
بسم الله الرحمن الرحيم
1
2
SYMPTOMS
PainStiffness
Deformity
limping

3
How to Start
• IPEEP
• INTRODUCE.
• PERMISSION.
• EXPLANTION.
• EXPOSURE.
• POSITION.
4
The Apley System
All joint examinations follow this system:Look
Feel
Move : Active then Passive
Special Tests
Radiograpgy.
5
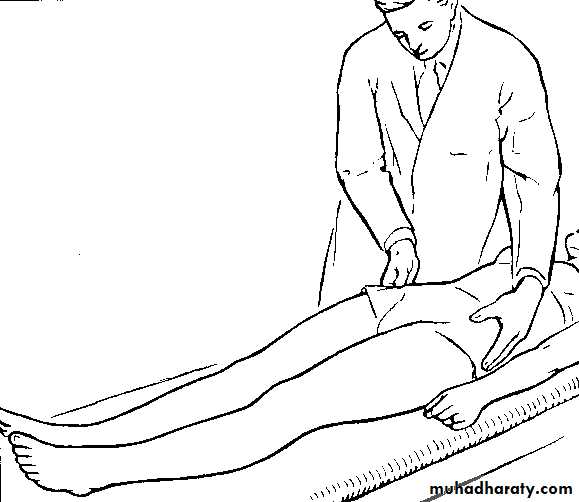
Steps in clinical examination
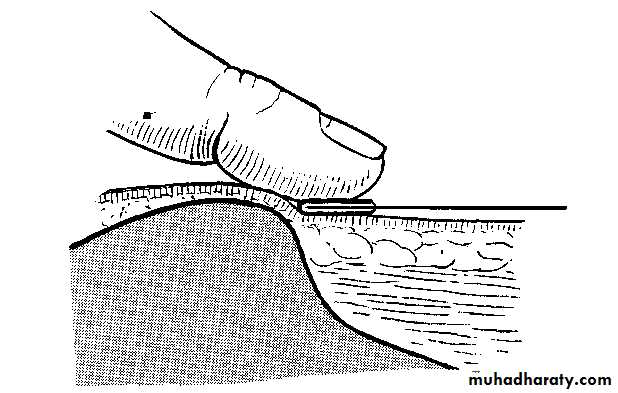
Setting the pelvis squareThis is an important preliminary step.
Determine from the position of
the anterior superior iliac spines whether Or not the pelvis is lying
Square.
adduction or abduction at one or other hip If this is impossible it means that there is in correctible
in that event the fact that
the pelvis is tilted should be noted and borne in mind during thesubsequent steps of the examination.
6
7
8
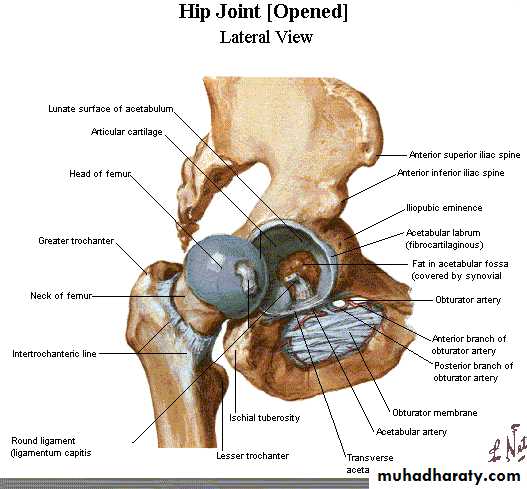
1. LOCAL EXAMINATION OF THE HIP REGION
9
(Patient recumbent)
10Inspectionlook
Bone contours and alignmentSoft-tissue contours
Colour and texture of skin
Scars or sin uses
11
Front and back of pelvis/hips and legs:
any ischaemic or trophic changesSwelling (e.g. lipoma)
Scars (previous surgery)
Sinuses (infection/neuropathic ulcers)
