Pelvic injuries
Less than 5% of all skeletal injuries. With high incidence of associated soft tissue injuries, and
the risks of severe blood loss, shock, sepsis and Adult Respiratory Distress Syndrome.
Demands a combined approach by experts in various fields.
Range in severity from low energy, to life-threatening high energy unstable fracture patterns.
10% associated with visceral injuries, and the mortality is more than 10%
BASICS:
✴ Initial management of severe fractures should follow Advanced Trauma Life Support
protocols.
✴ Clear understanding of the anatomy of the pelvis and its related structures.
✴ Clear understanding of the definition of pelvic stability and instability.
Clinical assessment:
History and Mechanism of injury.
Mostly low energy falls, or high energy mechanisms such as motor vehicle accidents.
Associated with significant visceral injuries, concomitant multisystem trauma and
hemorrhage ( acute abdomen, bladder, rectal, urethral, scrotal, vaginal, prostate
injuries and vascular injuries).
During secondary survey of ATLS do comprehensive musculoskeletal examination.
Position and symmetry of lower extremities.
Look for the skin any open wounds, degloved skin, injury in the perineum.
Detailed neurological examination.
Investigations:
1-X-ray: Basic AP view
Five main views are available, AP, inlet view, outlet view and two oblique views.
2-CT scan
: is the best for assessment of the pelvic injuries.
3-Contrast studies
: are used for possible abdominal or urogenital injuries.
4- Angiography :
in severe shock to assess vascular injury.
!
1
Types of pelvic fracture:
There are 3 main types;
1. Isolated fracture with intact pelvic ring.
2. Fractures with broken ring which can be stable or unstable.
3. Fractures of the acetabulum.
4. Sacrococcygeal fractures.
Pelvic instability:
✴
Depends on Bony and ligamentous integrity.
✴
If the pelvis can withstand weight bearing loads without displacement, it is stable.
✴
A stable pelvic ring injury is usually defined as one that will (theoretically) allow full
weight bearing without the risk of pelvic deformity.
✴
Occasionally the decision on stability cannot be made until the patient is examined under
anaesthesia.
1. Isolated fractures:
Those are avulsion injury, direct injury or stress fractures.
❖
Avulsion by the Sartorius tendon causes fracture of the anterior superior iliac spine
(ASIS).
❖
Avulsion by the rectus femoris tendon causes fracture of the anterior inferior iliac spine
(AIIS).
❖
Direct injury cases direct fracture anywhere in the pelvis.
❖
All above are simple stable injuries that needs only bed rest for several days and
reassurance. .
❖
Stress fracture of the pubic rami may occur with Osteomalacia or osteoporosis.
2. Fractures of the pelvic ring:
❖
The pelvis is like a complete ring formed by the 2 hip bones and the sacrum they are
joined by the symphysis pubis anteriorly and the 2 sacroiliac joints with their strong
sacroiliac and iliolumber ligaments posteriorly.
❖
Anterior pelvic segment disruption may occur with disruption of symphysis pubis,
fracture of the body of the pubis, or both pubic rami fracture (single ramus fracture is an
isolated fracture without ring disruption).
❖
Posterior segment disruption can occur with fracture of the sacrum, iliac crest fracture or
complete sacroiliac joint disruption. Sometimes the joint is
only partially disrupted with
ligament injury.
❖
Disruption of the ring at one point usually associated with other point disruption which is
sometimes a partial one.
❖
Fracture of pelvic ring is said to be stable if there is single complete ring disruption only.
❖
Fracture of pelvic ring is said to be unstable if there is two or more complete ring
disruptions that can be anterior and posterior on the same side or on both sides.
!
