1
First stage
Anatomy
Lec-2
8/12/2015
.ا
.د
ع
بدالجبار
THE AXILLA (Arm pit )
Is a pyramidal space between the upper part of the arm & the lateral thoracic wall.It has
4 walls (anterior,posterior,medial & lateral ), apex & base.The apex is pointed upward in
the direction of the root of the neck (to receive the brachial plexus) & communicates with
the superior aperture ( Inlet of thorax) of thorax to receive the axillary artery ( continuity
of subclavian artery).The apex is known as Cervico-axillary canal & has bony boundaries
which are :
1-The clavicle anteriorly.
2-Outer border of the first rib medially
3-Upper part of the scapula posteriorly
It allows the passage of the Neuro-vascular bundle( brachial plexus & Axillary artery) to
the upper limb .
The base : Is formed by skin & superficial fascia of the axilla,it is concave when the limb
is beside the trunk & becomes flat & straight on raising and abducting the limb due to
suspensory ligament of the axilla.
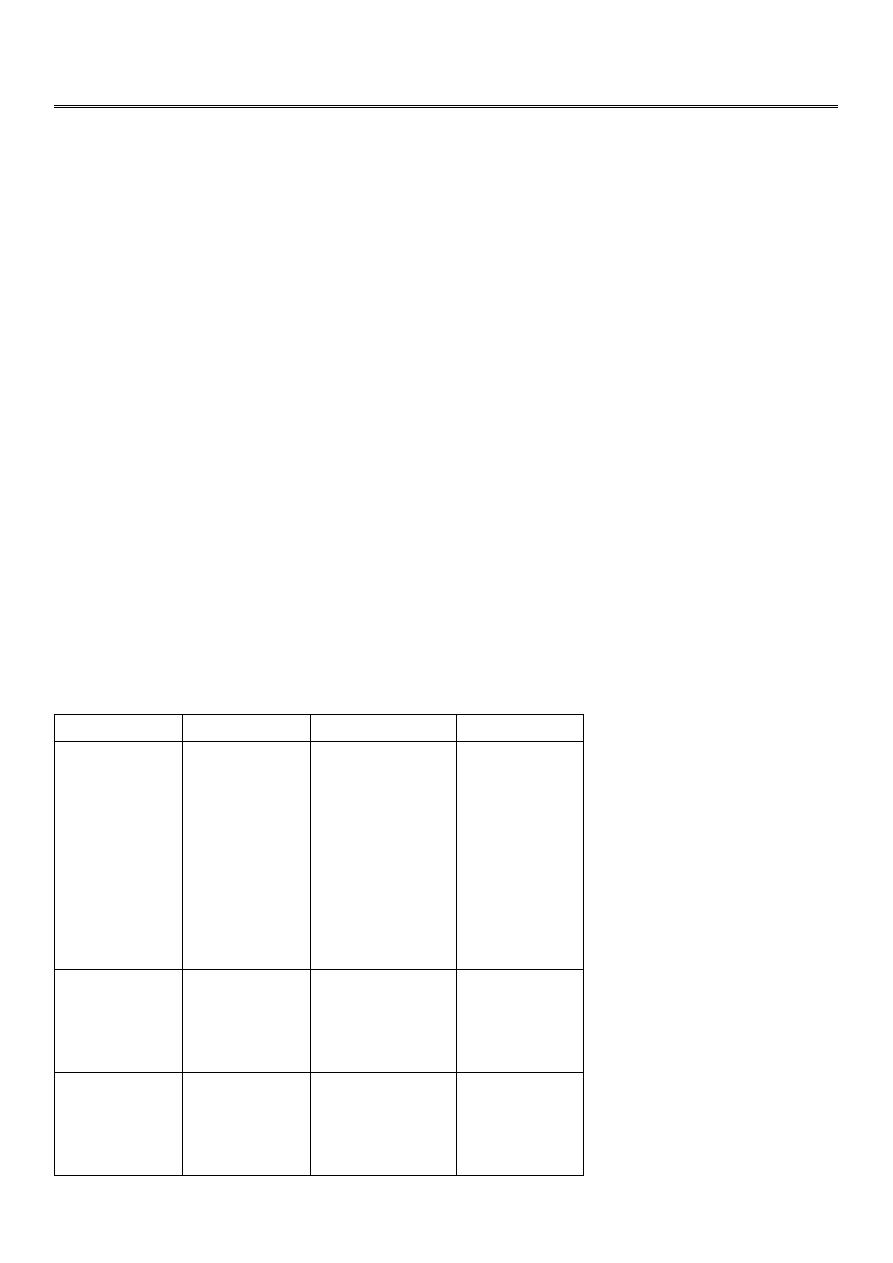
The anterior wall is formed by the clavicle, 3 muscles ( pectoralis major & minor Ms in
addition to the subclavius M ) and the Clavi-pectoral fascia
Muscle
Origin
Insertion
Nerve supply
Pectoralis
Major
1-Side of
sternum
(sternal)
2-
Medial 2 /3
of anterior
Border
of
clavicle
(Clavicular
head)
outer lip of
the
intertubercular
groove
Medial
&
lateral
pectoral Ns
Pectoralis
minor
from 3
rd
– 5
th
ribs
Near
their costal
cartilages
Coracoid
process
of
scapula
medial
pectora
Subclavius
from costal
cartilage of
the first rib
subclavius
groove
on
inferior surface
of clavicle
N.
to
subclavius

2
The clavipectoral fascia: Is part of the deep fascia attached to the clavicle,it encloses the
subclavius M,then descends down ward deep to pectoralis major & enclosing pectoralis
minor M & ends as suspensory ligament of the axilla.It is pierced by the following
structures:
1-Lateral pectoral nerve.
