GIT radiologysmall intestine
Dr. Khaleel IbraheemMBChB, DMRD,CABMS-RAD
Ba follow through
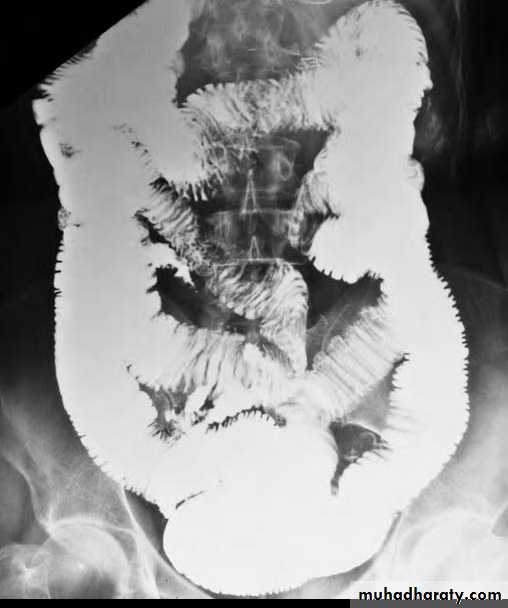
The standard contrast examination is barium follow-through (that involves drinking 200-300 ml of barium then taking films at regular intervals until the barium reaches the colon). It may take 2-3 hoursNormal barium follow-through
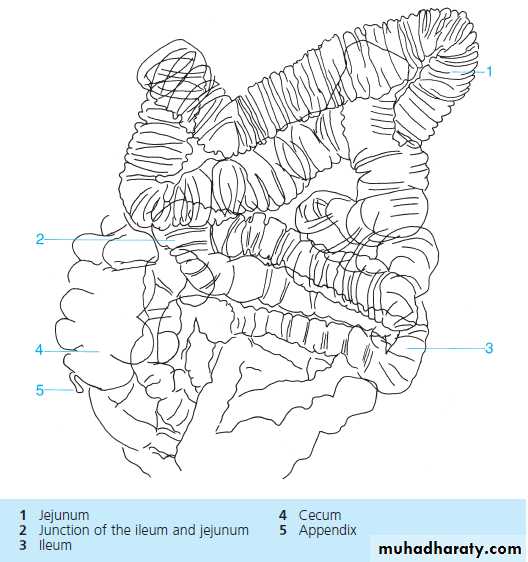
The barium forms a continuous column defining the diameter of bowel (< 25 mm). Transverse mucosal folds appear as lucent filling defects of about 2-3 mm in width. When the SB is contracted, their appearance is described as feathery. The folds are largest & numerous in jejunum & tend to disappear in the lower parts of ileum.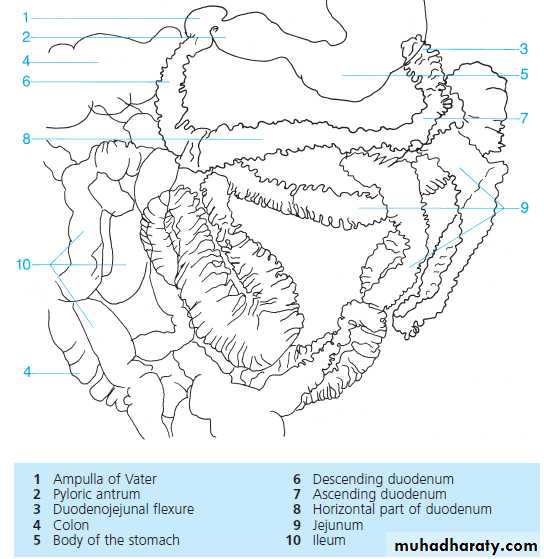

enteroclysis
Alternatively, small bowel enema (enteroclysis) is other contrast procedure (that distends the bowel with excellent mucosal detail), but it involves intubation with nasoduodenal tube through which barium is injected that is followed by water or methylcellulose to propel barium through the bowel
CT & US can show bowel wall thickening (sign of inflammatory bowel diseases & lymphoma). CT can show mucosal irregularity & neoplasms