12
Wasting
(old polio, Carcot-Marie-Tooth) orhypertrophy
(e.g. calf pseudo-hypertrophy in muscular dystrophy)
Deformity
(leg length inequality, pes cavus, scoliosis)13
Palpation feel
Skin temperatureBone contours
Soft-tissue contour (Assess any swellings
Assess pelvic tilt by palpating iliac crests
Local tenderness
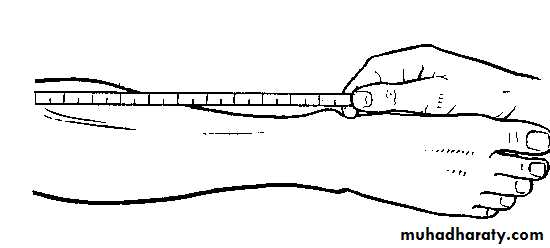
14Measurement of limb length
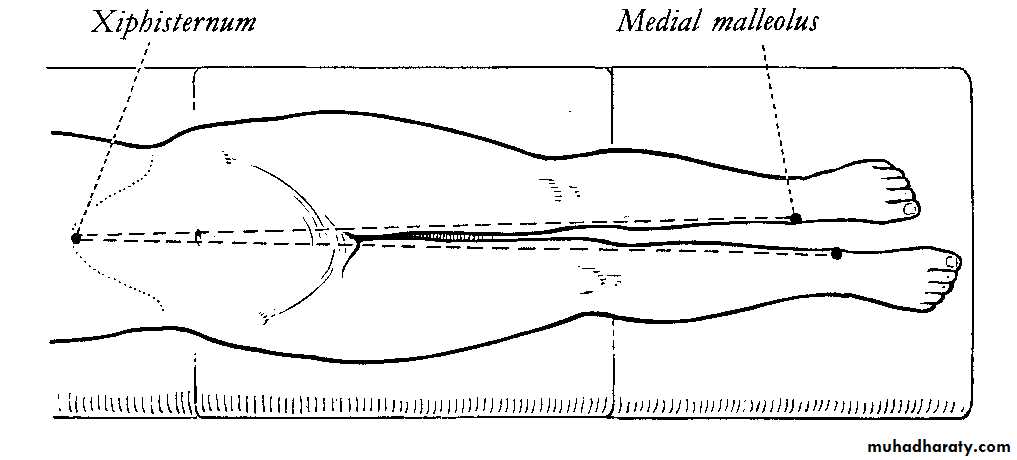
15Real or true length
Measure from anterior superior iliac spine to medial malleolus.(Angle between pelvis and limbs to be equal on each side)
If discrepancy found, determine site of shortening
16
Ideally it would be desirable to
measure from the nor111al axis of hip movement-that is, the centre of the femoral head-but since there is no surface landmark at that point it is impracticable to do so.The measurement is therefore taken from
the nearest convenient landmark namely, the anterior superior spine of the ilium.
Distally, measurement is usually made to the medial malleolus.
17
18

19
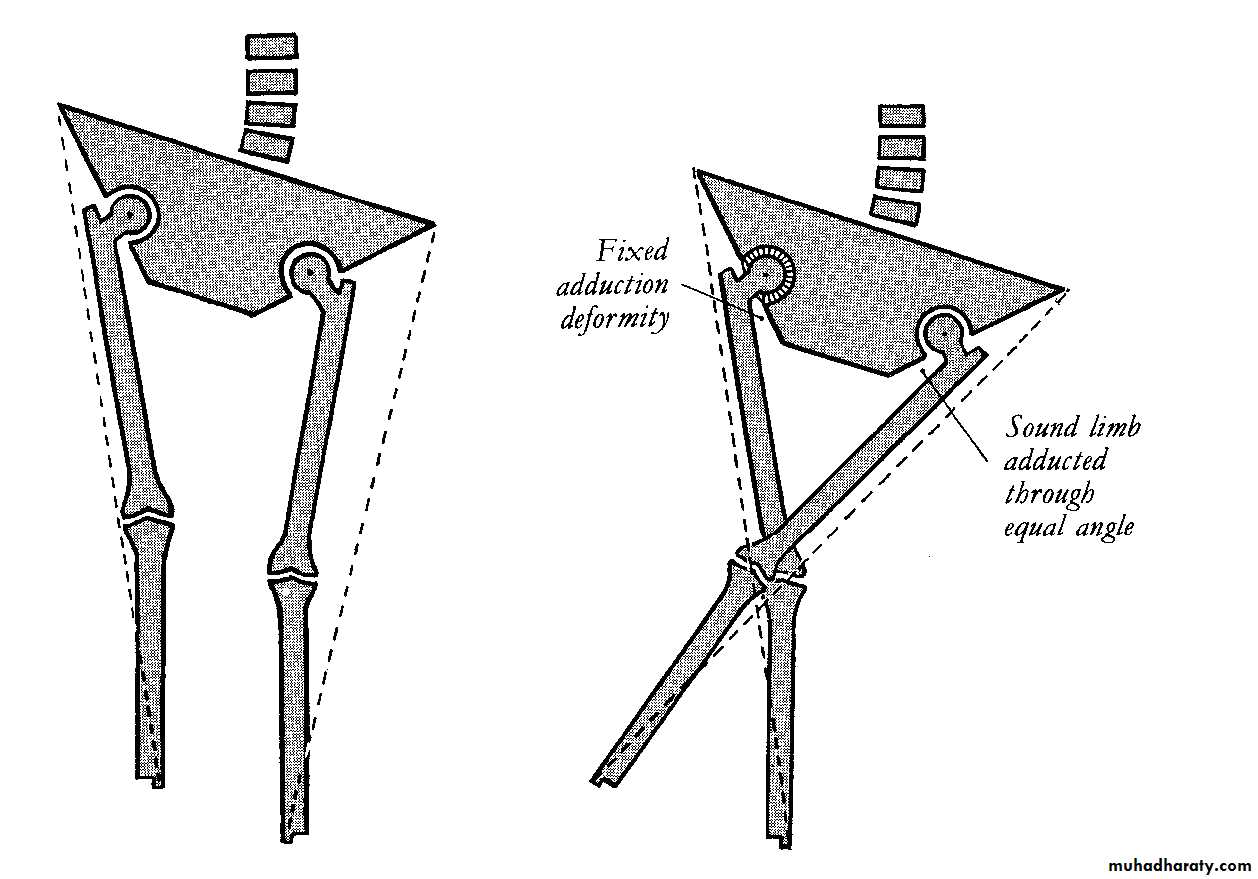
to obtain an accurate comparison of their true length
