Fifth stage
GynecologyLec-4
د.اسماء
26/11/2015
Polycystic ovary syndromeThe student at the end of this lecture should be able to:
Enumerate the diagnostic criteria for PCOS.Describe it’s clinical presentation.
Describe the underlying hormonal changes .
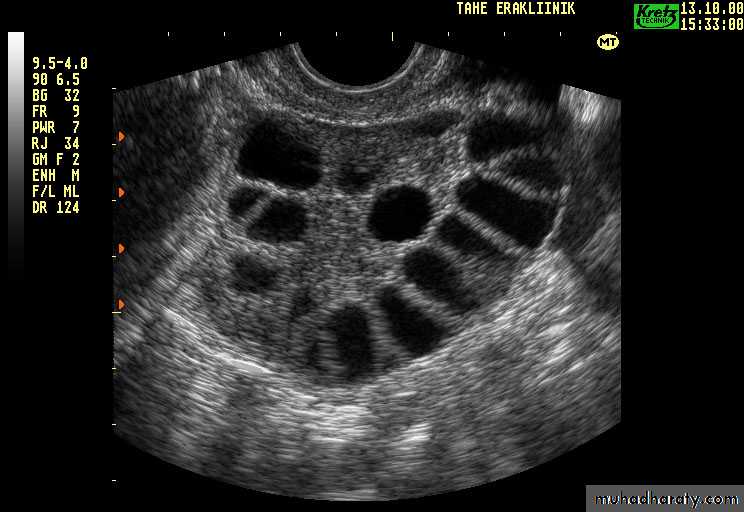
Describe the ultrasounic features diagnosing PCOS.
Predict the life long risk for PCOS.
Differentiate PCO from PCOS.
Describe the available options for treating the presenting problems.
Poly cystic ovary syndromeIs a heterogeneous collection of symptoms and signs .It's diagnosed by the presensce of two out of the following three criteria: oligo and /or anovulation. Hyperandrogenism clinically or biochemically. Polycystic ovaries by transvaginal ultrasound.
Incidence
In general,1-4% of women in the reproductive age
suffer from PCO.
It’s the commonest endocrine disorder in women,
prevalence(15-20%).
Inheritance:
It runs in families and affect approximately 50% of 1st degree relatives suggest dominant inheritance.Clinical presentations of PCOS
-no symptoms
-menstrual irregularities and dysfunction ranging from
oligomenorrhoea to amenorrhoea , about 30% have normal cycle,50%have oligomenorrhoea and 20% have amenorrhoea. Even in patient with regular cycle with hyperandrogenism the rate of anovulation is 21%.
-hyperandrogenism : hirsutism ,acne ,alopecia ,but not virilism.
-obesity (10-65%):central type with higher waist to hip ratio .
-
-recurrent miscarrige:its relation to PCOS has been recently questioned.
-insulin resistance and hyperinsulinemia .
-impaired glucose tolerance test(1/3 of obese PCOS patient have impaired glucose tolerance test and 7.5% to 10% have type 2 diabetes.
-abnormal lipoprotein are common in PCOS(elevated total cholesterol, triglyceride, LDL, and low level of HDL.
Pathophysiology and labrotory finding:
Hyperandrogenism and anovulation in PCOS is caused by endocrine abnormality mainly in the ovary with the total testosterone level is usually not more than twice the upper normal range(20-80 ng/dl).
High intraovarian androgen concentration inhibit follicular maturation.
E1 level is increased as a result of peripheral aromatization
of hyperandrogenisim .
There is abnormal estrogen feed back at the hypothalamic
pituitary gland result in elevated LH and LH:FSH ratio
and exhibit elevated prolactin level in 25% of patients.
PCOS patient insulin resistance and compensatory
hyperinsulinaemia as a result of PCOS and obesity. Insulin
is a potent stimulus for insuline secretion of androgen by
the ovary by the presence of different type of receptor
doesn’t exhibit insulin resistance also it suppress the
synthesis of SHBG by the liver thus elevate the free
androgen index. Patient are at increased risk of glucose
intolerance or frank diabetes.
Long term risk for patients with PCOS
Persistently elevated level of estrogen uninterrupted byprogesterone increase the risk of endometrial cancer,
breast cancer and ovarian cancer.
Obesity and metabolic abnormality and increase of plasminogen activator inhibitor cause reduced fibrinolysis all are risk factors for the development of ischemic heart disease (7 fold increase in MI) ,hypertention and dyslipidaemia .
Insulin resistance and hyperinsulinaemia make the
patient at risk of diabetes and gestational diabetes later on
in life.
During subsequent pregnancy there is increased risk of abortion ,gestational diabetes ,and pre-eclampsia.There is also increased morbidity in obese PCOS who fails to reduce their weight.
Diagnostic investigation:
Ultrasound: increased stromal thickness and increasedovarian volume (>10 cm3)(specific for PCOS),and the
presence of 12 or more follicles measured 2-9 mm in
diameter.
Serum endocrinology:
Increase serum LH
Increase serum LH : FSH ratio
Increase serum androgen (testosterone and androstenedione)
Decrease SHBG
Increase estradiol and estrone (not measured routinely
as Very wide rang of values).
