
1
4th stage
Obstetric
Lec:3
Dr.ahmed jasim
17/11/2015
Bleeding in Late Pregnancy (Antepartum Haemorrhage)
Objectives :-
-To know the causes of bleeding in late preg.
-To learn the clinical presentations of placenta previa & it management.
-To learn the complications of p.p .
Definition :-
It is bleeding from the genital tract after the 24th week of pregnancy and before the end of
the second stage of labour.
Stages of labour :
-stage 1 : cervix dilatation
-stage 2 : delivery of fetus
-stage 3 : delivery of placenta
Classification :
1-Placental site bleeding: (62%)
1-Placenta praevia (22%): Bleeding from separation of a placenta wholly or
partially implanted in the lower uterine segment.
2-Abruptio placentae (30%): Premature separation of a normally implanted
placenta.
3-Marginal separation(10%) : Bleeding from the edge of a normally implanted
placenta.
2-Non-placental site bleeding: (28%)
1-Vasa praevia: Bleeding from ruptured foetal vessels.
2-Rupture uterus.
3-Bloody show.
4-Cervical ectopy, polyp or cancer.
5-Vaginal varicosity.

2
placenta previa
Definition :
The placenta is partially or totally attached to the lower uterine
segment.
Incidence:
0.5% of pregnancies . It is more common in multiparas and in twin
pregnancy due to the large size of the placenta.
Aetiology :
Not well known but may be due to
1-Low implantation of the blastocyst.
2-Development of the chorionic villi in the decidua capsularis leading to attachment to
the lower uterine segment.
3-Large placenta as in twin pregnancy.
4-Older multipara.
5-Previous uterine damage and caesarean section.
6-Uterine abnormality.
7-Assisted conception.
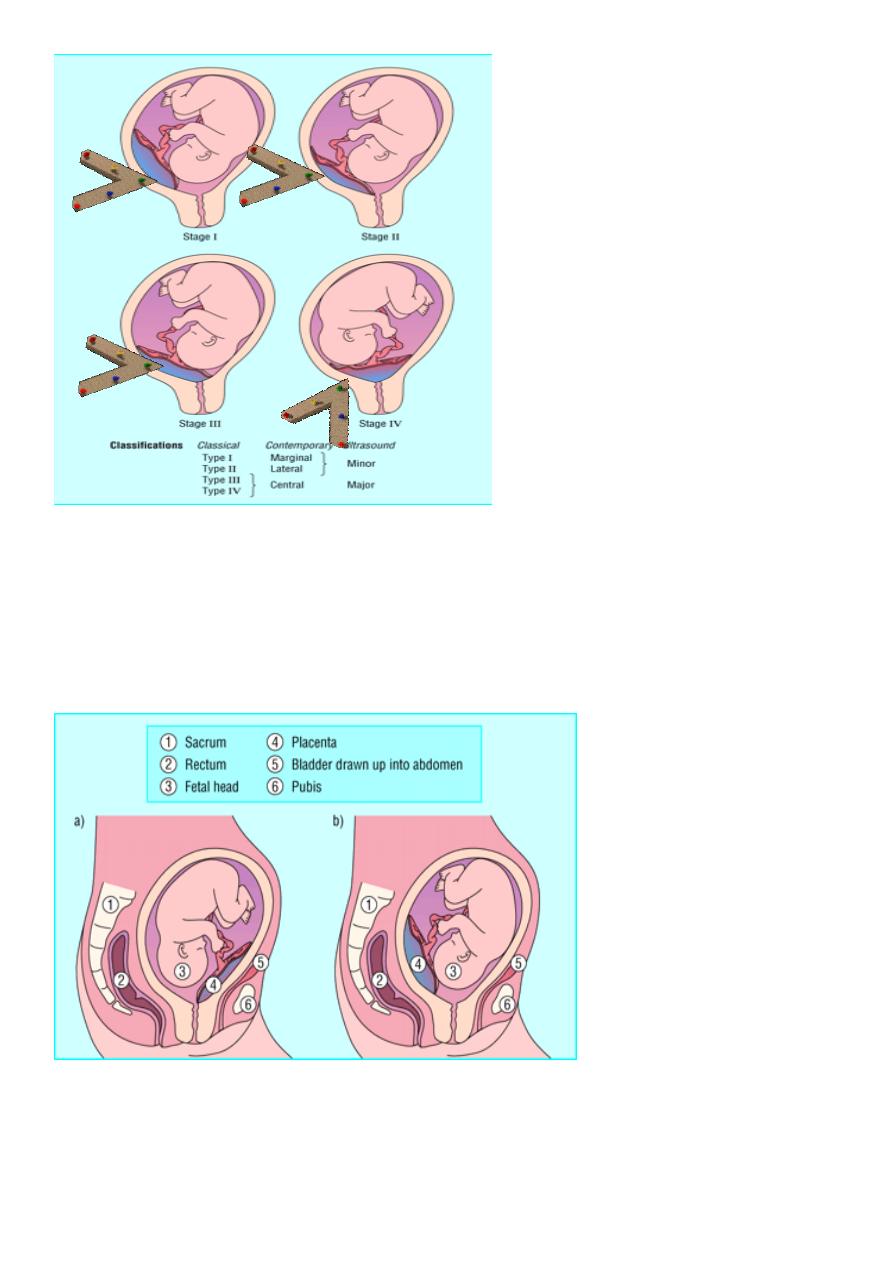
Degrees ( types ) :
-First degree (Type I = P.P. lateralis = low-lying placenta):-