measurement the two limbs must be placed in comparable positions relative to thepelvis.
Thus if one limb is adducted and cannot be brought out to the
neutral position the other limb must be adducted through a corresponding angle by crossing it over the first limb before the measurements are Taken.
20
Similarly, if one hip is in fixed abduction the other
must be abducted through the same angle before the measurements of true length are made.21
If there is a true leg length discrepancy
, determine which bone/segment of the lower limb is short.It may be below or above the knee (See Galeazzi test below).
.
22
Ask the patient to flex hips to about 45 o and knees to about 90 o . Make sure the heels are together on the couch, with medial malleoli touching.
Look at the knees from the side to see if they are at the same level.
If one is proximal to the other, there is femoral shortening;
if one is distal to the other there is tibial shortening.
23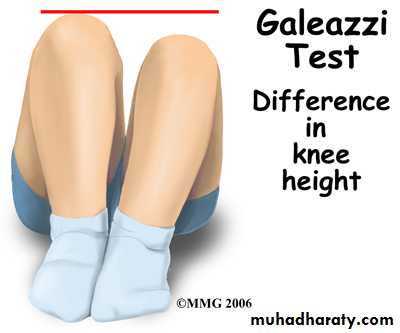
24

25
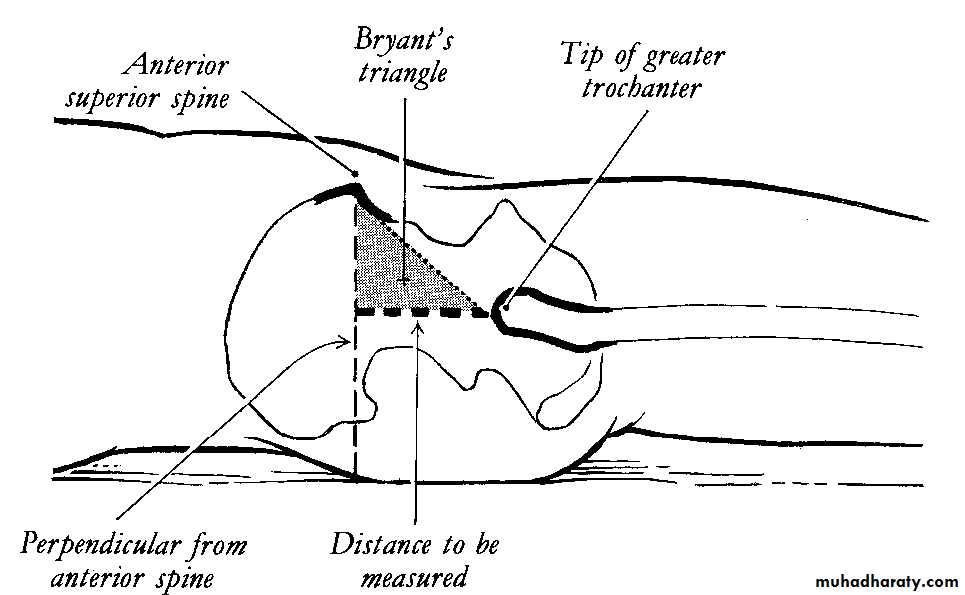
(a) Above trochanter
(Bryant's triangle;)26
With the patient lying supine a
perpendicular is dropped from the anterior superior spine of the iliumtowards the couch.
