Movement disorders 2
ChoreaChorea is derived from the Greek word ‘chorea’ meaning a dance they are rapid, purposeless, irregular, jerky movements that seem to flow randomly from one part of the body to another.
Causes
Chorea has many causes which can be simply divided into inherited and acquired:
1-Inherited causes
Huntington’s disease
Wilson’s disease
2-Acquired causes
Stroke
Drug induced: (Levodopa and other dopaminergic drugs, Antipsychotic drugs, Oral contraceptives, Phenytoin)
Chorea gravidarum(during pregnancy)
Thyrotoxicosis
Systemic lupus erythematosus/antiphospholipid syndrome
Post-infective Sydenham’s chorea
Huntington’s disease
Huntington’s disease (HD) is a slowly progressive autosomal dominant neurodegenerative disorder and the most important inherited cause of chorea discovered by George Huntington in 1872. In 1993, the causative gene defect was identified as a CAG triplet repeat expansion mutation in the HD gene on chromosome 4. Onset is usually in adult life with a mean age of about 40 years it progresses inexorably, with death occurring 15–20 years from HD.
Clinical features
Motor features
Subtle motor abnormalities seen early in the disease include general restlessness, abnormal eye movements, and fidgety movements of fingers, hands and toes during stress or when walking. Also Dysarthria.
Cognitive features
Cognitive abnormalities are variable but universal in HD. The key cognitive abnormalities seen are impaired executive function with poor planning and judgment, disorganized actions.
Psychiatric features
Psychiatric symptoms are common, particularly depression and anxiety. Irritability is also very common and some patients become aggressive.
Investigation
MRI imaging to exclude stroke
Wilson screen(Serum caeruloplasmin, serum copper, urinary copper level and KF ring)
Pregnancy test
Anti-dsDNA, ANA
Thyroid function tests
Antistreptolysin O (ASO) titer
Treatment
No intervention currently slows or halts the degenerative process.Drug used to treat chorea
Chorea usually responds to treatment with dopamine receptor blockers or dopamine depleting agents:
dopamine receptor blockers e.g.: Olanzapine, Risperidone, Quetiapine
Dopamine-depleting agents e.g.: Reserpine, Tetrabenazine
Benzodiazepines e.g.: Clonazepam
Drugs Used to Treat Depression and irritability in Huntington’s disease:
Selective serotonin reuptake inhibitors e.g.: Fluoxetine
Tricyclic anti-depressants e.g.: Nortriptyline
Sydenham’s chorea (SC):
One of the major manifestations of rheumatic fever, appears months after the index streptococcal infection in children with rheumatic fever, the usual clinical picture of SC is the insidious development of choric movements in a girl during childhood or adolescence. The chorea evolves over weeks, then recedes within 6 months.
Treatment: is valproicacid.
Dystonia
Is a disorder marked by the presence of involuntary, sustained muscle contractions causing abnormal postures. Pain may accompany the motor symptoms of dystonia.
Classification of Dystonia
Body Distribution
Focal: single body region
Segmental: contiguous body regions
Generalized: both legs and at least one other body region
Multifocal: noncontiguous body regions
Hemidystonia: involving one half of the body
Etiology
Primary: Dystonia is only sign; may be sporadic or inherited
Secondary: Dystonia occurring associated with a defined etiology or associated with other neurologic abnormalities
Primary dystonia
Young onset dystonia (before the age of 26 years) most commonly manifests with limb onset dystonia, followed by subsequent generalization In severe cases, patients can suffer disabling postural deformities and was referred to in the older literature as dystonia musculorum deformans or Oppenheim’s dystonia It has an autosomal dominant inheritance. This condition is more common in Ashkenazi Jewish, with a possible founder in Eastern Europe about 3 centuries ago.
Focal Dystonias
These are the most common forms of dystonia. They typically present in the fourth to sixth decades and affect women more than men. The major types are
Blepharospasm—dystonic contractions of the eyelids with increased blinking that can interfere with reading, watching TV, and driving.
Oromandibular dystonia (OMD)
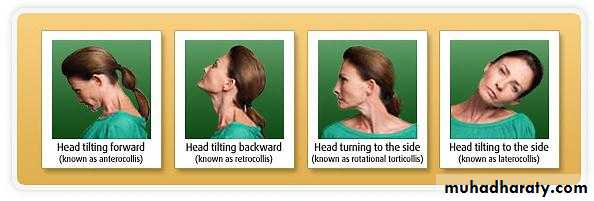
Cervical dystonia—dystonic contractions of neck muscles causing the head to deviate to one side (torticollis), in a forward direction (anterocollis), or in a backward direction (retrocollis).
Task-specific dystonia such as handwriting (writer's cramp), playing a musical instrument (musician's cramp)
Secondary Dystonias
These develop as a consequence of drugs or other neurologic disorders e.g.: Wilson disease, levodopa, metoclopramide etc.
Investigation:
MRI of brain and cervical spin
Wilson screen e.g.(serum copper ,serum ceruloplasmin ,KF ring)
Genetic study
Treatment
Treatment of dystonia are:
Treatment of a primary underlying condition is available e.g.: Wilson's disease
Anticholinergics (e.g.: trihexyphenidyl)
Baclofen (muscle relaxant)
Clonazepam (bezodiazepin)
Tetrabenazine (dopamine depleting drug)
Botulinum toxin has become the preferred treatment for patients with focal dystonia
DBS of the pallidum can provide dramatic benefits for patients with primary dystonia.