Indication of Ba follow through
1. Inflammatory bowel diseases.2. Suspected stricture.
3. Malabsorption.
4. Assess bowel length after surgical resection.
5. SB obstruction.
6. Malrotation.
Abnormal signs in contrast examinations
A. Dilatation: > 30 mm. The folds are effaced & the valvulae conniventes become clearly visible.1. Malabsorption.
2. Paralytic ileus.
3. SB obstruction.
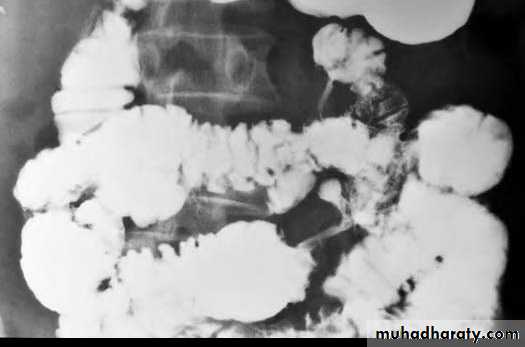
Multiple dilated small bowel loops are present. The valvulae conniventes
are thin and straight and closely stacked together.
cont
B. Diffuse Mucosal abnormality (fold thickening)Occurs in many conditions e.g.
-malabsorption,
-oedema,
-hemorrhage,
-Inflammation
-And infiltration of the SB wall.

thickened folds with separation of the loops
Focal segmental fold thickening
1. Ischemia
2. Intramural hemorrhage3. Adjacent inflammatory process (appendiceal or pelvic
abscess)
A loop of abnormal small bowel is seen in the pelvis. The lumen is slightly narrowed with thick, straight folds
C. Narrowing (other than peristalsis)
1. Cohn's disease.
2. TB.
3. Lymphoma
Peristalsis is smooth, concentric, transient with normal mucosal folds, while strictures don't contain normal mucosal folds & cause proximal dilatation.


Normal peristalsis
D. Ulceration SB outline is smooth apart from indentation of mucosal folds. Ulcers appear as spikes projecting outwards which may be shallow or deep.1. Crohn's disease.
2. TB.
3. Lymphoma.
Ulceration + mucosal oedema may give the appearance of cobblestone.