The lower edge of the placenta reaches the lower uterine segment but not the internal
os.
-Second degree (Type II= P.P. marginalis):
The lower edge of the placenta reaches the margin of the internal os but does not cover
it.
-Third - degree (Type III= P.P. incomplete centralis):
The placenta covers the internal os when it is closed or partially dilated but not when it
is fully dilated.
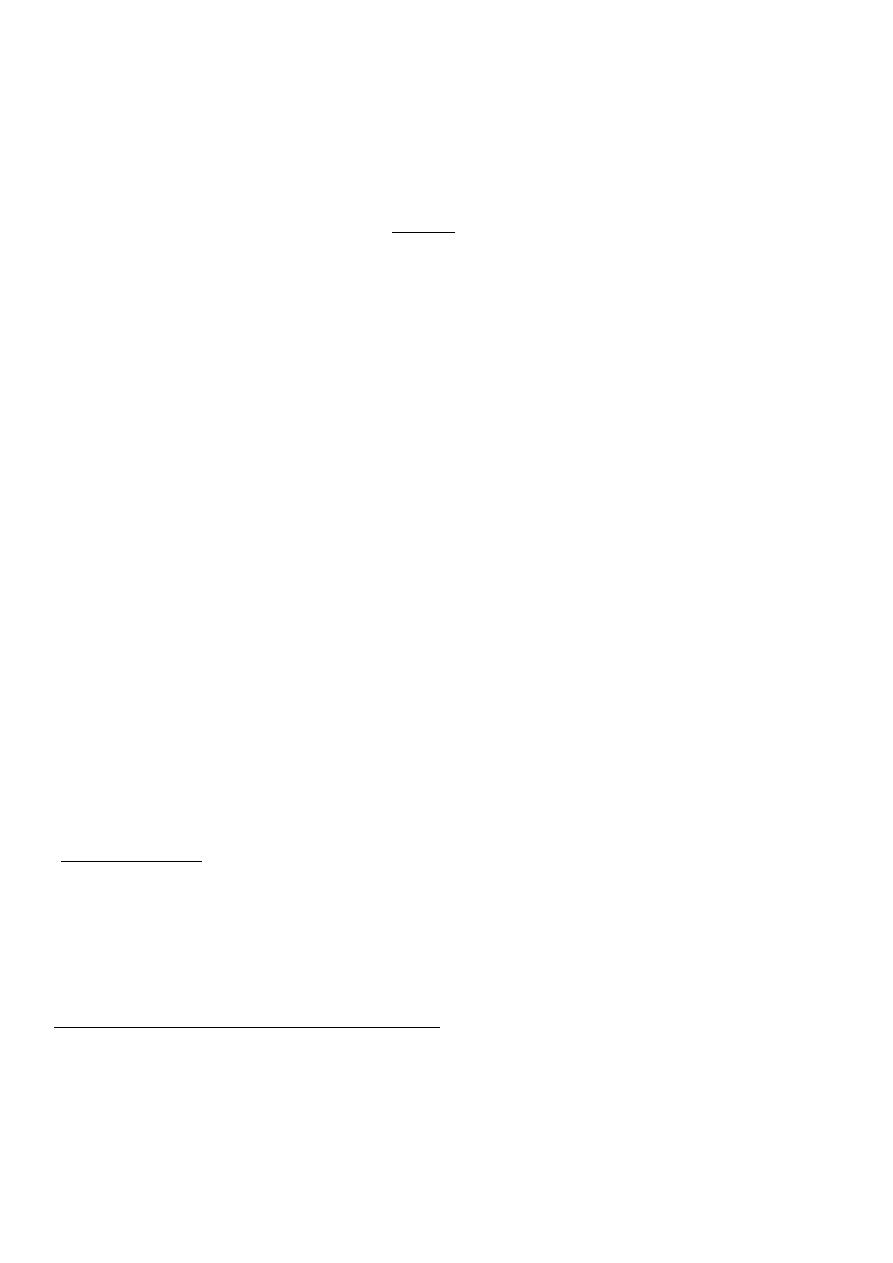
-Fourth - degree (Type IV = P.P. complete centralis):
The placenta covers the internal os completely whether the cervix is partially or fully
dilated.
3
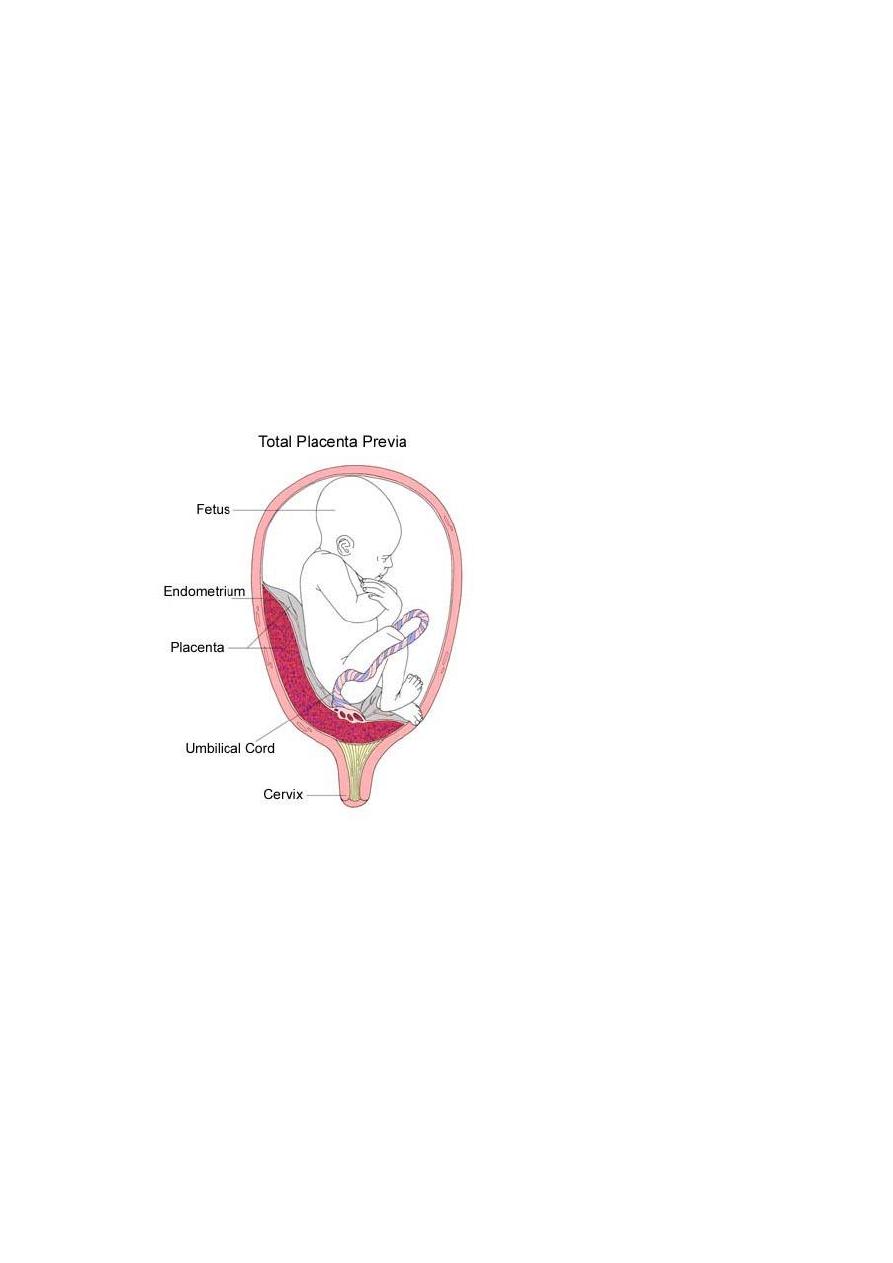
-Placenta praevia marginalis posterior is of bad prognosis than marginalis anterior
because It encroaches on the true conjugate diameter delaying engagement of the
head. Engagement of the head will compress the placenta against the sacrum, causing
foetal asphyxia.
