LEC. Dr.Khaled
MEDICINELymphoma
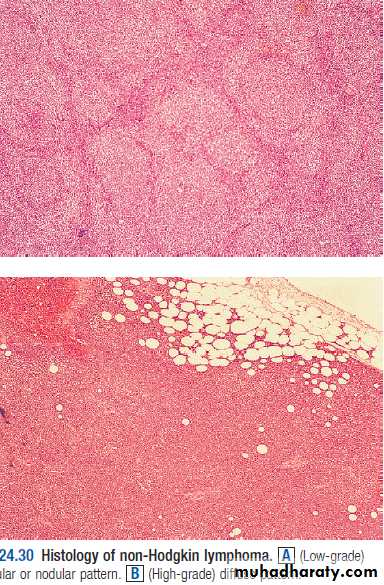
Most present as tumor Involving lymph nodes or otherlymphoid organs such as the spleen. But extra nodalpresentation may seen.1. Hodgkin’s Lymphoma.2.Non - Hodkin’s Lymphoma; Non-Hodgkin lymphomas areclassified as low- or high-grade tumours on the basis of theirproliferation rate.High-grade tumours divide rapidly, are typically present for amatter of weeks before diagnosis, and may be life-threatening.• Low-grade tumours divide slowly, may be present for manymonths before diagnosis, and typically behave in an indolentfashion.
Hodgkin lymphoma
Histological WHO classification
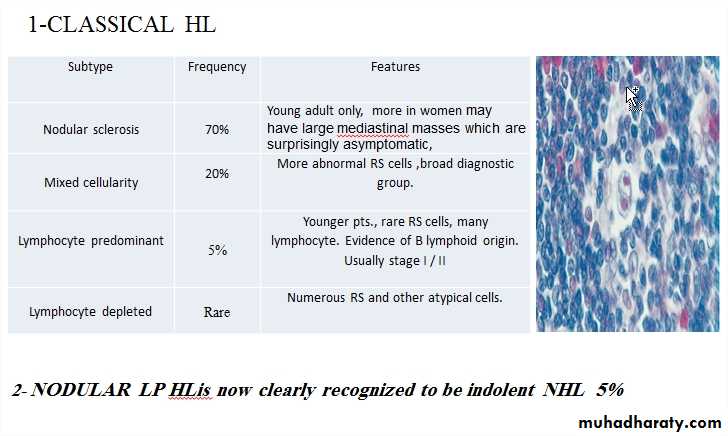
Clinical featuresThere is painless, rubbery lymphadenopathy, usually in the neckor supraclavicular fossae; the lymph nodes may flucuate insize(wax an wan).
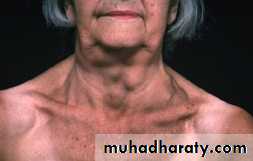
Hepatosplenomegaly may be present but does not alwaysindicate disease in those organs.Spread is contiguous from one node to the next and extranodaldisease, such as bone, brain or skin involvement, is rare.
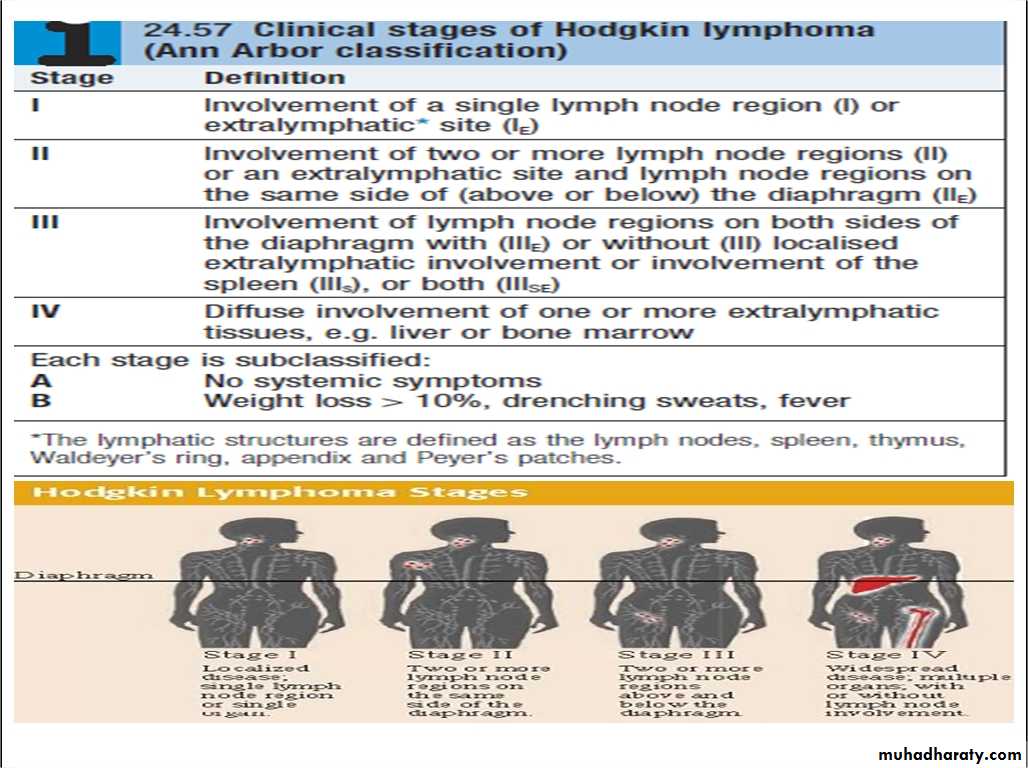
InvestigationsFBC may be normal. If a normochromic, normocyticanaemia or lymphopenia is present, this is a poorprognostic factor. An eosinophilia or a neutrophiliamay be present.• ESR may be raised.• Renal function tests are required to ensure function is normal prior to treatment.• Liver function may be abnormal in the absence of disease or may reflect hepaticinfiltration. An obstructive pattern may be caused by nodes at the porta hepatis.LDH measurements showing raised levels are an adverse prognostic factor.