2
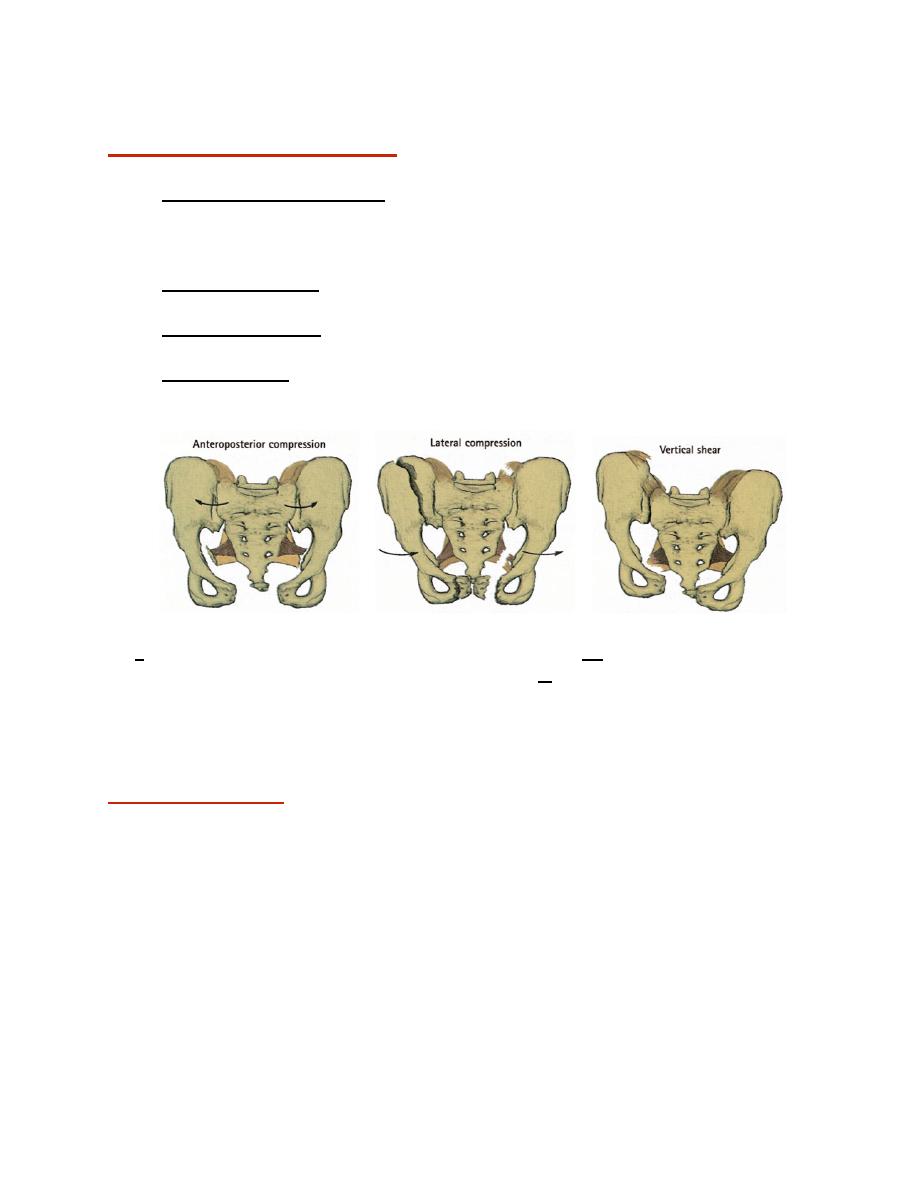
Mechanism of pelvic injury:
This can be one of the followings;
1. Anteroposterior compression: as the frontal force that may be caused by a car hitting a
pedestrian leading to complete disruption of the symphysis pubis (open book fracture) or
one side double pubic rami fracture, this is usually associated with only partial posterior
disruption it could be mostly stable or could be unusable unstable.
2. Lateral compression: side-to-side ring compression causing highly unstable fracture
with complete anterior and posterior disruptions.
3. Vertical shear injury: the hip bone of one side vertically displaced upwards causing
unstable fracture with both anterior and posterior disruptions on the same side.
4. Complex injury: it’s a combination of any of the above injuries which is highly serious
and associated with other system injuries.
!
(b)
!
(c)
!
a; anteroposterior compression injury with open book fracture; b; lateral compression force
with double rami fracture that may occur on both sides, c; vertical shear injury with complete
disruption of both anterior and posterior segments of one side.
Clinical features:
❖ With isolated fractures and stable injuries the patient is not severely shocked but has
pain on attempting to walk, there is localized tenderness but seldom any damage to
pelvic viscera.
❖ With unstable injuries the patient is severely shocked, in great pain and unable to stand;
he may also be unable to pass urine. There may be blood at the external meatus. One
leg may be partly anesthetic because of sciatic nerve or sacral root injuries. These are
extremely serious injuries, carrying a high risk of associated visceral damage.
!
3
Emergency treatment:
ATLS PROTOCOLS.
❖ As with all major injuries, the first priority is to ensure that the airway is clear and venti-
lation is unimpaired.
❖ Shock and blood loss should be treated immediately and throughout the period of
assessment. If the blood pressure cannot be restored, a diagnostic peritoneal aspiration
should be carried out to exclude intra-abdominal bleeding. Occasionally an emergency
laparotomy is necessary to deal with visceral injuries.
❖ If the patient cannot pass urine he must not be catheterized; gentle retrograde
urethrography is harmless and may show a urethral tear.
❖ Urogenital damage is particularly likely in bilateral pubic rami fractures. If the urethra is
ruptured, urinary drainage should be provided by suprapubic cystostomy.
❖ Temporary immobilization of the pelvis using external fixation or pelvic binders may
reduce shock and control bleeding.
Treatment of the fractures
1. UNDISPLACED RING FRACTURES:
These injuries can usually be treated by 4 weeks rest in bed. Throughout this
period exercises are encouraged.
2. DISPLACED FRACTURES WITHOUT SACROILIAC DISRUPTION:
❖ Disruption of the symphysis pubis (the ‘open book’ injury), if displacement is not marked
less than 2 cm, simply nursing the patient on his side for 6—8 weeks can reduce it. For
more severe degrees of displacement, or if Urogenital surgery is being done, external
fixation is better. The fixator is retained for 6—8 weeks but the patient can get up and
walk around.
❖ Pubic rami fractures, these are usually due to lateral compression. If displacement is not
severe, bed rest and leg traction for 3—6 weeks will be enough. For severe
displacement, external fixation provides more stability.