A second line is projected upwards from the tip of the greater trochanter to 'meet the first line at a right angle.
27
Bryant's triangle
28
If above the knee, it may be above or below the greater trochanter.
Drop a perpendicular from the side of the ASIS and measure distance from greater trochanter to this line.If above the trochanter,
it may be the femoral neck (varus/valgus neck)or head (DDH):
Don't forget to ask yourself "Is the hip in joint?" as a dislocated hip will cause a positive
29
(b) Below trochanter
measure each bone30
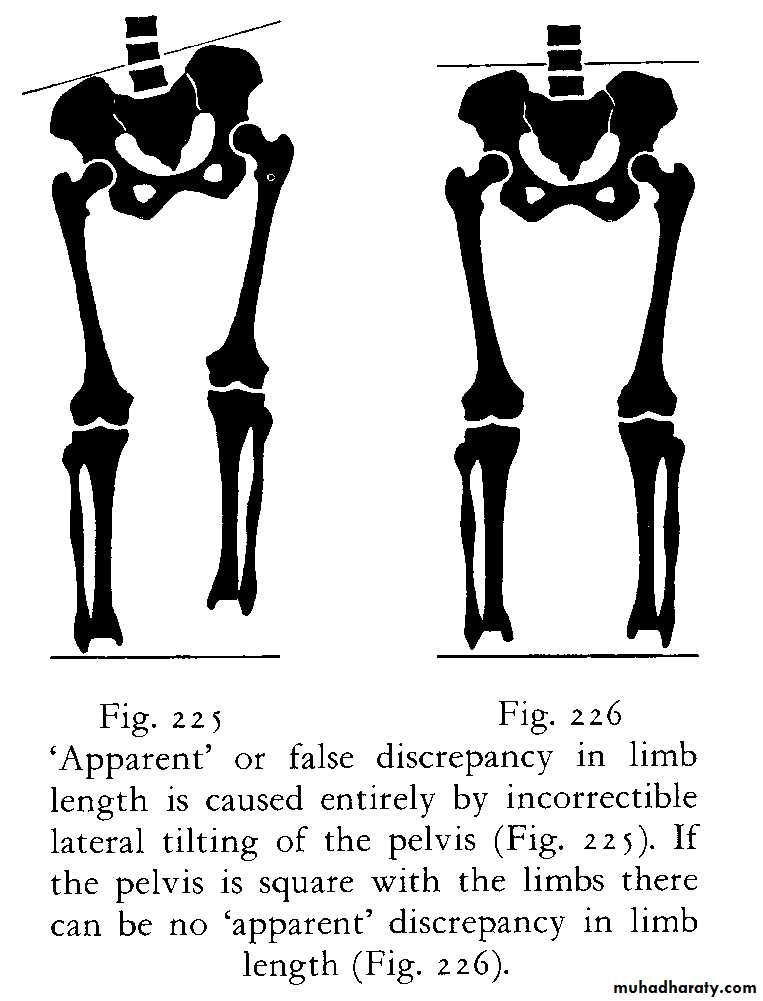
'Apparent' or false discrepancy
31'Apparent' or false discrepancy
IT IS EQUAL TO
PELVIC TILIT +REAL LIMB LENGHT
Measure from xiphisternum to medial malleolus.
