1
Fifth stage
Radiology
عملي
د.هديل
2/12/2015
Regarding GIT radiology
Must describe the part of the tract we examine Ba - swallow , meal , follow through &
enema
If the film is chest XR with upper abdomen must exclude 2 things
1.Pnemoperitonium if it is crescent shape
2. Sub phrinic abscess if there is straight air fluid level
In KUB film of abdomen
Once see dilated bowel loops 2 things must verified
The film is erect or supine
a.The dilated bowel loops if being central small numerous in no. cross the midline with
valvula convents (it is small bowel obstruction ).
b.If the dilated bowel loops is peripheral large few in no. (it is large bowel obstruction ) .
Once see dilated esophagus in Ba swallow 3 things have to exclude
1.If the stricture is long length it is being benign stricture of the esophagus
2.If it is short length & below diaphragm it is achalasia
3.If the length is variable have missing part with meniscus sign it is being malignant
In ba- meal examination concentrate on lesser & greater curvature
a. Any projection from the lesser curvature in profile view it is ulcer unless proven other
wise .
b. Any irregularity in the greater curvature or distal pyloric antrum of stomach , filling
defect , irregular narrowing +/- meniscus sign or what is called apple core sign it is Ca
stomach
Examination of duodenum is also called ba-meal examination
Must exclude 2 things
2
a.Ulcer
b. Duodenal diverticulm ( which is well defined oval or rounded shape smooth wall out
pouching from the second part of duodenum )
In ba-enema examination must look carefully to any area of narrowing & constriction &
any constriction looks like apple core sign
( meniscus sign ) it is infiltrative ca colon
Regarding the KUB + IVU films
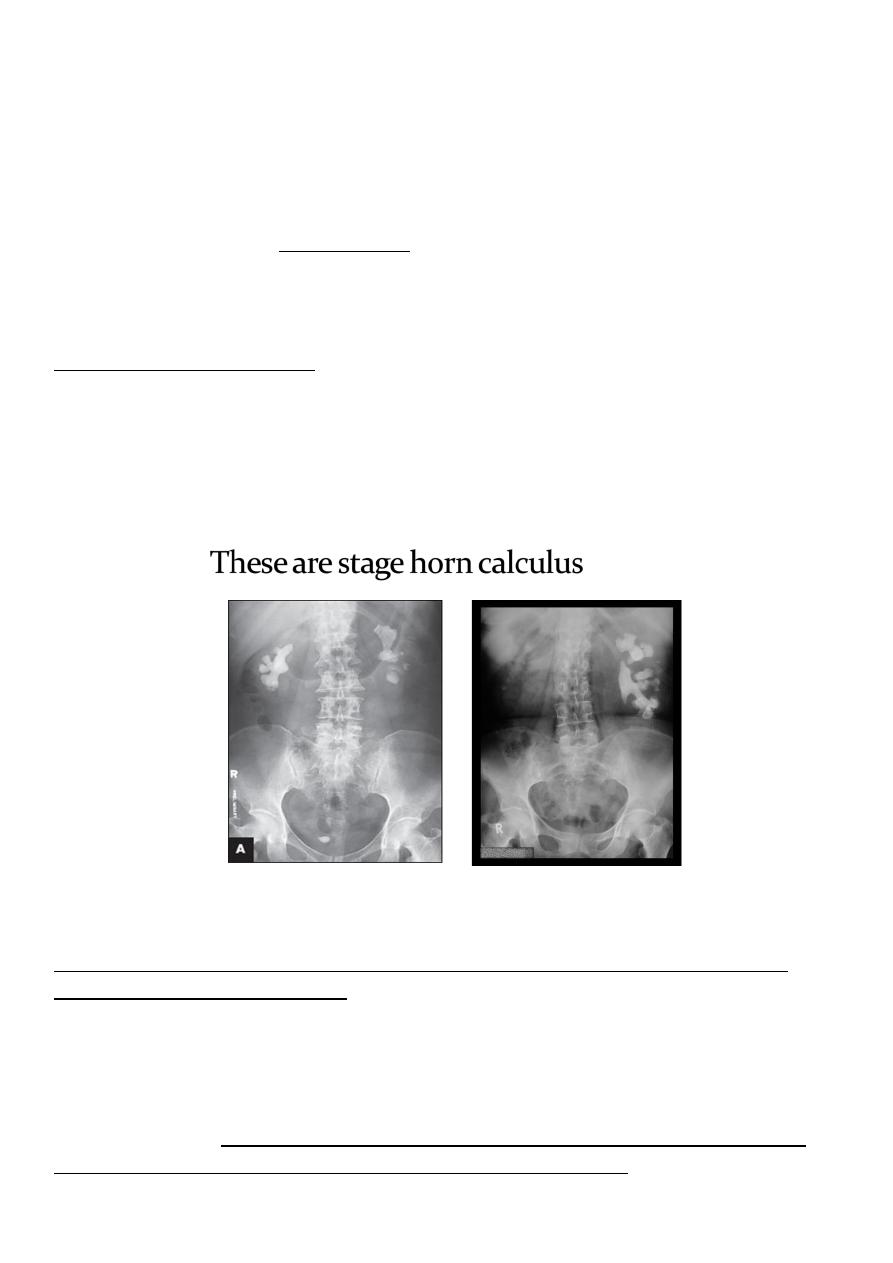
a. Must looks carefully to KUB film for any radio opaque shadow ( so it is stone )
important pitfall in stage horn calculous the calcified large stone take the shape renal
pelvis could be unilateral or bilateral so not to be confused with hydronephrosis by looking
to the pelvis in which cystogram is not seen
b. In IVU films
Once we see hydro nephrosis & hydro ureter looks to the distal ureteric obstruction &
exclude the followings obstructed causes
1.Stone ( unilateral or bilateral )
2.VUR ( uniulatral or bilateral )
3.Uretrocele ( there is unilateral or bilateral HN +HN although the distal ureter is rounded
cobra head shape ) so it is being big trick !!!!!!!!!!!!! must not to fall in it !!!!!!!! although
the distal ureteric end rounded but the it is orifice is being narrow )
3
In IVU film interpretation must look to for important thing
a. Renal pelvis & ureter for any duplication
b. The inferior pole of the renal pelvis directed outward parallel always to psoas muscle any
medial inward direction with fusion of the lower pole calyx it is being horse shoe kidney
In US examination of the kidney 3 important integral findings being almost the hallmark of
the kidney sono graphic examination request
*Stone ( echogenic white ) with reflection .
*Renal cyst ( echolucent black rounded ) with enhancement .
*Centraly dilated renal pelvis with dilated major & minor calyx ( hydro nephrosis ) .
In CT scan films
We can solve the film easily !!!!!! By comparison
Always compare the 2 sided aspect
1.The stone always in CT scan is white hyper dense even if it is of low ca .
2.The tumor in CT scan is cause heterogeneous mass destructed the whole kidney & renal
pelvis & the lesion could enhance heterogeneously or cause over all necrotic non enhancing
mass lesion .
3.The absent kidney easily excluded in CT scan although the CT scan being of high radiation
dose but indicated in certain cases .