3. DISPLACED FRACTURES WITH SACROILIAC DISRUPTION:
❖ All vertical shear injuries, and some of the more severe compression injuries, disrupt the
sacroiliac joint or produce unstable fractures around the joint. The fracture or dislocation
must be stabilized, either by internal fixation anteriorly with plates and screws and
posterior fixation with screw through open or percutaneous fixation or by combined
external fixation anteriorly and posterior sacroillaic fixation and prolonged rest in bed (8
—12 weeks).
!
4
!
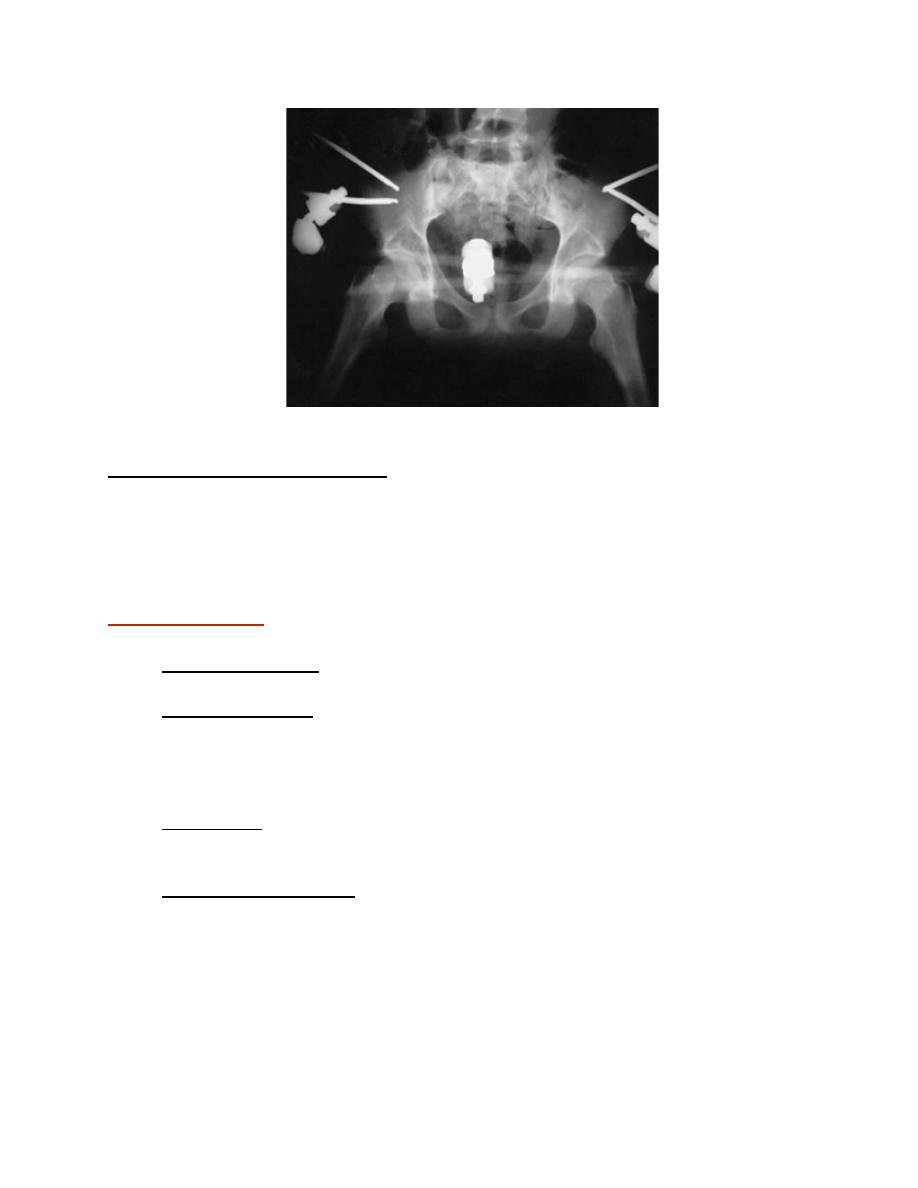
Figure shows external fixation of pelvis
4.OPEN PELVIC FRACTURE:
Treated by wound debridement and external fixation. A diversion colostomy may be
necessary.
Complications:
1. Thromboembolism: DVT or pulmonary embolism. Anticoagulation should be
considered in pelvic injuries especially when there are risk factors.
2. Urogenital damage: Compression fractures are the usual cause of Urogenital tract
damage; also with all pelvic ring disruptions, damage must be excluded. It needs
adequate urinary drainage, which is accomplished by suprapubic cystostomy. Definitive
repair of can he delayed while the patient’s general condition improves. Urethral injuries
sometimes result in stricture, incontinence or impotence.
3. Nerve injury: Displacement of the sacroiliac joint or fracture of the sacrum may injure
the Lumbosacral plexus. The damage is usually permanent and some weakness will have
to be accepted.
4. Persistent sacroiliac pain: this is fairly common after unstable pelvic fractures and may
occasionally indicates arthrodesis of the sacroiliac joint.
!
5