2-Cephalic vein .
3-Pectoral branch of thoracoacromial artery.
4-Some lymphatic vessels.
The lateral border of pectoralis major M forms the anterior fold of the axilla.
The posterior wall of the axilla is formed by 3 muscles, these are subscapularis, teres
major & latissimus dorsi Ms.The posterior fold by latissimus dorsi & teres major Ms
Subscapularis takes origin from the subscapular fossa& inserts into the lesser tuberosity
of the humerus.It is innervated by upper & lower subscapular nerves ( from post.cord ).
Teres major takes origin from posterior surface of lateral border of scapula near the
inferior angle & is inserted in to the medial lip of intertubercular groove.It is innervated
by the lower subscapular nerve .
Latissimus dorsi takes origin from the following sites:
A- Spines of T 7 __T 12 vertebrae.
B- Thoracolumbar fascia.
C- Iliac crest of the Hip bone.
D- Inferior angle of scapula
The muscle is inserted into the floor of intertubercular ( Bicepital0 groove & is innervated
by the middle subscapular ( Thoracodorsal ) nerve.
The medial wall is formed by the upper 4-5 ribs,their intercostal spaces& the upper part
of serratus anterior muscle covering them,which arises from the outer surfaces of upper
8-9 ribs& is inserted into the anterior aspect of the medial(vertebral ) border of the
scapula.It is innervated by the long thoracic nerve( C 5—C 7).
The lateral wall is formed by the intertubercular ( Bicepital ) groove containing the
corachobrachialis M & short head of Biceps..

3
The Contents of the Axilla
1-The axillary vessels: The axillary artery,starts as the continuity of the subclavian artery
at the outer border of the first rib& ends at the lower border of teres major M( the lower
limit of the axilla),where it continue as the Brachial artery.It is crossed by the pectoralis
minor M ,which divides it into 3 parts.The first part between outer border of first rib &
the upper border of pectoralis minor M( it gives a single branch known as highest thoracic
or superior thoracic A ).The second part lies behind pectoralis minor M& is related to
the 3 cords of the brachial plexus* laterally to lateral cord, medialy to medial cord &
posteriorly to the posterior cord) ,while anteriorly it is related to pectoralis minor M.It gives
2 branches, the thoracoacromial & lateral thoracic .The thoracoacromial gives 4 branches
,2 of them to bones ( acromial & clavicular) & other 2 to muscles (Deltoid & pectoral
branches).While the lateral thoracic branch descends to the side of the chest wall to
accompany the long thoracic nerve within the substance of serratus anterior muscle..
The third part of the axillary artery extends from lower border of pectoralis minor to
lower border of teres major muscle,where it continues as the Brachial artery,it is related
to the derivatives of the 3 cords of the brachial plexus & it gives 3 branches these are
subscapularis ( bifurcates into thoracodorsal & circumflex scapular branches ) ,anterior &
posterior circumflex humeral arteries around the surgical neck of the humerus.
2-The Brachial plexus:It is formed by the ventral rami of lower 4 cervical nerves & the
ventral ramus of the first thoracic nerve.The first stage is roots arrangement to form
trunks ( C 5& 6
th
form the upper trunk , C 7 alone forms the middle trunk,while C 8 & T 1
form the lower ( inferior ) trunk.
The second stage is the splitting of each trunk to form anterior & posterior divisions.
The third stage is the formation of the 3 cords by the Re-union of these divisions.The
posterior divisions of the 3 trunks unite to form the posterior cord,the anterior division of
the upper & middle trunks unite to fornm the lateral cord,while the anterior division of
inferior trunk forms the medial cord of the brachial plexus.
The last stage is the derivatives of each cord as follows:
The posterior cord gives off:
1-Upper subscapular.
2-Middle subscapular ( Thoracodorsal ).
3-Lower subscapular .
4-Axillary nerve.
5- Radial nerve.

4
The letral cord gives the following derivatives:
1-Lateral pectoral nerve.
2-Musculocutaneous nerve.
3-Lateral root to median nerve.
The medial cord gives:
1-Medial pectoral nerve.
2-Medial cutaneous of Arm.
3- Medial cutaneous of forearm.
4-Ulnar nerve.
5- Medial root to median nerve.
In addition to these derivatives ,the upper trunk gives 2 branches suprascapular & nerve to
subclavius muscle,while the roots gives dorsal scapular & long thoracic nerve) C5-7)
3-The axillary lymph nodes which are arranges in the following groups:
A-Anterior ( pectoral ) group,under anterior border of pectoralis major M.
B-Posterior ( subscapular ) group along the course of subscapular vessels.
C-Central group within the loose areolar tissueof the base of the axilla.
D-Lateral group along the course of the axillary V near bicipital groove.
E-Medial group along the course of lateral thoracic vein.
F-Apical group in the apex of the axilla,it receives lymphatics from the above groups &
takes them ( direct them ) to the deep cervical nodes in the root of the neck.