(Limbs to be parallel and in line with trunk)32
33
34
35
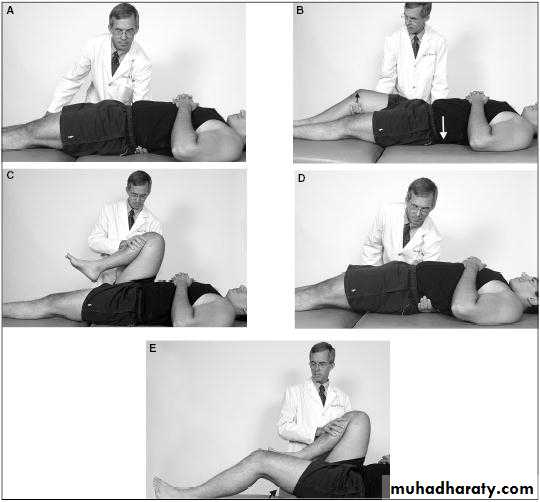
Examination for fixed deformity
Including Thomas's manoeuvre for detectionand measurement of fixed flexion deformity
36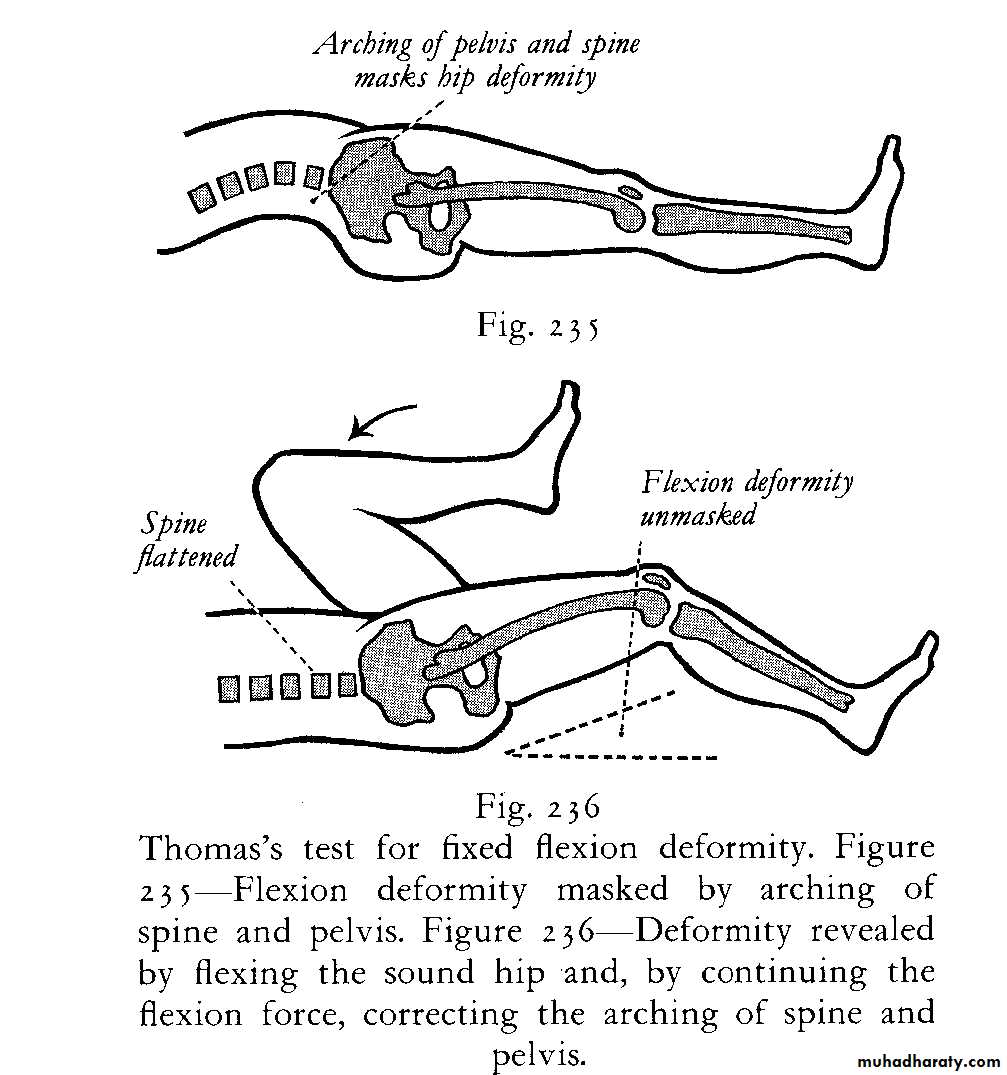
37
38
39

40
Technique of the maneuver
: One hand is placed behind the lumbar spine (between it andthe couch) to assess the degree of lumbar lordosis.
