Immunopathology
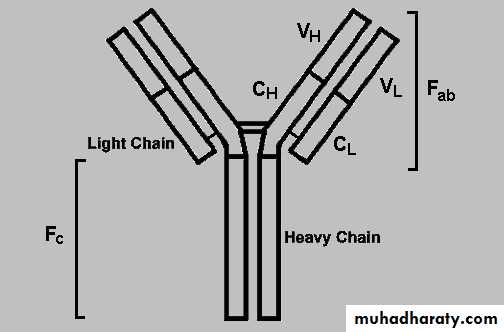
Structure of immunoglobulin
Type I hypersensitivity reaction: a cross linking of IgE antibodies on the surface of mast cells following re exposure to the antigen leading to degranulation of mast cells & release of mediators of inflammation.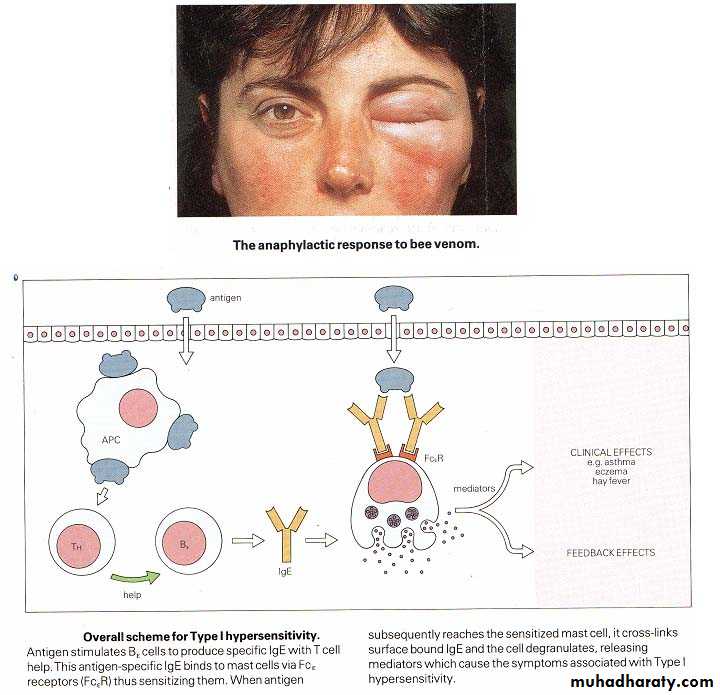
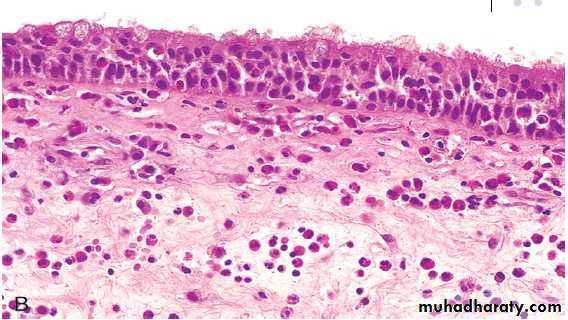
Chronic inflammation due to type I hypersensitivity reaction: Nasal mass with edematous stroma with chronic inflammatory cell infiltrate ( mainly eosinophils) covered by ciliated columnar epitheliumDiagnosis: allergic nasal polyp.