THE BREAST:
Is rudimentary in male & well developed in the female specially in lactating woman.It is a
modified sweat gland located under the superficial fascia covering the pectoral region&
lying on the deep fascia covering pectoralis major & part of the serratus anterior Ms.It
extends from the sde of the sternum medially to the anterior axillary fold laterally( part of it
extends into the axilla as axillary tail of the breast),while supero-inferiorly it extends from the
level of 2
nd
rib to the 6
th
rib.The gland consists of 15-20 lobes extending from the periphery
of the gland to the area near the nipple.Each lobe has its own duct( lactiferous duct) which
opens externally in to the nipple( has about 15-20 openings).The nipple is a small conical
projecting part surrounded by a lighter area ( Areola).The breast is supplied by:
5
1-Pectoral branch of thoracoacromial artery.
2-Mammary branches from the lateral thoracic artery.
3-Perforating branches from the internal thoracic artery(i.e internal mammary A ).
4-Branches from intercostal arteries for the spaces 3
rd
-5
th
.
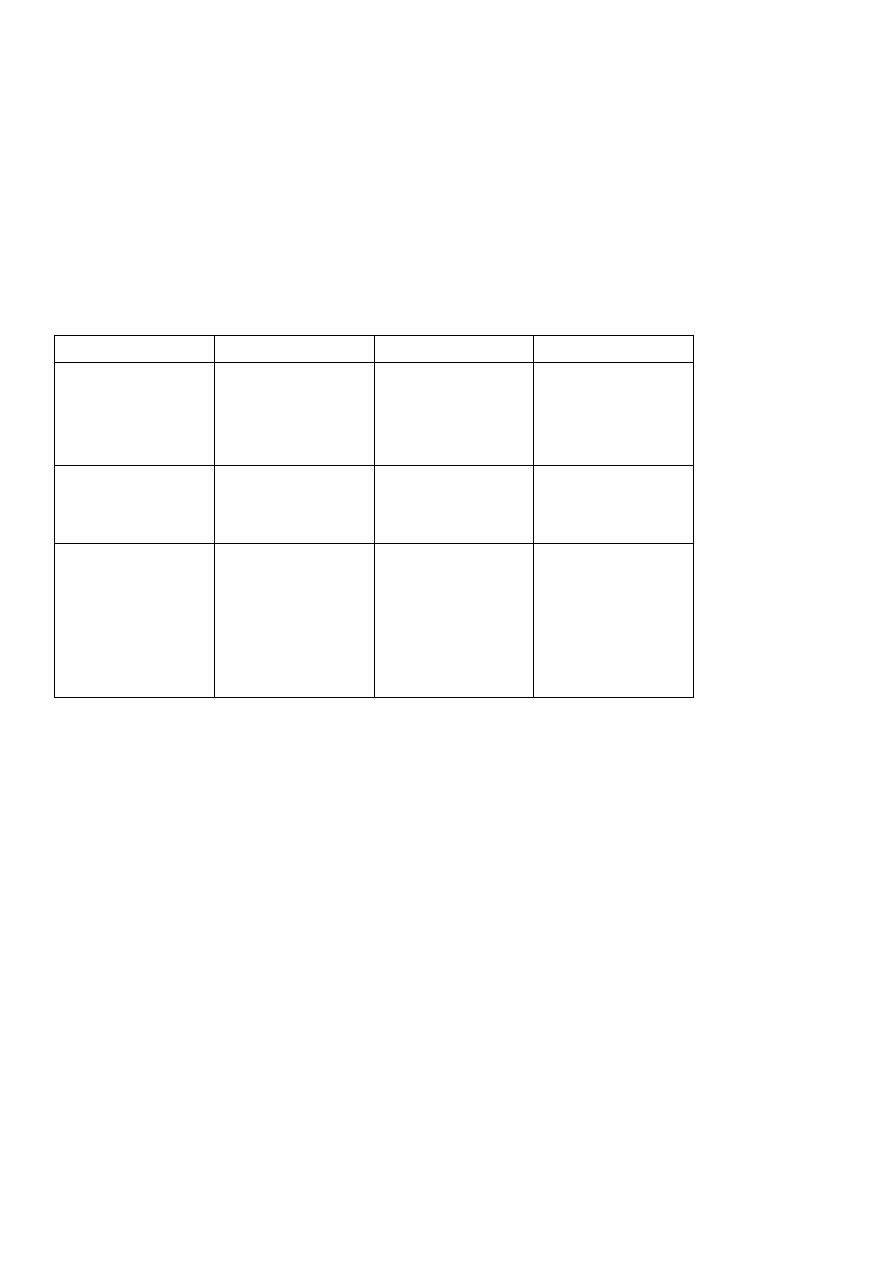
Rotater Cuff Muscles: are 4 in number surrounding the capsule of the shoulder joint to
support &share in stabilizing the shoulder joint.One of these Ms inserts into the lesser
tuberosity ( Subscapularis ),the other 3 are inserted into the greater tuberosity (
Supraspinatous,infraspinatous & teres minor muscles)
Muscle
Origin
Insertion
Nerve supply
Supraspinatous from
supraspinous
fossa Of the
scapula
into the superior
facet
of
the
greater
tuberosity
Suprascapular N
Infraspinatous
from
infraspinous
fossa
middle facet of
greater
tuberosity
Suprascapular N
Teres minor
from posterior
aspect of lateral
Border
of
scapula
just
above the origin
of teres major
inferior facet of
= = =
Axillary N
The muscles responsible for Abduction movement of the arm at shoulder joint are:
1- From 0 – 18 degree by Supraspinatous muscle.