If there is no lordosis
when the affected limb lies flat on the couch there can be no fixed flexion deformity and there is no need to proceed with the test.
If there
is excessive lordosis, as indicated by arching of the back, it is corrected in the following way:
41
The sound hip is flexed to the limit of its range.
The limb is then pushed further into flexion, thereby rotating the pelvis on a horizontal transverse axis until the arching of the spine isobliterated.
During this manaouvre the disordered limb, if in fixed
flexion, is automatically lifted from the couch as the lumbar lordosis is reduced .
The angle through which the thigh is raised from
the couch is the angle of fixed flexion deformity.
42
Movements
43Movements
(active and passive)Flexion
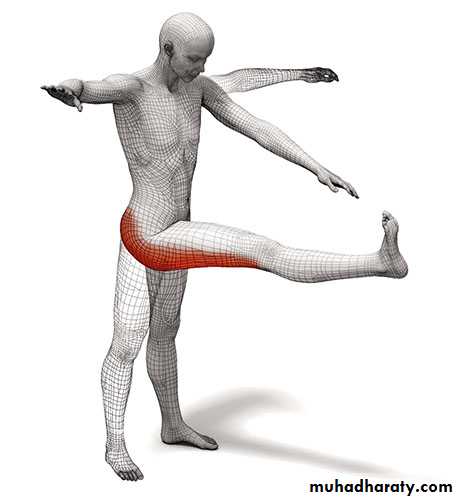
Abduction; abduction in flexion
Adduction
Medial rotation
Lateral rotation
44
flexion
45
flexion
46
EXTENSION
47
ABDUCTION
48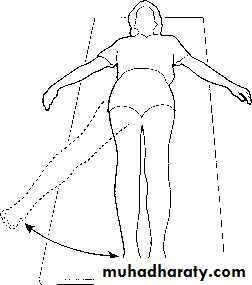
ABDUCTION-ADDUCTION
49
ABDUCTION-ADDUCTION
50
INTERNAL ROTATION
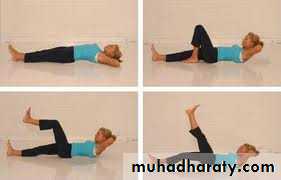
51Power
(tested against resistance of examiner)Estimate strength of each muscle group
52

POWER FLEXOR
ILIOPSOAS53

POWER
EXTENSOR OF THE HIP54
Examination for abnormalmobility
Test for longitudinal (telescopic) movementClick test (in new-born)
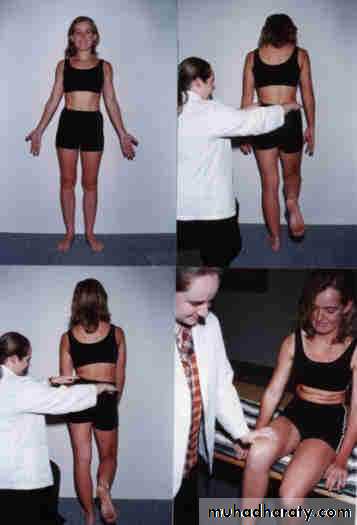
55(Patient standing)
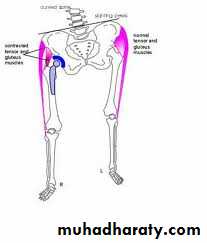