Antibody –mediated (type II) hypersensitivity
Is mediated by antigen present on cell surface by one of the following mechanisms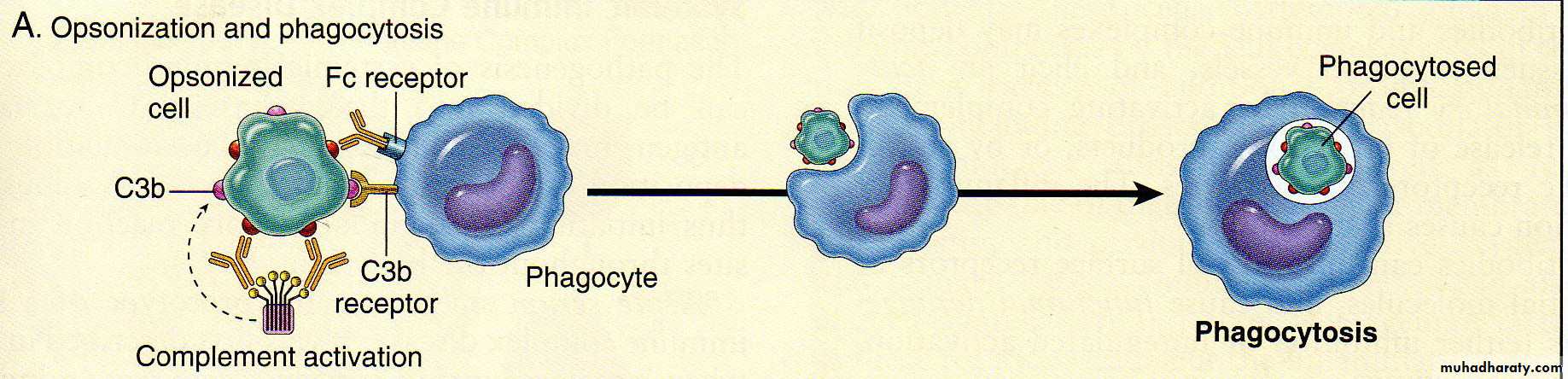
Opsonization of cell by antibody & complement followed by phagocytosis
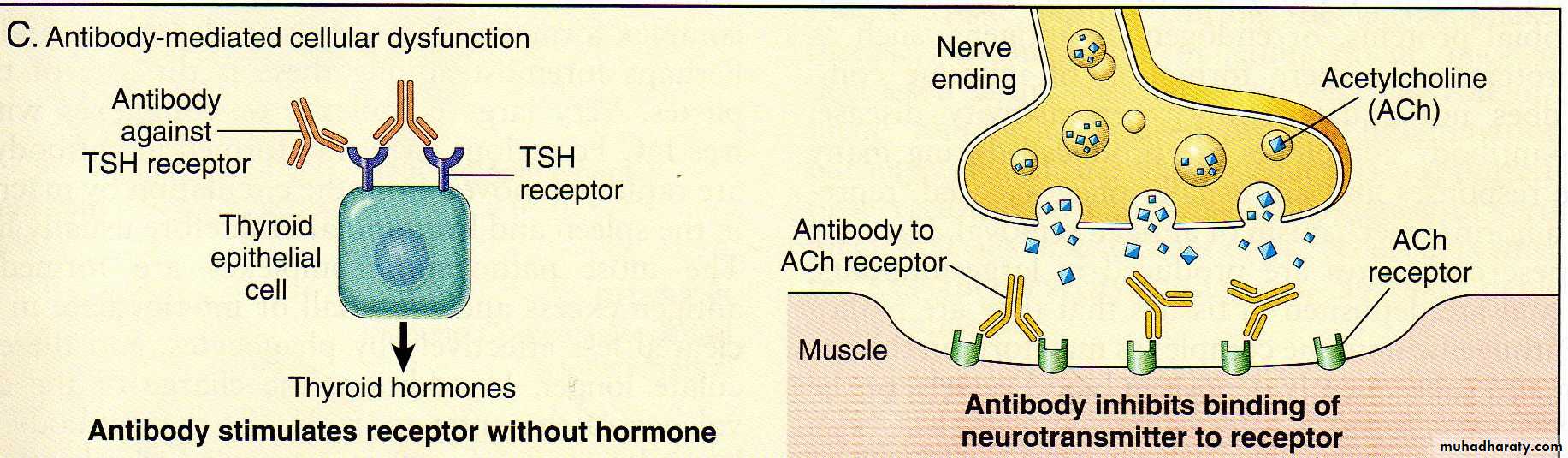
Anti-receptor antibodies disturb the normal function of the receptor leading to either impairment of cell function or stimulation of cells
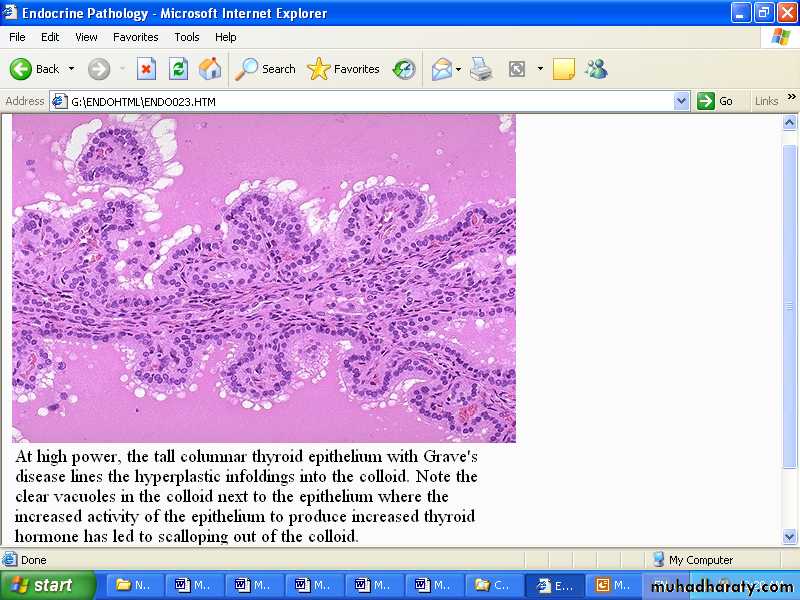
Antibodies to TSH-receptors activate thyroid cells in Grave’s disease leading to hyperplastic infolding into the colloid which show clear vacules next to the epithelium
Immune complex mediated (type III) hypersensitivity : the pathologic reaction is initiated when antibodies combine with circulating or fixed antigens & then deposited in the vessel wall & basement membranes producing local inflammation