• Chest X-ray may show a mediastinal mass.• CT scan of chest, abdomen and pelvis permits staging. Bulky disease (> 10 cm in asingle nodemass) is an adverse prognostic feature.• Lymph node biopsy may be undertaken surgically or by percutaneous needle biopsyunder radiological guidance
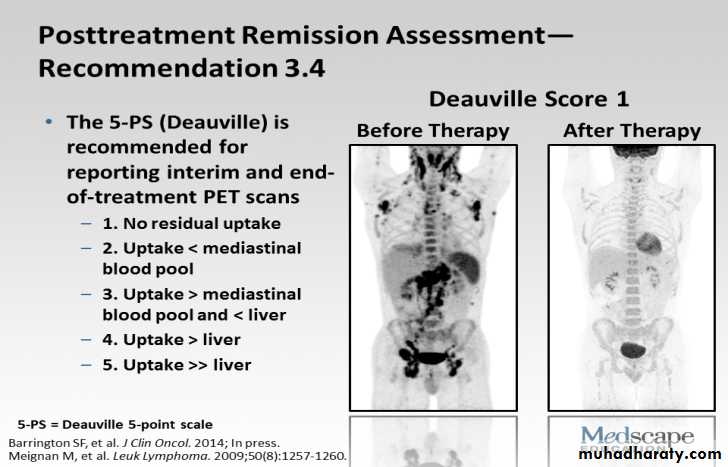
Management1-chemotherapy;The ABVD regimen (doxorubicin,vinblastine,bleomycin and dacarbazine)*cardiac and pulmonary toxicity, due to doxorubicinand bleomycin respectively.2-radiotherapy* The majority of HL patients are now treated withchemotherapy and adjunctive radiotherapy.* Early-stage patients usually includes additional treatment with radiotherapy to the involved lymph nodes after four courses of ABVD.* Advanced-stage disease are most commonly managed with chemotherapy alone. 6–8 cycles of ABVD.* Patients with disease which is resistant to therapy may be considered for autologous HSCT.* Treatment response is assessed clinically and by repeat CT and newerscanning modalities such as positron emission tomography (PET(
Prognosis
Non-Hodgkin lymphomaNon-Hodgkin lymphoma (NHL) represents a monoclonalproliferation of lymphoid cells of B cell (70%) or T cell (30%)origin.
working formulation for lymphoma classification• Low grade :• diffuse small lymphocytic.• follicular small cleaved cell.• follicular mixed small and large cell.• Intermediate grade :• diffuse small cleaved cell.• diffuse small and large cell.• diffuse large cell lymphoma.• follicular large cell lymphoma.• High grade :• immunoblastic lymphoma.• small non cleaved cell (Burkitt-type).• lymphoblastic lymphoma.