2- 18—90 degree by Deltoid muscle(innervated by the Axillary nerve ).
3- Beyond 90 degree & above the head is by Trapezius & Serratus anterior muscles.
The muscles attaching the limb to the back are by Trapezius,Rhomboid minor,Rhomboid
major, Levaetor scapula & Latissimus dorsi.
The latissimus dorsi id active during swimming , climbing, rowing ,pulling & scratching the
opposite scapular region.
The Trapezius takes origin from the following sites:
a-From medial third of the superior nuchal line.
b-From ligamentum nuchae.
c-From the spine of C 7 vertebra
d-From spines of T1 –T 12 vertebrae( T = Thoracic ).
6
The M is inserted into the front of lateral third of the clavicle,acromion process & upper
lip of the spine of the scapula.It is innervated by the spinal root of accessory nerve( 11
th
cranial nerve)which is motor ,while proprioception sensations from C4 & C5 nerves.
Levaetor scapula takes origin from transverse processes of upper 4 cervical vertebrae.
It is inserted in the area around the superior angle of scapula..
It is innervated by dorsal scapular nerve from the ventral ramus of C 5.
Rhomboideus minor takes origin from the spines of C 7 & T 1 vertebrae.
It is inserted into dorsal aspect of vertebral border of scapula at the base of the spine.
Is innervated by dorsal scapular nerve.
Rhomboideus major arises from the spines of T 2 – T 5 vertebrae.It is inserted into dorsal
aspect of vertebral border below the base of the spine till inferior angle of scapula &
being innervated by dorsal scapular nerve.
The last 3 Ms are known collectively as Elevators of the scapula( one of them is levaetor
scapula)& all the 3 has a common nerve supply( dorsal scapular nerve) and all the 3 has a
common action i.e all of them work in elevating the scapula.
The Deltoid M takes origin from the same areas of the insertion of the trapezius M .Thus
it arises from the inferior aspect of the crest of spines of scapula,acromion process&
lateral third of the clavicle.The M fibers from the 3 sites of origin converted into a single
tendon of insertion & being inserted into the Deltoid tuberosity( on the lateral aspect of
the middle part of the humerus).The deltoid is supplied by the Axillary nerve& its main
action is flexion of arm at shoulder joint( anterior fibers),extension of the arm ( posterior
fibers)& abduction of the arm at shoulder ( middle fibers) & in fact it is considered as
powerfull & main abductor M of the arm( from 18-90 degree).Thus if the Axillary nerve is
injured or compressed by local haematoma due to fracture at the surgical neck of the
humerus,abduction becomes impossible because of loss of innervation of the deltoid
M.8-90 degree).Thus if the Axillary nerve is injured or compressed by local haematoma
due to fracture at the surgical neck of the humerus,abduction becomes impossible
because of loss of innervation of the deltoid M.

7
Compartment of The Arm
The arm is surrounded by deep fascia which sends 2 septae attaching to medial & lateral
compartments,an anterior ( B.B.C muscles which are flexors at the Elbow joint),these Ms are
Biceps brachi,Brachialis & Coracobrachialis.The posterior compartment is an Extensor
compartment at the Elbow joint mainly Triceps M & lower down a small M (Anconeus M ).
The anterior compartment Ms are innervated by Musculocutaneous N ( from lateral cord).
The Biceps takes origin from 2 sites,long head from supraglenoid tubercle of the
scapula,while the short head takes origin from coracoid process of scapula in common origin
with the Coracobrachialis muscle,then the 2 head leads to a common belly of the muscle
before going to insert ( by a single tendon) into the radial tubercle of the radius bone.Biceps
is a powerfull supinater of the forearm in addition to flexion at the Elbow joint.
The Brachialis M takes origin from the anterior surface of the lower part of the shaft of the
humerus& its insertion into the front(anterior surface) of Coronoid process of the Ulna
bone.It is a flexor at Elbow joint along with the Biceps M.
The Coracobrachialis M takes origin from the Coracoid process of the Scapula in common
with the short head of Biceps M& is being inserted on the medial aspect of upper part of the
shaft of the humerus.
Note: As the tendon of Biceps passes through the front of Elbow(Cubital fossa) in its way to
its insertion site,it sends a flat ribbon like aponeurosis medially & superficially to cover the
terminal part of the brachial A+ the Median nerve known as Bicepital Aponeurosis.
The three B.B.C muscles are supplied by musculocutaneous nerve ( from lateral cord ).It is
motor to the 3 Ms & sensory to the skin on the lateral side of the F.A,where after supplying
motor to the 3 Ms of anterior compartment of Arm,it will continue as lateral cutaneous nerve
to the forearm.
The Sensory Nerve supply of the Arm
1-Medial cutaneous nerve of Arm from the Medial cord of the Brachial Plexus.
2-Upper lateral cutaneous of of Arm from the Axillary nerve.
3-Lower lateral cutaneous nerve of Arm from the Radial nervewhile runnibg in the spiral (
Radial ) groove on the back of the shaft of the Humerus.
4-Posterior cutaneous nerve of Arm from Radial nerve as it descends through the Axilla.