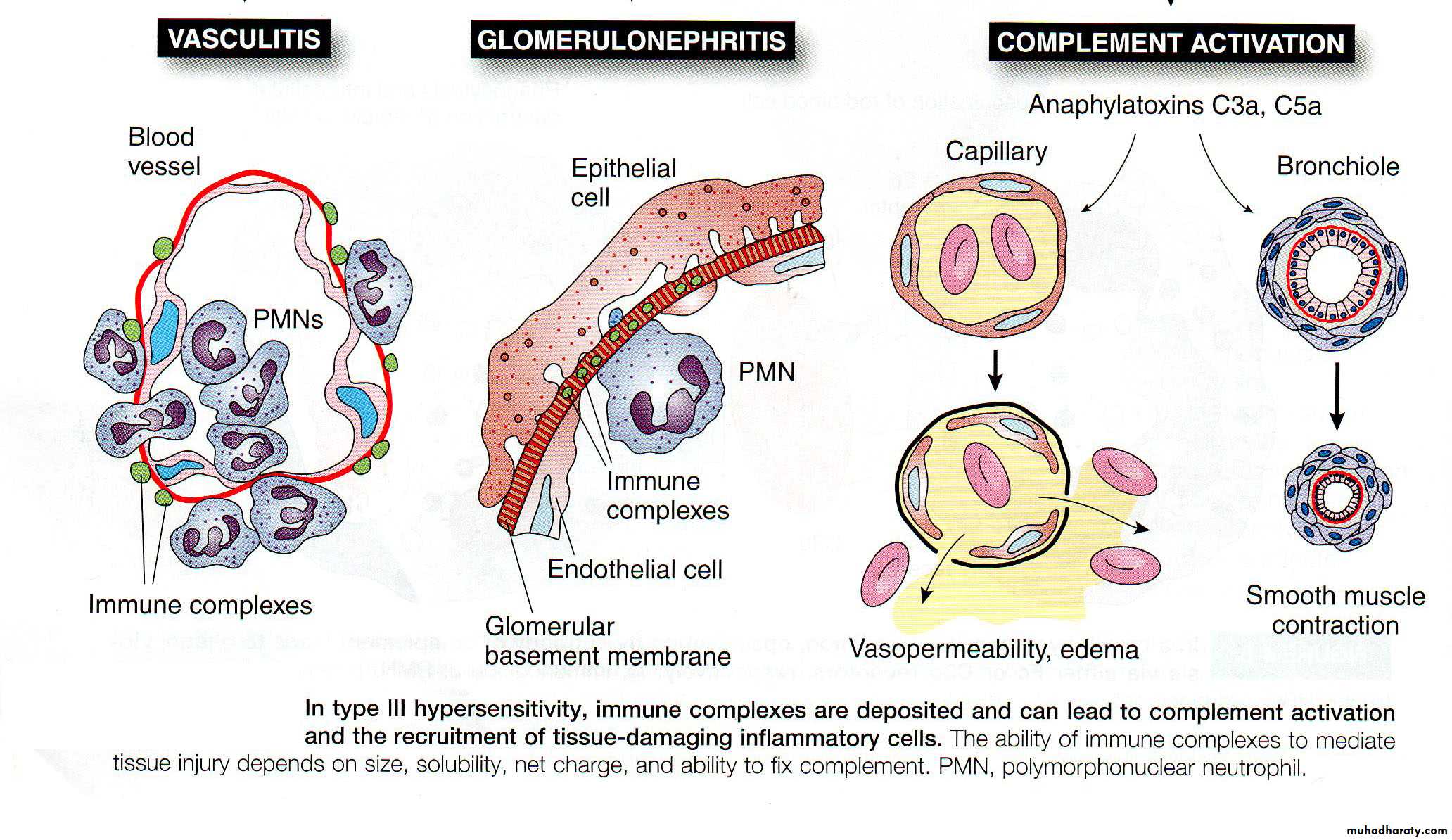
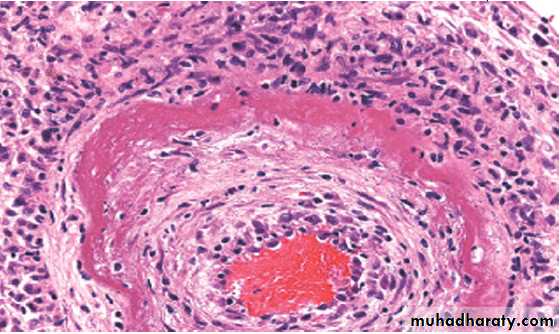
The deposition of immune complexes in an artery is called vasculitis with circumferential bright pink area of fibrinoid necrosis with protein infiltration & inflammation
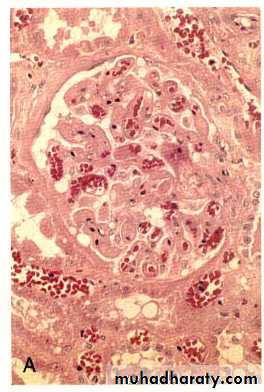
a glomerulus with subendothelial deposites of immune complexes (PAS stain)
IgG antibodies detected in granular pattern by immunoflourescenceCell mediated (type IV) hypersensitivity : the antigen presented by dendritic cell ( antigen presenting cell) leads to activation of TH1 cell which secrete cytokines that activate macrophages to form epitheliod cells & granuloma.
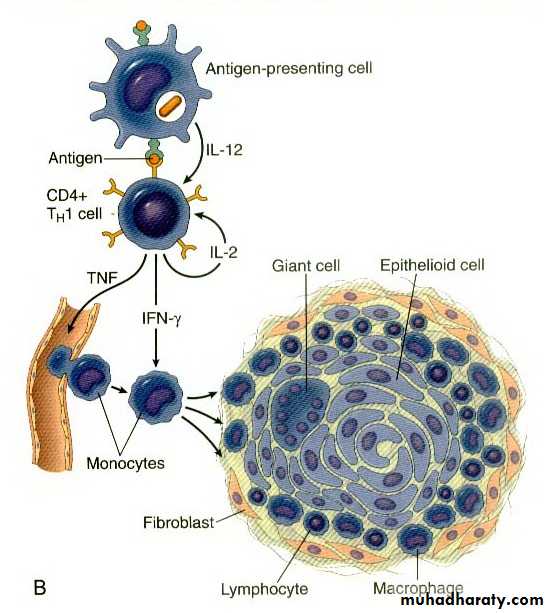
