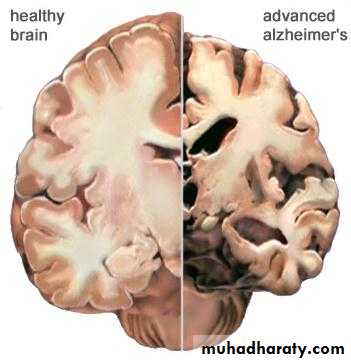
Vascular Dementia
Dementia associated with cerebrovascular disease, cerebrovascular disease appears to be a more common cause of dementia, due to the increased prevalence of intracranial atherosclerosis. Individuals who have had several strokes may develop chronic cognitive deficits, commonly called multi-infarct dementia. The strokes may be large or small (sometimes lacunar) and usually involve several different brain regions.Treatment of AD
The management of AD is challenging and gratifying, despite the absence of a cure or a robust pharmacologic treatment. The primary focus is on long-term amelioration of associated behavioral and neurologic problems, as well as providing caregiver support.
Building rapport with the patient, family members, and other caregivers is essential to successful management. In the early stages of AD, memory aids such as notebooks and posted daily reminders can be helpful.
Pharmacological
Cholinesterase inhibitors
The cholinesterase inhibitors (AChEIs) have been specifically developed as symptomatic treatment for AD.
There are currently three AChEIs licensed for the treatment of mild to moderate AD:
Donepezil (Aricept)
Galantamine (Reminyl)
Rivastigmine (Exelon).
Memantine
Potentially preventing glutamate-mediated neurotoxicity. It is a N-methyl-d-aspartate (NMDA)-receptor antagonist.
END
Appendix (added by the students not included in the lecture):
Case (1)
A 45-year-old man comes to the office for the evaluation of excessive wasting of his extremity muscles, which is more apparent on the extensor side. The weakness began distally and asymmetrically. He recently started to have difficulties with swallowing, chewing, and speaking. He feels some movements in his face and tongue. He also has muscle stiffness. His bowel, bladder, cognitive, and sensory functions are intact. The physical examination reveals excessive wasting of his muscles, which is more prominent in the lower extremities. Fasciculations and hyperreflexia of all extremities are noted. His bulbar reflexes are decreased. What neural pathway is most likely damaged?
Pyramidal tract
Lower motor neuron
Upper motor neuron
Lower and upper motor neuron
Cerebral cortex
Explanation:
This patient has amyotrophic lateral sclerosis (ALS), which is one of the worst and most devastating neurodegenerative disorders. It is characterized by the presence of both upper and lower motor neuron lesions. Spasticity, bulbar symptoms, and exaggerated deep tendon reflexes are signs of upper motor neuron damage, while fasciculations indicate a lower motor neuron damage. Weakness and wasting of the muscles may be due to both upper and lower motor neuron lesions.
So the answer is D
Case (2)
A 74-year-old woman comes to your office with her husband for a routine check-up. Her husband complains that she often forgets to take her blood pressure pills. He feels that her speech has changed because she occasionally struggles to find appropriate words. Two days ago, she drove to the nearby grocery store and did not find her way back. She has difficulty falling asleep and she always wakes up early in the morning. Her appetite is good. Which of the following is the best indicator of dementia in this patient?
Memory impairment
Language difficulty
Sleep abnormalities
Advanced
Impaired daily functioning
Explanation:
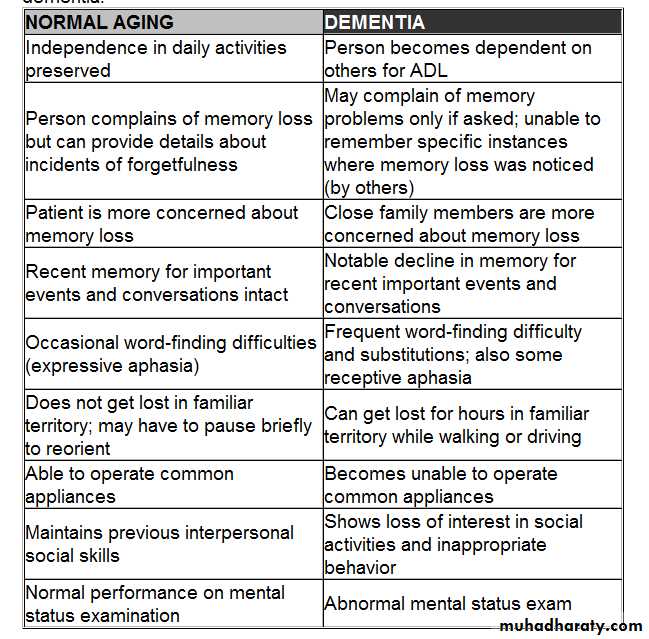
This woman is an elderly patient with forgetfulness. word finding aphasia. impairment of daily functioning. and insomnia. Of these symptoms. the most specific for dementia is impairment in functioning. Social and personal functioning requires performance of activities of daily living (e.g. personal hygiene. dressing. food acquisition and intake. self administration of medications). navigation through surroundings. and the ability to operate common appliances. This patient shows deficiencies in at least two areas of functioning. Forgetfulness. word finding aphasia. and insomnia can occur with normal aging and are therefore less specific for dementia. However, many patients with age-related memory loss will not get lost in common settings nor will they have poor recollection of when they experienced memory loss. The table below summarizes the changes in normal versus dementia.