Oculogyric crisis
Is the name of a dystonic reaction to certain drug or medical condition. The term "oculogyric " refer to rotating of eyeballs also crisis associated with backwards and lateral flexion of the neck ,widely opened mouth, tongue protrusion and agitation.Causes: some e.g.:
Neuroleptic drugs e.g.: olanzapine
Metoclopramide and domperidon
Treatment
Antimuscarinic e.g.: procyclidin, benzatropin
Diphenhydramine
Diazepam
Tic
Brief, repeated, stereotyped muscle contractions that are often suppressible. Can be simple and involve a single muscle group or complex and affect a range of motor activities.
Tourette's syndrome (Ts)
TS is a neurobehavioral disorder named after the French neurologist Georges Gilles de la Tourette, It predominantly affects males, and TS is characterized by multiple motor tics often accompanied by vocalizations (phonic tics). Associated behavioral disturbances include anxiety, depression, attention deficit hyperactivity disorder, and obsessive-compulsive disorder.
Treatment
Patients with mild disease often only require education and counseling (for themselves and family members). Drug treatment is indicated when the tics are disabling and interfere with quality of life. Therapy is generally initiated with the alpha-agonist e.g.: clonidine and Guanfacine also atypical antipsychotic can be used, the DBS (deep brain stimulation) is going on.
Hemifacial spasm
This is a benign, usually painless but often distressing condition, characterized by unilateral, involuntary, irregular tonic or clonic contractions of muscles supplied by the facial nerve. It is now generally accepted that hemifacial spasm is usually caused by extrinsic compression of the root entry zone of the facial nerve, generally by vascular structures such as the vertebral or basilar arteries or their branches.Drug treatment with carbamazepine, gabapentin, clonazepam and baclofen are rarely very effective and seldom result in resolution of symptoms
Botulinum toxin injection into affected muscles is now the first line for those patients who want treatment
Surgical decompression.
Hemiballismus
Hemiballismus is a violent form of chorea composed of wild, flinging, large-amplitude movements on one side of the body. Proximal limb muscles tend to be predominantly affected. The movements may be so severe as to cause exhaustion, dehydration, local injury, and in extreme cases, death. The most common cause is a partial lesion (infarct or hemorrhage) in the subthalamic nucleus (STN).Athetosis
Slow, distal, writhing, involuntary movements with a propensity to affect the arms and hands.Causes: the same as chorea.
END
Note: the below cases were added by the students (it’s not included in lecture)
Case (1):A 47-year-old obese female comes to the office for the evaluation of recent episodes of mood instability. Her mood varies between sad and irritable. She denies any other symptoms. Except for some mild forgetfulness. She tearfully shares that she is convinced that she is going to die. As her father also developed similar symptoms around the same age and died subsequently. On physical examination. Writhing movements of the extremities are prominent this patient's clinical presentation is most consistent with:
Alzheimer's disease B. Pseudodementia C. Huntington's disease D. Hypothyroidism
Explanation:
This patient has Huntington's disease. This autosomal dominant condition affects both sexes equally. The age at presentation is typically between 30-50 years. The typical presenting features are mood disturbances (depression, apathy), dementia, and choreiform movements (facial grimacing, ataxia, dystonia, tongue protrusion, writhing movements of extremities). The symptoms are progressive, eventually disabling the patient severely. So the answer is C
Case (2):
A 27 -year-old woman presents to the ER with severe vomiting and abdominal pain that started several hours ago. She describes her emesis as "yellowish." She has a history of alcohol and cocaine use. Her temperature is 36.7C (98F), pulse is 98/min, respirations are 16/min, and blood pressure is 140/86 mmHg. Physical examination reveals dryness of the oral mucosa. Her abdomen is soft, non-distended, and without hepatosplenomegaly. Mild epigastric tenderness is present on deep palpation. Bowel sounds are increased. No rebound or rigidity is noted. She is treated with intravenous normal saline and metoclopramide. Several hours later she complains of neck pain and her neck muscles are noted to be stiff and tender. Which of the following best explains this patient's current complaints?
Meningeal irritation B. Fat necrosis C. Medication side effect D. Eosinophilic myositis
Explanation:
This patient is experiencing a metoclopramide-induced dystonic reaction. Metoclopramide is a dopamine receptor antagonist used to treat nausea, vomiting, and gastroparesis. It has significant prokinetic properties, which include promoting increased peristalsis, increased strength of gastric contractions, and relaxation of the pyloric sphincter. Common side effects include agitation and loose stools. Extrapyramidal symptoms (tardive dyskinesia, dystonic reactions, and Parkinsonism) occur less frequently. Rarely, neuroleptic malignant syndrome may occur. Treatment for a dystonic reaction involves discontinuation of the medication and administration of benztropine or diphenhydramine. So the answer is C
Case (3):
A 43-year-old man presents to your office complaining of periodic involuntary head turning and head fixation to the right side. Physical examination reveals a hypertrophied left sternocleidomastoid muscle. What is the most likely diagnosis?
This patient suffers from torticollis. A focal dystonia of the sternocleidomastoid muscle. Dystonia is defined as sustained muscle contraction resulting in twisting. Repetitive movements. Or abnormal postures. It may be focal (affecting only one muscle) or diffuse. Torticollis can be congenital, idiopathic. Secondary to trauma or local inflammation. Or drug-induced. Medications commonly responsible include the typical antipsychotics. Metoclopramide. And prochlorperazine.