


Inflammations of the larynxacute and chronic
Acute laryngitis
Acute non-specific laryngitis:Aetiology:
1- Up.respiratory tact infection
2- Trauma(voice abuse).
3- Irritation(tobacco and fumes).
Clinical features:
1- Hoarseness which might progress to aphonia
2- Sore throat
3- Irritant paroxysmal dry cough
4- Pyrexia and malaise
5- On exam. : redness, swelling and discharge
Treatment:
1- Absolute voice rest (whispering is not voice rest)
2- Steam inhalation(tincture benzoin or menthol)
3- Analgessics and antihistamines
4- Antibiotics (for bact. infection)
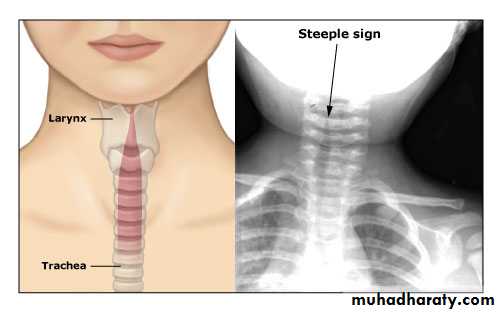
Acuta laryngotracheobronchitis(croup)
Age: young children, mean age 18 months
Micro-organism: Parainfluenza virus type 1
Pathology:
Whole laryngotracheal tract is affected but mainly the subglottis
Clinical featutes:
1- gradual onset
2- history of up.resp.tract infectin
3- croupy cough(crowing or bark of a seal) is the chief complaint
4- hoarseness
5- pyrexia
6- stridor
7- dyspnea and cyanosis in severe cases
On examination: the child is irritable, crying, dyspnic and assume supine position
Radiology: church steeple sign, due to narrowing of the subglottic region.
Treatment:1- Hospitalization
2- Rest and reassurance
3- Humidification of inspired air
4- Oxygen
5- I.V fluids
6- Antibiotics (controversial)
7- Steroids (controversial)
8- Intubation and tracheostomy: rarely required
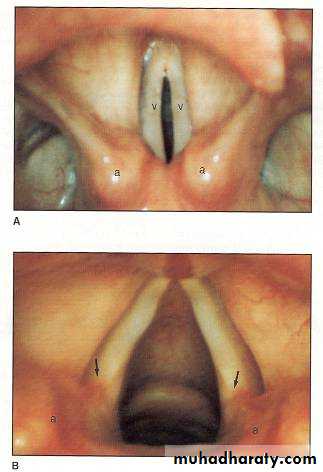
Acute epiglottitis
Age: older children, mean age 2-6 yearsM.O: H.influenzae type B
Pathology: It affects the
Supraglottic region of the larynx and mainly the epiglottis
Clinical features:
1- Rapid onset
2- Stridor is the main feature, inspiratory
3- Sore throat, odynophagia and drooloing saliva
4- Dyspnea and cyanosis
On examination: the child is quite (in croup usually irritable and crying) and prefers sitting position (tripod sign).
