


Subarachnoid Hemorrhage(SAH)
An Intracranial Hemorrhage which has occurred primarily into the subarachnoid space of the basal cisterns, the most likely cause being intracranial aneurysm.Incidence:
22.5 cases /100,000 populations
Risk factors
- >50 y (40-60y most common range of age)
- Female depending on hormonal status
- Hypertensive patients
- Cigarette smoking, alcoholic, cocaine or any sympathomimetics agents' user
- Prior history of SAH from separated aneurysm or family history of SAH( Between five and 20% of patients with SAH have a positive family history)
Etiological factors
- 50% aneurysmal Hemorrhage- Trauma
- Rupture AVM
- Hypertension
- Blood dyscrasias, Anticoagulant drug
- Malignant brain tumor
- Unknown cause
Clinical feature
- Sudden sever headache
- Sudden loss of consciousness (25% of the patients not recover)- Focal neurological deficit ex: (hemiplegic or dysphasia) which occurs either due to acute disturbance of an eloquent part of brain or direct pressure of aneurysm on adjacent structures.
- Neck stiffness, photo phobia, seizure vomiting which all occurs due to meningeal irritation
- Vasospasm (3 days – 3 wk) after Hemorrhage usually fatal due to irritation of vessel wall by blood products
- Second fatal hemorrhage (40%) within 6 weeks
Management
Objective: - improve chance of survival-prevent 2nd fatal hemorrhage.
40% death if hemorrhages occur from 2nd – 5th weeks after hemorrhage
- Good outcome:
-younger age
- Good neurological status (especially level of Consciousness)
-interval since hemorrhage (the longest the best)
-absence of Hypertension, arterial spasm, significant Cardiac and pulmonary diseases.
-site, configuration & relationships if aneurysm is the cause.
Confirmative Investigations: -
Lumbar puncture
in the absence of rise ICP
Xanthochromia in supernatant fluid.
C.T scan and C.Tscan angiography:
* demonstrate site of hemorrhage in relatively well patients.
* Size of hematoma in poorly condition patients.
* In the 1st 24 h .sensitive up to 97%
* can detect lumen thrombosis &wall calcification if the cause was an aneurysm.
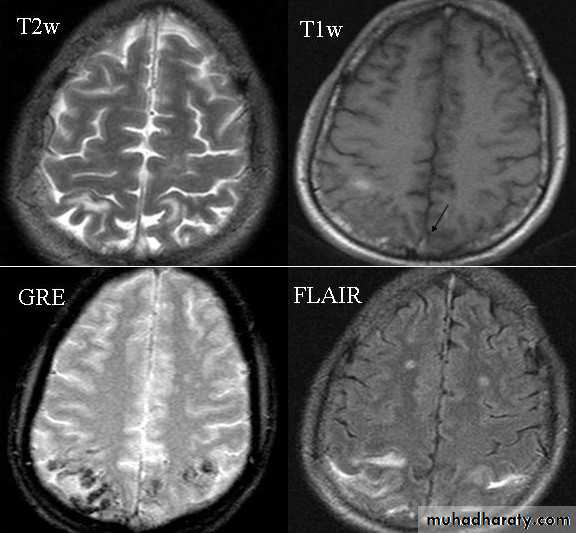
MRI:
* Initial diagnosis of SAH* detect completely thrombosed aneurysm
* limited in acute cases
4- Vessels arteriography (carotids& vertebrales)
* can be used when C.T scan& MRI were negative.* After exclusion of medical cause of hemorrhage.
*deferred in patients who remain unconscious.
line of management
NursingContinuous observation (Glasgow Coma Scale, temperature, ECG monitoring, pupils, any focal deficits)
Nutrition
Oral route preferred, but only with intact cough and swallowing reflexes
If nasogastric tube is necessary:
Deflate endotracheal cuff (if present) on insertion
Confirm proper placement by X-ray
Begin with small test feeds of 5% dextrose
Prevent aspiration by feeding in sitting position and by checking gastric residue every hour
Tablets should be crushed and flushed down (phenytoin levels will not be adequate in conventional doses)
Total parenteral nutrition should be used only as a last resort
Keep stools soft by adequate fluid intake and by restriction of milk content; if necessary add laxatives
Blood pressure
Do not treat hypertension unless there is evidence of progressive organ damageFluids and electrolytes
Intravenous line mandatoryGive at least 3 l/day (normal saline)
Insert an indwelling bladder catheter if voiding is involuntary
Compensate for a negative fluid balance and for fever
Monitoring of electrolytes (and leucocyte count), at least every other day
Pain
Start with paracetamol and/or dextropropoxyphene; avoid aspirin
Midazolam can be used if pain is accompanied by anxiety (5 mg intramuscularly or infusion pump)
For severe pain, use codeine or, as a last resort, opiates
Prevention of deep vein thrombosis and pulmonary embolism
Before occlusion of aneurysm: apply compression stockingsAfter treatment of the aneurysm: fractionated heparin
Medical treatment to prevent secondary ischaemia
Nimodipine 60 mg orally every 4 h; to be continued for 3 weeks
- 3-H THERAPY
- Oxygenation (Hyperventilation)- optimize cerebral perfusion (Hydration)
- control ICP .blood pressure & seizure (Hypertension)
Indication for surgery
- Aneurysm either by clipping, coiling- AVM obliteration the feeders either by clipping or flow diversion or injection of Embolizing agents.
- Brain tumor according to the type, site, size, age of the patient.
Causes of poor clinical condition on admission
Early rebleeding
Intracerebral haematoma
Acute subdural haematoma
Global cerebral ischaemia
Acute hydrocephalus