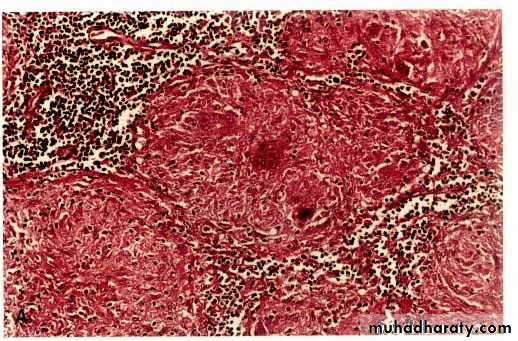
The granuloma is composed of localized collection of epitheliod cells surrounded by lymphocytes

It is a complex immunologic phenomenon involving both cell & Ab mediated hypersensitivity responses of the host directed against histocompatibility molecules on the donor allograft
TRANSPLANT REJECTION
It is a complex immunologic phenomenon involving both cell & Ab mediated hypersensitivity responses of the host directed against histocompatibility molecules on the donor allograft
TRANSPLANT REJECTION
Hyper acute rejection of a kidney allograft showing endothelial damage, platelet & thrombin thrombi in the glomerulus

Acute vascular rejection of the kidney with inflammatory cells in the interstitium& in between the tubules
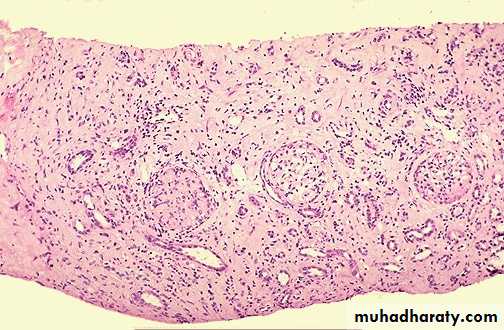