•
Descending head can compress anterior placenta
praevia against pubis (left) but not posterior sited
placenta (right) as too much soft tissue intervenes

4
Mechanism of bleeding :
Progressive stretching of the lower uterine segment
normally occurs during the 3rd trimester and labour, but the inelastic placenta cannot
stretch with it. This leads to inevitable separation of a part of the placenta with
unavoidable bleeding. The closer to term, the greater is the amount of bleeding.
Pathology :
Placenta praevia is most dangerous for the mother.
The bleeding is from maternal circulation. Bleeding usually occurs for the first time
early in third trimester when the lower uterine segment begins to change, causing the
cervix to efface and dilate.
Bleeding is caused by the tearing of placental attachment at or near the internal os, as
the cervix changes. The bleeding continues because the stretched fibers of the lower
uterine segment are unable to contract and compress the torn vessels.
The bleeding is inevitable as cervix takes up and dilate.
The separation during pregnancy may be slight but it greater during labour where
severe bleeding occurs.
Diagnosis :
Symptoms :Causeless, painless and recurrent bright-red vaginal bleeding;
1-It is causeless, but may follow sexual intercourse or vaginal examination.
2-It is painless, but may be associated with labour pains .
3-It is recurrent, but may occur once in slight placenta praevia lateralis.
Fortunately, the first attack usually not severe.
Signs :
General examination:
The general condition of the patient depends upon the amount of blood loss. Shock
develops if there is acute severe blood loss and anaemia develops if there is
recurrent slight blood loss.
Abdominal examination:
-The uterus is corresponding to the period of amenorrhoea, relaxed and not
tender.
-The foetal parts and heart sound (FHS) can be easily detected.
-Malpresentations, particularly transverse and oblique lie and breech
presentation are more common as well as non-engagement of the head. This
is because the lower uterine segment is occupied by the placenta.
Vaginal examination :
5
-Speculum examination to exclude local lesions is only permissible when
placenta praevia has been excluded by ultrasound.
-P/V is indicated only if active treatment is initiated. This may provoke a
severe attack of bleeding so it should be done with the following
precautions:
1-In the operating room,
2-under general anaesthesia,
3-cross- matched blood is in hand,
4-operating theatre is ready for immediate caesarean section.
If the index finger is introduced gently through the dilated cervix, the
placenta can be felt as a tough fibrous mass.
Differential diagnosis : Other causes of antepartum haemorrhage.
Investigation :
-Ultrasound: It is the most simple, precise and safe method for placental localization.
A partially full bladder is necessary to identify the lower edge of the placenta. If it is
less than 3 cm from the margin of the internal os, it is diagnosed as placenta praevia.
The posterior placenta praevia is difficult to be identified due to shadowing from the
presenting part of the foetus. This can be overcome by head-down tilt of the patient or
displacing, the presenting part manually. If difficulty still present, the distance
between the presenting part and the promontory of the sacrum is measured. If this
exceeds 1.5 cm it means that placenta lies in-between.
In mid - pregnancy the placenta reaches the internal os in up to 20% of pregnancies.
With increasing gestational age and the formation of the lower uterine segment, a gap
6
develops between the placental edge and the internal os " placental migration". So it is
recommended to repeat scan when placenta praevia is diagnosed in mid - pregnancy.