Small bowel diseases
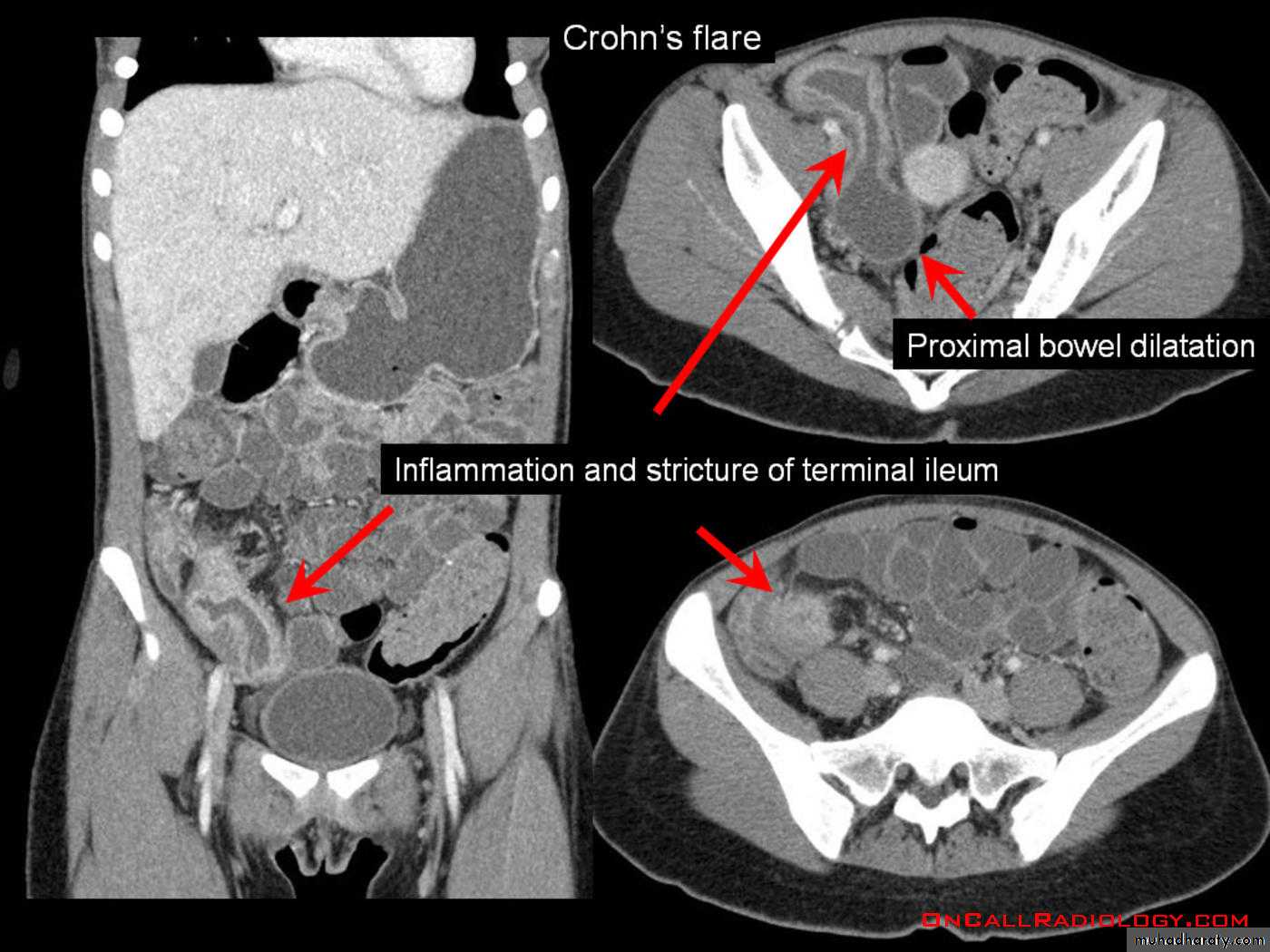
1.Crohn's diseaseis a disease of unknown etiology characterized by localized areas of chronic granulomatous inflammation which Nearly always affects the terminal ileum, it may also affect several parts (skip lesions) of SB & LB with normal intervening parts.
Radiological findings
Main signs are strictures & mucosal irregularitya. The strictures (string sign) are variable in length (due to spasm of ulcerated loop or due to oedema & fibrosis of bowel wall) with proximal dilatation. When there is obvious disease of terminal ileum, the caecum may be contracted.

A long segment of narrowed ileum (string sign) is present with proximal ileal dilation& caecal contraction
TI
caecum
Two regions of high-grade stenosis are present in the proximal
small bowel.b. Ulcers may be deep +/- cobblestoning

Multiple discrete ulcerations are present in the distal small bowel.
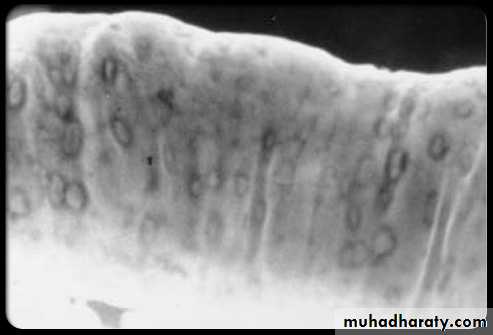
The central barium collections (ulcer crater) and mounds of edema are characteristic of aphthous ulcers.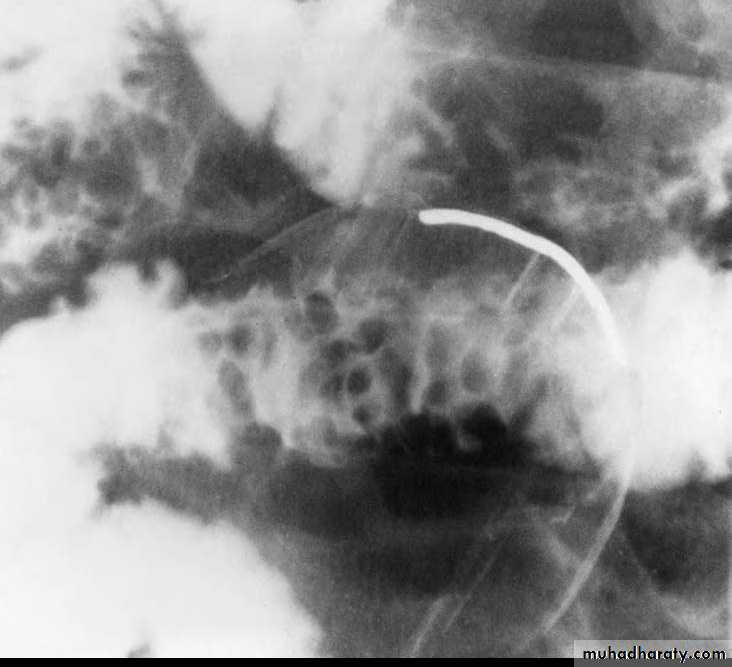
A cobblestone mucosal pattern affects a nonstenotic segment of small bowel
c. Due to bowel wall thickening, the folds may be thickened, distorted or disappear & the loops may be separated in severe wall thickening. With inflammatory mass, greater displacement of loops is seen.
Mucosal fold thickening, ulceration, nodularity, asymmetric bowel wall
involvement, regions of narrowing, and separation of small bowel loops are present.d. Fistulae to the other loops of SB, colon, bladder or vagina.
e. Signs of malabsorption may be seen.
2. Tuberculosis
Commonly affects ileocecal region & causes cecal contraction & can not be differentiated from Crohn's disease.