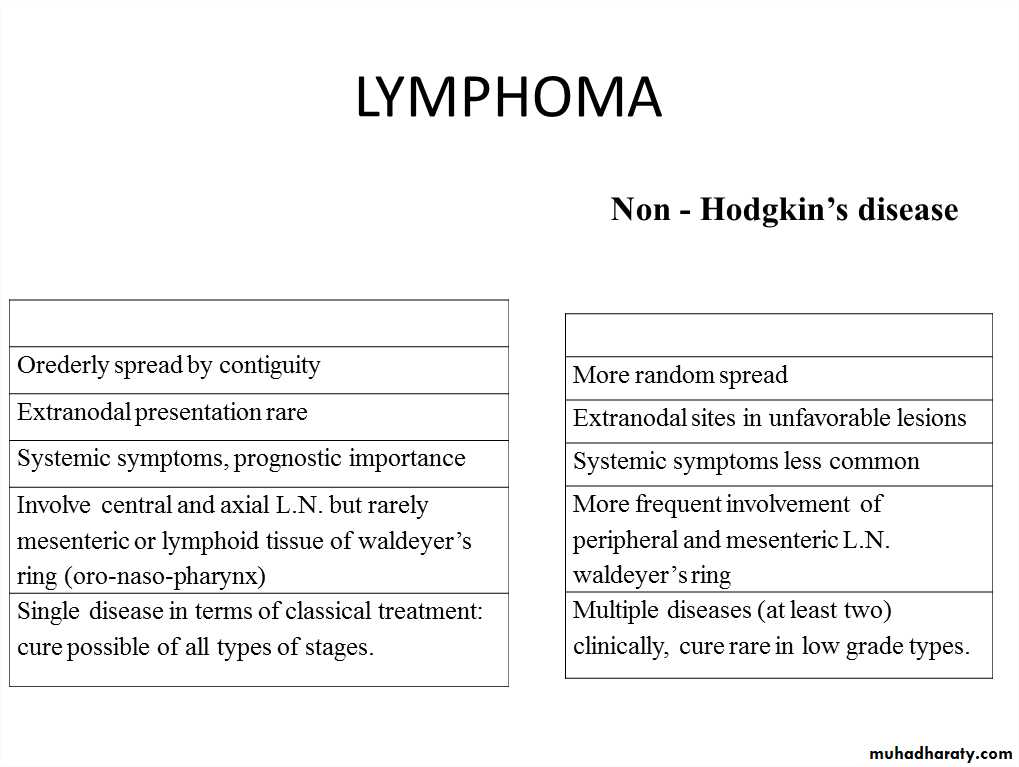
Clinical presentation1- most pt present with one or several enlarge painless LN. cervical, inguinaland axillary's nods are most frequently involved. Hepatosplenomegaly may bepresent2- 1/5-1/3 of pt with intermediate and high grade lymphoma present in extranodal site such as waldeyers ring, GIT, skin, salivary gland, bone.3- compression syndromes may occur, gut obstruction,ascites, superior vena caval obstruction and spinal cord compression.4 - BM involvement in high grade 10% and 50-60% in low grade.5- T cell lymphoma are usually first diagnosed in the skin lead to cutaneous T cell lymphoma (sezary syndrome), erthro-derma and circulating lymphoam cellswith hyper convoluted nuclei.**The same staging system is used for both HL and NHL, but NHL is morelikely to be stage III or IV at presentation.
InvestigationsSame as HD inaddition;1-Bone marrow aspiration and trephine.• 2-Immunophenotyping of surface antigens todistinguish T from B cell tumours.3-Cytogenetic analysis to detect chromosomaltranslocations.4-Immunoglobulin determination.5- Measurement of uric acid levels.6- HIV testing.
Treatment• Low grade NHL |:• A symptomatic pts may not require treatment• Radiotherapy : for stage I disease.• Chemotherapy : oral therapy with chlorambucil.• The anti-CD20 antibody rituximab.* Rituximab (R) in combination with cyclophosphamide, vincristineand prednisolone (R-CVP).**Transplantation.High-grade NHL *PrognosisChemotherapy; R-CHOPRadiotherapyHSCT