8
The Sensory Nerve Supply to The Forearm
1-Medial cutaneous of F.A from the medial cord of the Brachial plexus.
2-Lateral cutaneous of F.A from Musculocutaneous nerve.
3-Posterior cutaneous of F.A from the Radial nerve as it runs in the spiral groove.
Note: The anterior compartment contains the followings:
1-The 3 Ms i.e B.B.C .
2-The Brachial Artery.
3-Three nerves i.e the Musculocutaneous,Median & Ulnar nerves
The Musculocutaneous nerve motor component is only to the 3 Ms of the anterior
compartment ,while both the Median & Ulnar are not supplying any structure in the
Arm,these 2 nerves just passing through the anterior compartment to reach their areas of
destination( supply) in the F.A & the Palm of the Hand.
The Ulnar nerve runs in the anterior compartment,then inters the medial intermuscular
septa( leave the arm ) to reach the F.A by passing behind the medial Epicondyle of the
humerus( i.e bypassing the cubital fossa),then it passes through the 2 heads of origin of flexor
carpi ulnaris M of the F.A.
The Median nerve is formed on the anterolateral aspect of the beginning of the brachial
A,then it becomes on the lateral side of the upper third of the Brachial A,then crossing
obliquely in front of the middle third of the A ( from lateral to medial ) to becomes on the
medial side of the lower third of the Brachial A& then both the terminal part of the Brachial
A + the Median nerve are sheltered by Bicepital aponeurosis within the Cubital fossa.
The Posterior Compartment of The Arm
It contains mainly the Triceps M + the Radial nerve & Profunda Brachi A ,and just inferiorly
near the back of the Elbow joint, there is a small superficially placed slightly triangular muscle
known as Anconeus.
Triceps origin : The long head from infraglenoid tubercle of the scapula,the .The lateral head
from posterior aspect of the shaft of the Humerus above the spiral groove,while the Medial
head takes origin from the back of the humerus below the spiral groove & slightly from the
medial side of the Humerus.Thus the spiral groove separates the lateral head from the
medial head of the Triceps.The muscle fibers of the 3 heads of origin converge inferiorly into
a single tendon which is inserted into the top of the Olecranon process of the Ulna bone.The
M is supplied by many branches from the Radial nerve at different levels& it is a powerfull
Extensor muscle at the Elbow joint.

9
The Intermuscular Spaces
There are 2 main Triangular spaces, a superior horizontal one between teres minor ( above
), teres major ( below )& the Surgical neck of the Humerus laterally.This space is divided by
the long head of Triceps into a smaller triangular space medially ( between teres minor,teres
major & long head of Triceps)which transmits the Circumflex scapular branch of the
Subscapular artery & a lateral Quadriangular space bounded by teres minor above,teres
major below,long head of Triceps mediall and the Surgical neck of the Humerus laterally.This
Quadriangular space transmits the Axillart nerve & posterior circumflex humeral A.The
Axillary nerve as it passes through this space ,it divides into anterior & posterior divisions.The
anterior division supplies the major part of the Deltoid M,while the posterior division supplies
teres minor,the remaining part of the Deltoid and then continues as upper lateral cutaneous
nerve of the Arm ( i.e supplies the skin on the upper lateral part of Deltoid.
The inferior vertical Triangular space between teres major ( above ),long head of Triceps (
medially ) & the side of the Humerus.It transmits the Radial nerve & Profunda Brachi A (a
branch from the Brachial A ).
The Cubital Fossa
Is a triangular depressed space in front of the Elbow joint.It is bounded by the Pronater teres
medially,brachioradialis laterally,its base is formed by an imaginary line joining the 2
epicondyles of the humerus&its apex is formed as brachiradialis M crosses over the pronater
teres .The floor is formed by the insertion of Brachialis M & the supinater M below it,while
its roof is formed by the skin & fascia.The contents includes 2 groups as follows:
A-The superficial contents are :
1-Median cubital vein joining the Cephalic & Basilic veins.
2-Lateral cutaneous nerve of the F.A laterally.
3-Medial cutaneous nerve of F.A medially.
4-Bicepital Aponeurosis .
5-Some superficial lymphatic vessels & lymph nodes.
B-Deep group of structures includes :
1-The termination of the Brachial A & its bifurcation into Radial and Ulnar As.
2-The Median nerve just medial to the terminal part of the Brachial A.
3-Tendon of Biceps Brachi in its way to reach its insertion site.
4-Radial nerve laterally emerging in the groove between Brachialis & Brachioradialis.

11
THE BRACHIAL ARTERY
Is the direct continuity of the Axillary artery at the lower border of Teres major M ,it runs in
the anterior compartment of the Arm & ends opposite the Neck of the Radius bone ( in the
cubital fossa ) by dividing into Ulnar & Radial As.It gives the following branches:
1-Profunda brachi ( Deep brachial )which goes to the Radial( spiral ) groove on the back
of the shaft of the humerus accompanies by the Radial nerve ( after the Axilla).The A divides
into 3 smaller branches while running in the spiral groove these are,ascending branch to
reach surgical neck of humerus & share in the anastomosis there with both anterior &
posterior circumflex humeral A from 3
rd
part of Axillary A,the second one is middle collateral
descends on the back of the Arm to reach the back of Elbow joint & the 3
rd
branch is the
Radial collateral ( considered the continuity of the profunda brachi A.This branch
accompanies the Radial nerve into the front of lateral epicondyle.