-Soft tissue placentography, isotopes and thermography : are old methods for
placental localization that are obsolete nowadays .
condition when morbid adherence of
special
It is expensive and indicated in
:
MRI
-
placenta was suspected (accrete).
Treatment :
1. Gestational age.
2. Amount of bleeding.
treatment can be either:
1. expectant management
2. Delivery
At Home
-Arrange for immediate transfer to the hospital.
-No vaginal examination and no vaginal pack, only a sterile vulval pad is applied.
-No oral intake as anaesthesia may be required.
-Antishock measures as pethidine IM, fluids and blood transfusion may be given in the
way to the hospital if bleeding is severe.
At Hospital
-Assessment of the patient's condition, general and abdominal examination and
resuscitation if needed.
-At least 2 unites of cross matched blood should be available.
for:
Ultrasonography
-
A- differentiation between abruptio placentae (retroplacental haematoma in a normally
implanted placenta), marginal bleeding (separation of the margin of a normally
implanted placenta) and placenta praevia (in the lower uterine segment),
B- assessment of foetal viability age, position and presentation.
ment is carried out as following:
Then manage
If the patient is not in labour , Look to the amount of bleeding;
-If the bleeding is severe, continue antishock measures and do immediate caesarean
section .
-If the bleeding is slight,
look to the gestational age;

7
-If completed 37 weeks (36 weeks by some authors) or more, pregnancy is terminated by
induction of labour or caesarean section (see later). At this time, the foetus is mature and
the mother will be in a risk of severe haemorrhage as term approaches.
-If less than 37 weeks (36 weeks by others), conservative treatment is indicated till the
end of 37 (or 36) weeks but not more.
Conservative treatment:
-The patient is kept hospitalized with bed rest and observation till delivery.
-Anaemia should be corrected if present.
-Observation of foetal wellbeing.
-Anti-D immunoglobulin is given for the Rh-negative mother.
If the patient is in labour:
-Vaginal examination is done under the previously mentioned precautions. According to
the findings, the patient will be delivered either vaginally by amniotomy + oxytocin or by
caesarean section.
-Vaginal delivery is allowed if the following findings are fulfilled:
1-Placenta praevia is lateralis or marginalis anterior,
2-bleeding is slight,
3-vertex presentation,
4-adequate pelvis with no soft tissue obstruction.
5-partially dilated cervix to allow amniotomy. Amniotomy has 2 benefits:
1-Allows descent of head so it compresses the placental site preventing further bleeding.
2-It abolishes the shearing movement of the placenta during uterine contractions. As the
bulging of fore bag of water during contractions with intact membranes will drag the edge
of the placenta evoking more bleeding.
Caesarean section is indicated in:
1-Placenta praevia centralis whether complete or incomplete even if the foetus is dead.
2-Placenta praevia marginalis posterior.
3-Severe bleeding.
4-Presentation other than vertex.
5-Other obstetric indications as contracted pelvis, cord prolapse and elderly
primigravida.
6-Vasa praevia
8
Although upper segment C.S. is sometimes advocated to be away from the placenta,
lower segment C.S. is preferable because:
-It allows better control of bleeding from the placental site.
-It leaves a stronger scar can withstand subsequent vaginal delivery.
-If placenta praevia was anteriorly implanted it is gently displaced laterally to reach the
foetal head otherwise cut through it (not preferred).
Complication of placenta previa :
1-Maternal: Maternal mortality rate is 0.2%.
:
pregnancy
During
-
a
-Abortion.
-Preterm labour.
-Antepartum haemorrhage.
-Malpresentation and non-engagement.
During labour:
-
b
-Premature rupture of membranes.
-Cord prolapse.
-Inertia.
-Obstructed labour.
-Postpartum haemorrhage.
-Retained placenta.
-Placenta accreta due to deficient decidual reaction in the lower segment
allows deep penetration of chorionic villi. This may necessitate
hysterectomy.
-Lacerations of lower uterine segment due to increased vascularity and
friability.
-Air embolism due to low placental site.
2-Foetal: Foetal mortality rate is 20 %.
Prematurity.
Asphyxia.
Malformations (2%).
SH.J