Increase serum prolactin.
Increase serum insulin level.
Impaired glucose tolerance .
Management of PCOS:
The clinical management of PCOS should be focused on the individual problemsObesity : obesity worsen the symptoms and the endocrine profile so obese women (BMI >30 kg/m2) should reduce their weight and modify their life style by diet modification , increase exercise , stop smoking.
Menstrual irregularities:
low dose combined oral contraceptive preparation.
Progesterone as medroxy progesterone
acetate (provera) Or dydrogesterone
(duphastone) for 12 days every 1-3 months to
induce withdrawal bleeding.
Hyperandrogenism and hirsutism :
A standirized scoring system as the modified Ferriman
and Gallway score may be used to evaluate the degree
of hirsutism before and during treatment .
Physical treatment : electrolysis, waxing and bleaching,
Laser and photothermolysis may be helpful while
waiting the effect of medical treatment.
Medical treatment : stop further progression and decrease
the rate of hair growth. Adequate contraception is
important during treatment as antiandrogen disturb the
development of male genital tract:
First line is diane (ethinylestradiol 30 Mg with cyproterone acetate 2mg.CPA may cause liver damage
So require regular checking and once response is achieved we should be switched to COCP because diane can increase the risk of thromboembolism.
Spironolactone is a weak diuretic with antiandrogenic
properities can be used at a daily dose of 25-100 mg .Other antiandrogen as Ketoconazole ,Finasteride and
Flutamide (not used because their side effect and they
are no more effective thane CPA
Treatment of infertility in PCOS
1. life style modification including diet reduction and exercise. A loss of 5-10% of body weight in obese PCOS patients improve the prospect of both spontaneous and drug induced ovulation2.Medical Induction of ovulation in PCOS patient by a. antioestrogen : - clomiphene citrate . - Tamoxifene.
Clomiphene citrate : is an orally active synthetic non
steroidal compound with oestrogenic and nonoestrogenic properties.
It displace the oestrogen from it’s receptor at the hypo-
thalamic pituitary axis reduce it’s negative feed back
and encourage GnRH secretion.
It’s administered at 50 mg daily dose on day 2-6 of
a spontaneous and induced menstrual cycle(increased
by 50 mg /day till ovulation occur for a max. Dose.
A course of 6-12 cycles can be used in women who
respond to treatment with monitoring by ultrasound
for follicular response.
Ovulation is expected in 80% and pregnancy in 40% .
Adverse reaction to such treatment:
-Antioestrogenic side effect including thickening of the
cervical mucos and hot flushes in 10% of women.
-abdominal pain ,nausea , vomiting .
-headache and visual disturbance.
-breast tenderness.
-reversible hair loss.
-ovarian enlargement, and ovarian hyperstimulation syndrome is rare in <1%.
-Multiple pregnancy in 10%.
-Ovarian cancer described in women receive treatment for more than 12 cycles.
Tamoxifen:has structure similar to clomiphene .the recommended dose is 20- 40 mg per day from day 3 for 5 days it have the same pregnancy rate as clomiphene with less potent antioestrogenic action on the cervical mucos.
b. Medical induction by gonadotrophin :
Gonadotrophin are used when the patient do not respondto clomifene or fails to conceive after 6-12 ovulatory cycles.
Preperation in common use include recombinant FSH or
purified urinary human menopausal gonadotrophin (FSH
and LH). Gonadotrophin treatment result in cumulative
Pregnancy rates of 40-50% and 1-2% rate of OHSS.
c. GnRH analogues in ovulation induction : it’s usedin conjunction with gonadotrophin to achieve pituitary down regulation to facilitate cycle control
d. Metformin : this is an oral biguanide inhibits the
production of hepatic glucose ,enhance the sensitivity ofperipheral tissue to insulin thus decrease the secretion
of insulin and treat hyperinsulinaemia.
Metformin is shown to decrease hyperandrogenism and
abnormalities of gonadotrophin secretion and can
restore menstrual cyclicity and fertility.
The usual dose is 850 mg bid or 500 mg t.d.s. taken
Before meal .
Side effect of metformin: nausea ,vomiting , flatulance and diarrhoea . (these can be reduced by taking the drug before the meal and by gradually increasing the dose start with 850 mg nocturnal then 850 mg bid for the next week.
Metformin is not usually cause Lactic acidosis in non
diabetic patient with PCOS with normal liver and renal
Function.
Regular checking of renal and liver function, metformin
should discontinued for 3 days after iodine containing
compound and should be discontinued during
pregnancy(although there is no evidence of
Teratogenesis).
3. Surgical method of ovulation induction
Laparoscopic ovarian diathermy LOD: by diathermy orLaser, it appear to be more successful in a slim patient
with high LH level. A unipolar coagulating current is
used to deliver four punctures to a depth of 4 mm in
each ovary .The principle advantage of ovarian drilling is
monofollicular ovulation resulting in fewer multiple
pregnancy rate with the cumulative pregnancy rate
similar to those obtained with 3-6 cycle of gonadotrophin.
LOD has replaces the wedge resection of the ovaries as it
result into extensive peri-ovarian and peritubal adhesion.