2-Superior ulnar collateral A which accompanies the Ulnar nerve into the medial
intermuscular septum.
3-Nutrient branch to the Humerus bone .
4-Muscular branches to supply B.B.C muscles of anterior compartment of Arm.
5-Inferior ulnar collateral which arises just above the cubital fossa& goes to the medial
intermuscular septum to join the Ulnar N.
THE RADIAL NERVE
Is the direct continuity of the posterior cord after giving off its branches.In the Axilla it gives
branches to long head & medial head of Triceps M & posterior cutaneous nerve of Arm. In
the spiral groove it gives 4 branches 2 muscular ( many branches to medial & lateral heads of
triceps + Nerve to Anconeus M) & other 2 branches as sensory these are lower lateral
cutaneous of Arm & posterior cutaneous of F.A.Then the Radial N leaves the spiral groove &
enters the lateral intermuscular septum with the Radial collateral A,then it leaves the septum
to appear in the Cubital fossa between Brachialis & Brachioradialis Ms ( gives branches to
both ),then it divides within the Cubital fossa into Superficial (sensory) & deep branch (
motor).The deep branch will pierce supinator & becomes posterior interosseous N.
THE MEDIAN NERVE
Is formed by a contribution from both lateral & medial cords of the Brachial plexus,then
descends within the anterior compartment of the Armin direct relation with the Brachial A.It
reaches the Cubital fossa just medial to the terminal part of the Brachial A& becomes
sheltered with the A by the Bicepital aponeurosis&then the N leaves the Cubital fossa by
passing between the 2 heads of the Pronater teres M.It supplies 4 Ms of the superficial group

11
of the flexor Ms of the F.A ( Pronater teres, Flexor carpi radialis, Palmaris longus & Flexor
digitorum superficialis) directly& it supplies two & a half Ms of the deep Flexor group
indirectly( i.e via the anterior interosseous branch of the Median N ) to the lateral half of
Flexor digitorum profundus ,Flexor pollicis longus & Pronater quadratus Ms.Finally it leaves
the F.A by passing deep to Flexor Retinaculum to reach the Palm of the Hand.
The Flexor Compartment of Forearm
Is the anteromedial compartment of the F.A ,it includes 8 Ms ( 5 of them are superficial & 3
deep).The superficial are Pronater teres,Flexor carpi radialis,Palmaris longus,Flexor
digitorum superficialis & Flexor carpi Ulnaris.The other 3 deep Ms are Flexor digitorum
profundus, Flexor pollicis longus & Pronater quadratus Ms.
Pronater teres takes origin by 2 heads , humeral & ulnar heads,the humeral head arises from
medial epicondyle& medial supracondylar line ,while the ulnar head from medial side of
Coronoid process of the ulna.The M is inserted into the lateral surface of the middle part of
the shaft of the Radius bone.
Flexor carpi radialis takes origin from the medial epicondyle of humerus& is inserted into th
base of the 2
nd
metacarpal bone.
Palmaris longus takes origin from medial epicondyle & inserts into palmer aponeurosis.
Flexor carpi ulnaris has 2 heads of origin a humeral head from medial epicondyle & ulnar
head from medial side of olecranon process of ulna bone.The M is inserted into the Pisiform
bone ( one of the carpal bones ).
Flexor digitorum superficialis has 2 heads of origin too humeral & radial heads ,humeral from
medial epicondyle,ulnar collateral ligament & medial margin of coronoid process of ulna
bone.while the radial head arises from oblique line on the anterior surface of the radius
bone.The M gives 4 tendons to the medial 4 fingers( each tendon inserts into the sides of the
middle phalange of the corresponding finger).
Flexor digitorum profundus takes origin from the upper 3/4(three fourth)of anterior,medial
&posterior surfaces of the ulna bone and from anterior surface of interosseous membrane.
The M gives 4 tendons to the 4 medial fingers ( inserts into the base of the distal phalanges).
Flexor pollicis longus takes origin from middle 2/4 of anterior surface of Radius bone
&interosseous membrane.The M inserts into the base of distal phalanx of the thumb.
Pronater quadratus takes origin from oblique line on the lower 1/4 of anterior surface of ulna
bone & inserts into the lower 1/4 of anterior surface of the radius bone.
Notes : 1-The first 5 Ms are superficial group,while last 3 are deep group.

12
2- Four of them are innervated directly by median N ,two & half indirectly ( i.e via
the anterior interosseous branch of the median N ).
3-Flexor carpi ulnaris & medial half of Flexor digitorum profundus are supplied by the
ulnar nerve.
THE FLEXOR RETINACULUM
It is the thickened part of the deep fascia of the F.A located anteriorly at the junction
between the F.A & palm of the hand in front of some carpal bones.It is attached to pisiform
& hook of hamate medially,while laterally attached to scaphoid & trapezium ,this fibrous
retinaculum bridges over some carpal bones forming a fibro—osseous tunnel known as the
carpal tunnel through which pass the following structures:
1- Four tendons of Flexor digitorum superficialis.
2- Four tendons of Flexor digitorum profundus.
3- Tendon of Flexor pollicis longus .
4- The Median nerve.Thus the median N is liable for compression in certain
circumstances leading to what is called Carpal Tunnel Syndrome.
The following structures cross superficial to Flexor Retinaculum:
1-Tendon of palmaris longus M.