3. Lymphoma Is often difficult to be distinguished from Crohn's disease on Ba examination.
There may be small mucosal filling defects (due to tumor nodules) & displacement of loops by LAP.
Hepatosplenomegaly may be present.
CT & US may show wall thickening. CT can show mesenteric LAP, hepatic & splenic deposits.

follow-through (spot radiograph).
An intraluminal polypoid mass is present within the smallbowel. Small bowel

A long segment of terminal ileum is involved with multiple submucosal, polypoid filling defects. The lumen is increased in diameter
4. Malabsorption:
Definitive diagnosis is done by jejunal biopsy.Radiological signs:
a. SB dilatation (mostly jejunal) in case of celiac disease

Celiac disease: The jejunum is devoid of most of its normal mucosal markings with Ileal loops in the pelvis have a prominent fold pattern
b. Thickening of mucosal folds.
c. Dilution of barium.d. signs of the causative abnormality (e.g. Crohn's disease, lymphoma, anatomical abnormalities)
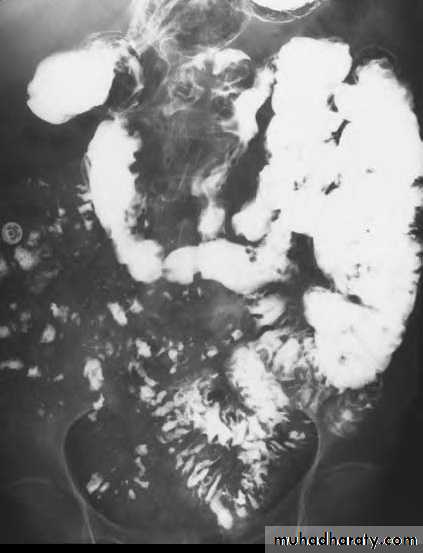
Celiac disease:
Flocculation and segmentation of barium indicate the presence of excessive fluid in the distal small bowel. The normal jejunal fold pattern also isabsent. These loops appear featureless. A few small bowel loops in the pelvis have thickened folds.
Decreased SB length (surgical resection, fistula short-circuiting a length of SB) can cause malabsorption.
Stagnation of SB contents as in multiple diverticulae, blind loop syndrome, stagnant loop (proximal to stricture)also cause malabsorption

Multiple large saclike structures project from multiple small bowel loops
5. Acute SB obstruction
The diagnosis is clinical with plain film findings & in most cases; there is no need for barium examinationA contrast examination (water soluble contrast is preferred) is performed if the cause of obstruction is not evident. If the contrast is seen within the colon at 24 hours, conservative management is likely to be useful. If not, there is mechanical obstruction.
CT is used in selected cases to demonstrate the site of obstruction by showing the transition between dilated & normal bowel & also to confirm or exclude a mass at the site of obstruction.