Exam. of the larynx by mirror or tongue depressor should be avoided(laryngeal spasm and edema might develope)
Radiology: thumb print sign
Treatment:1- Hospitalization
2- secure the airway :tracheostomy or intubation is needed in larger percentages than croup
3- humidification
4- antibiotics: amoxiclav or cefotaxim
5- steroids: cntroversial
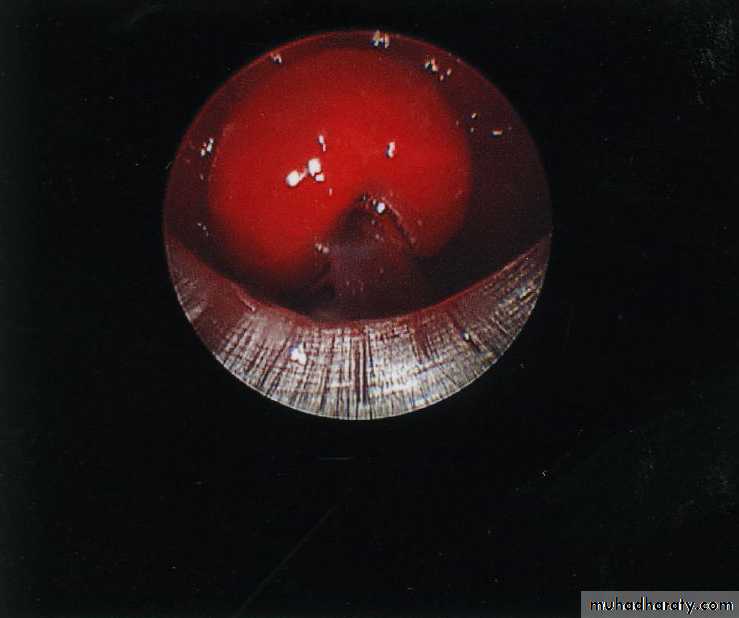

Diphtheric laryngitis
Secondary to pharyngeal diphtheria, caused by Corynebacterium diphtheriae.more common in childrean 10 yearsClinical features:
1-insidous onset2- sore throat
3- cough and hoarseness
4- srtidor inspiratory in nature
5- pyrexia and malaise
6- dyspnea and cyanosis in sever cases
7- on exam. : grayish-white to black membrane
Diagnosis:
Swab for culture and sensitivity
Treatment:
1- anti-toxin: 20000-100000 IU
2- antibiotics: penicillin
3- oxygen and tracheostomy in sever cases
Complications:
1- resp.obstruction
2- neurological: paralysis of soft palate, then mm. Of eye accomodation, then respiratory and limb muscles.
3- cardiac: cardiac arrest
Acute perichondritis
Inflammation of the laryngeal cartilage perichondrium.
Aetiology:
1- primary : blood-born
2- secondary to superficial infection in the larynx
3- radiotherapy: commonest cause
4- autoimmunity: SLE, rheumatoid disease
Clinical features:
1- develops slowly
2- dull pain over the entire laryngeal skeleton
-3 fever and malaise
4- resp.obstruction and cyanosis in sever cases
5- sometimes the cartilage is exposed with foul smell from the necrotic tissue.
Treatment:
1- broad spectrum antibiotics
2- steroids in high doses for one week
3- tracheostomy or itubation in sever cases
4- total laryngectomy in resistant cases.
Chronic laryngitis
Chronic non-specific laryngitisPrimarly affect middle aged men
Aetiology:
1- Exogenous
a- physical: vocal abuse
b- chemical: tobacco, alcohol, irritants and fumes
c- infection: sinusitis, rhinitis
2- Endogenous
a- shotr heavily-built males
b- DM
c- hypothyroidism
d- tense personality
e- reflux esophagitis
Clinical features:
1- Insidious onset
2- Hoarseness is the main feature, the voice is worse at the morning
3- Cough and sputum
4- On exam.: redness and edema of the mucosa, there might be white patches (leukoplakia) or polypoid lesion resembling malignancy.
Histopathology:
Squamous cell hyperplasia and keratosis. With or without atypia and carcinoma in situ in sever cases.
Malignant transformation : in long standing cases.
Treatment:
1- correct the underlying cause
2- careful follow-up
Chronic specific laryngitis
Tuberculous laryngitis:Secondary to open pulmonary TB (sputogenic) causedby Mycobacterium tuberculosis
Age: 20-40 years, males=females
Pathology:
Mostly involve the posterior parts of the larynx and arytenoid cartilages.The lesion could be ulcerative (undermined edge) or exophytic like a mass (tuberculoma)
Clinical features:
1- pain in the throat
2- cough productive of sputum
3- hoarseness
Diagnosis:
1- elevated ESR
2- endoscopy and biopsy
Treatment:
Anti-TB drugs : INH, rifampicin, streptomycin, para-aminosalycilic acid and ethambutol.