2-The Ulnar Nerve.
3-The Ulnar Artery.
4-Palmer cutaneous branch of the Median nerve.
5-Palmer cutaneous branch of the Ulnar nerve.
The Ulnar Nerve
Is one of the branches of the medial cord of the Brachial plexus,it doesn’t supply any
structure in the arm,just above the middle part of the Arm it pierces the medial
intermuscular septum of the Arm( accompanied by both superior & inferior Ulnar
collateral As ).It leaves the Arm by passing behind the medial epicondyle of the humerus
to reach the F.A,it passes between the 2 heads of Flexor carpi ulnaris to reach F.A. In the
F.A it descends under cover the Flexor carpi ulnaris M accompanied by the Ulnar A .It
supplies Flexor carpi ulnaris & medial half of Flexor digitorum profundus M,then at the
lower part of the F.A it gives dorsal ulnar cutaneous branch which goes to the back of the
hand to supply sensations .Just before it leaves the F.A it gives palmer cutaneous branch
which passes superficial to the Flexor retinaculum to reach the Palm of the hand.

13
Posterior compartment of Forearm
It includes 7 superficial & 5 deep Ms .The superficial are Brachioradialis,Extensor carpi
radialis longus, Extensor carpi radialis brevis,Extensor digitorum,Extensor digiti minimi
,Extensor carpi ulnaris & Anconeus muscles.The Deep group includes Abductor pollicis
longus,Extensor pollicis brevis, Extensor pollicis longus , Extensor indices & Supinator Ms
The Brachioradialis takes origin from upper two thirds of lateral supracondylar ridge&
lateral intermuscular septum.It is inserted into the lateral side of Radius bone.
Extensor carpi radialis longus takes origin from lower third of lateral suracondylar ridge &
lateral intermuscular septum.It inserts into the base of 2
nd
metacarpal bone.
Extensor carpi radialis brevis arises from lateral epicondyle& radial collateral ligament.It
is inserted into the base of the 3
rd
metacarpal bone.
Extensor digitorum takes origin from lateral epicondyle .It gives 4 tendons to the medial
four fingers on the back& insert via extensor expansion to middle & distal phalanges.
Extensor digiti minimi takes origin from lateral epicondyle too.Its tendon join the tendon
of extensor digitorum for the little finger.
Extensor carpi ulnaris takes origin from lateral epicondyle & posterior border of Ulna
bone.It is inserted into the medial side of the base of 5
th
metacarpal bone.
Anconeus takes origin from lateral epicondyle & inserts into the lateral side of Olecranon
process& upper one fourth of posterior surface of Ulna bone.
Abductor pollicis longus takes origin from posterior surface of Ulna & Radius below the
Anconeus.It is inserted into the base of 1
st
metacarpal bone.
Extensor pollicis brevis takes origin from posterior surface of Radius & from interosseous
membrane.It is inserted to the base of the proximal phalanx of the Thumb.
Extensor pollicis longus takes origin from posterior surface of Ulna & interosseous
membrane .It is inserted to the base of the distal phalanx of the Thumb.
Extensor indices takes origin from posterior surface of Ulna & interosseous membrane.
Its tendon goes with the tendon from extensor digitorum for the index finger & joins its
extensor expansion .
Supinator takes origin from many sites as lateral epicondyle , Radial collateral ligament ,
annular ligament of superior Radio-ulnar joint & from Supinator crest of Ulna bone.It
wraps round the upper third of Radius to get insertion to the posterior surface ,lateral &
anterior surfaces of the upper third of Radius bone.Note the following for innervations:
1-Brachioradialis & Extensor carpi radialis longus from Radial nerve before its division.
2-The Supinator by deep branch of Radial N as it pierces its substance.

14
3-Anconeus by the nerve to Anconeus given off by Radial N as it runs in Spiral groove.
4-All the rest of the Extensor Ms are supplied by the posterior interosseous N which is the
direct continuity of the deep branch of Radial N as it leaves the substance of Supinator M
to run on the posterior surface of the interosseous membrane.
THE SNUFF BOX
Is seen at the base of the Thumbposteriorly,it is bounded laterally ( or anteriorly )by the
tendons of Abductor pollicis longus & that of Extensor pollicis brevis,while medially ( or
posteriorly) by the tendon of Extensor pollicis longus.Its roof is formed by the skin & fascia
being crossed superficially by the terminal branches of superficial branch of Radial N &
the beginning of Cephalic vein,where as its floor is formed by Scaphoid bone + Styloid
process of the Radius bonelying on them the Radial artery ( feel pulsation here).
EXTENSOR RETINACULUM
Exactly like the Flexor Retinaculum on the back of the Wtist region at the junction
between back of F.A & Dorsal aspect of the Hand.It is attached to the lower end of anterior
border of Radius ( laterally ) & to the Pisiform + Triquetral boneswith the Styloid process
of Ulna ( medially ).Deep to it the extensor tendons pass via 6 compartments.
THE SHOULDER JOINT
It is a synovial joint of ball & socket variety between the shallow glenoid cavity of Scapula
& hemispheroidal head of Humerus ( both articular surfaces are covered by hyaline
cartilage.The concavity of Glenoid fossa is deepened by a fibro-cartilagenous rim known
as Glenoid labrum.The thin & lax capsule allows freedom of movements at the joint ,it is
re-inforced by the tendons of the Rotator cuff Ms.The capsule is lined by from inside by
synovial membrane which forms a cavity ( synovial cavity).The ligaments of the joint are:
1- Glenohumeral ligaments which are 3 in number, superior ,middle & inferior (known as
intrinsic ligaments).