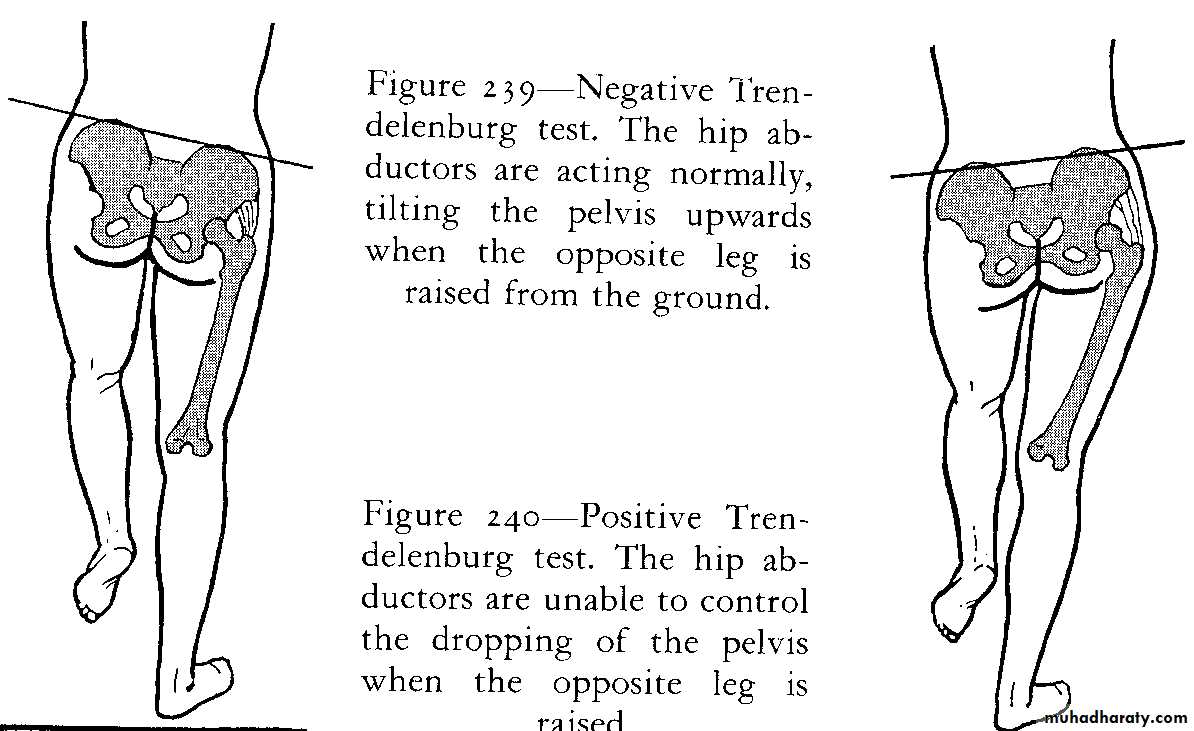
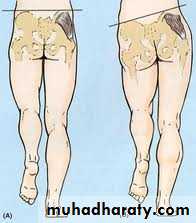
Examination for postural stability
(Trendelenburg's test)
56
57
58

59
60
Gait
61EXAMINATION OF POTENTIAL EXTRINSIC SOURCES OF HIP SYMPTOMS
This is important if a satisfactory explanation for the symptoms is not found onlocal examination. The investigation should include:
I) the spine and sacro-iliac joints
2) the abdomen and pelvis; and
3) the major blood-vessels.
62
3. GENERAL EXAMINATION
General survey of other parts of the body.The local symptoms may be only one
manifestation of a widespread disease.
63
CLASSIFICATION OF DISORDERS IN THE HIP REGIONARTICULAR DISORDERS OF THE HIP
64
CONGENITAL DEFORMITIES
(DEVELOPMENTAL HIP DYSPLASIA)65
ARTHRITIS
Transient synovitis of childrenPyogenic arthritis
Rheumatoid arthritis
Tuberculous arthritis
Osteoarthritis
66
OSTEOCHONDRITIS
Perthes' disease67
MECHANICAL DISORDERS
Slipped upper femoral epiphysis
68
EXTRA-ARTICULAR DISORDERS IN THE REGION OF THE HIP
69DEFORMITIES
Coxa vara70
INFECTIONS
Tuberculosis of the trochanteric bursa71
MECHANICAL DISORDERS
Snapping hip72
Age at Timeof Diagnosis Disease
(Years)0 to 2 Congenital dislocation
2 to 5 Tuberculous arthritis; transient synovitis
5 to 10 Perthes' disease; transient synovitis
73
10 to 20 Slipped upper femoral epiphysis
20 to 50 Osteoarthritis (secondary to previous Injuryor disease)
50 to 100 Osteoarthritis (primary)
74