2- Coraco-humeral ligament( Extrinsic ligament ).It is a thick band from the root of
coracoid process to the upper part of the front of greater tuberosity.
3- Transverse humeral ligament ( Extrinsic ) ,it stretches between the lips of Bicepital
grooveof the humerus converting it into a canal for the passage of the tendon of long
head of biceps.
4- Coraco-acromial ligament( accessory),its apex attached to the a cromion & its base
attaches to the lateral border of the Coracoid process.
5- There are 4 bursae related to the joint ,these are the subscapular,infraspinatous,

15
Subacromial & subcoracoid bursae.
The joint receives articular ( sensory ) nerve supply from the Axillary & suprascapular
nerves.It receives blood supply from anterior & posterior circumflex humeral ,and also
from circumflex scaular & suprascapular arteries.The movements are as follows:
1- Flexion is performed by anterior fibers of Deltoid,clavicular head of pectoralis
major,Biceps & Coracobrachialis muscles.
2- Extension by posterior fibers of Deltoid& teres major muscles.
3- Abduction by supraspinatous up to 18 degree,then by the lateral fibers of Deltoid
from 18—90 degree.Beyond 80 degree occurs at the shoulder girdle due to rotation
of scapula by Trapezius & Serratus anterior muscles.
4- Adduction by Pectoralis major & Latissimus dorsi muscles.
5- Medial rotation by Pectoralis major,anterior fibers of Deltoid& Subscapularis .
6- Lateral rotation by posterior fibers of Deltoid,infraspinatous & Teres minor Ms.
7- Circumduction is a combination of all the above movements.
Applied Anatomy:
1- Due to instability of the joint & laxity of the capsule,it is frequently lible to inferior
dislocation( the capsule here is least protected by muscles.This dislocation may
cause injury or pressure on the Axillary nerve.
2- Osteoarthritis & Rheumatoid arthritis which may needs artificial joint replacement,
3- Supraspinatous tendinitis is usually secondary to subacromial bursitis,thus results
in the inability to initiate abduction.
THE ELBOW JOINT
Is a compound synovial joint of hing variety,includes 2 articulations a Humeroulnar
& Humeroradial.
The Trochlea of the humerus articulates with the Trochlear notch of Ulna.The
Capitulum of Humerus articulates with head of Radius,they are covered by hyaline
cartilage.The capsule is attached (above ) in front to the medial epicondyle&upper
margins of Coronoid & Radial fossa,but from behind along the trochlear
margin,margin of Olecranon fossa & over the Capitulum.Below along the margins
of the Coronoid & Olecranon processes and to the Annular ligament around the
head of the Radius.The inner surface of the Capsule & the 3 fossae are lined by
synovial membrane.
Ligaments are the followings:
1-Ulnar collateral(Medial) ligament.It is triangular band with anterior,posterior &
inferior thick bands and middle thin part.
2-Radial collateral (lateral) ligament .It extends from lateral epicondyle of the
Humerus to the Annular collateral ligament.
3-Anterior & posterior ligaments which strengthen the capsule in front &behind.

16
The main relations are as follows:
1-Anteriorly by Brachialis,tendon of Biceps,Median N & Brachial artery.
2-Posteriorly by Anconeus & insertion of Triceps.
3-Medially by common Flexor origin & the Ulnar nerve.
4-Laterally by common Extensor origin & Supinator M.
The joint are supplied by articular (sensory) branches from Radial &
Musculocutaneous nerves.The blood supply by branches from the anastomosis
around the Elbow joint.The main movements at the joint are the followings:
1-Flexion movement is performed by Brachialis & Biceps .
2-Extension is performed by Triceps & Anconeus.
Applied Anatomy includes the following cases:
1-Dislocation which is usually a posterior one&is often associated with fracture of
the Coronoid process.Here the Anatomical Triangular relation ship between the
Olecranon & the 2 Epicondyles is lost.
2- Subluxation of the head of Radius(pulled elbow) occurs in children when the F.A
is suddenly pulled in Pronation movement.The head of the Radius slips away from
the Annular ligament.The Elbow is kept fixed in slight Flexion & Pronation,while
Supination is limited and is painfull.
3-Tennis Elbow.Any abrupt Pronation may lead to pain & tenderness over the
lateral epicondyle.This is possibly due to the following factors
A-The sprain of Radial collateral ligament.
B-Tearing of the fibers of Extensor carpi Radialis Brevis.
C-Inflamation of the Bursa related to M tendon.
4-Student's Elbow: Repeated excessive friction may cause inflammation of
subcutaneous Olecranon Bursa.Gout may cause subcutaneous Bursitis.
5-Effusion of the joint,leads to distension which occurs posteriorly ,because here
the Capsule is weak&the covering deep fascia is thin.Aspiration is done on any side
of the Olecranon to remove the fluids.
All lectures are found in:
QR code of PowerPoint
link of this lecture as PowerPoint :
https://www.muhadharaty.com/files/lectures/file4492.pptx
please join us on this group :
First Stage of Medicine
https://www.facebook.com/groups/1060611617304887
Edited by Hasan Abdulmawjoud