Chronic rejection of the kidney is dominated by interstitial fibrosis, tubular atrophy & loss of renal parenchyma due to arteriolosclerosis of arteries
Amyloidosis

Macroscopically the affected organ enlarged, firm & has waxy consistency
By H&E the amyloid appears as an amorphous, eosinophilic hyaline extra cellular substance that with progressive accumulation lead to pressure atrophy of adjacent cells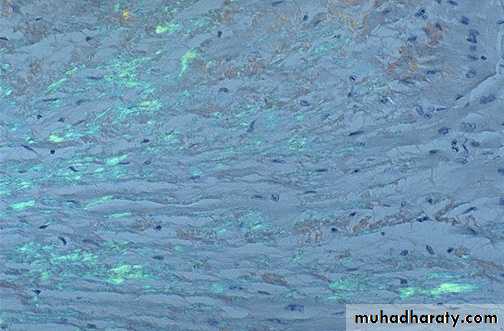
Note the yellow-green birefringence of amyloid in the heart with polarized microscope
In the heart, amyloid deposits begin to accumulate within the myocardium between muscle fibers & in the wall of blood vessels as seen by H&E as amorphous eosinophilic hyaline (right) & congo red stains as red deposits (left)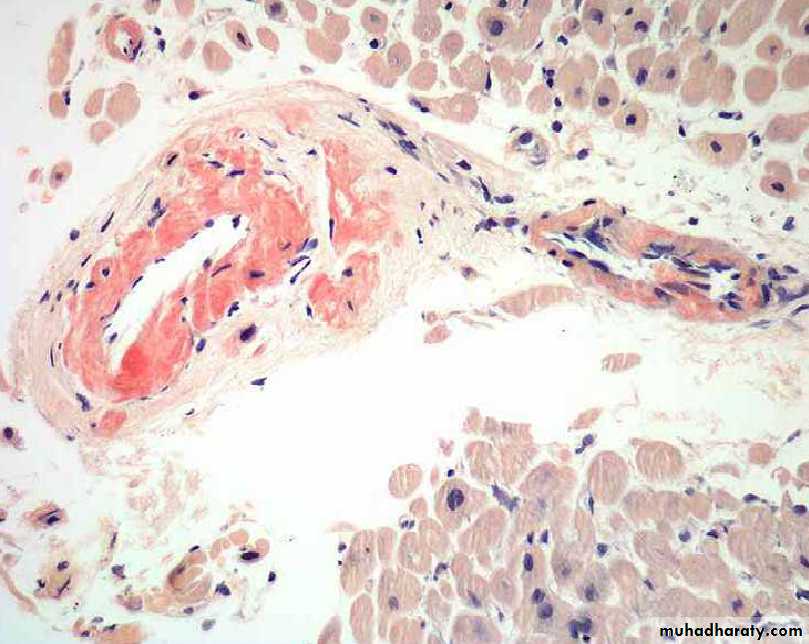
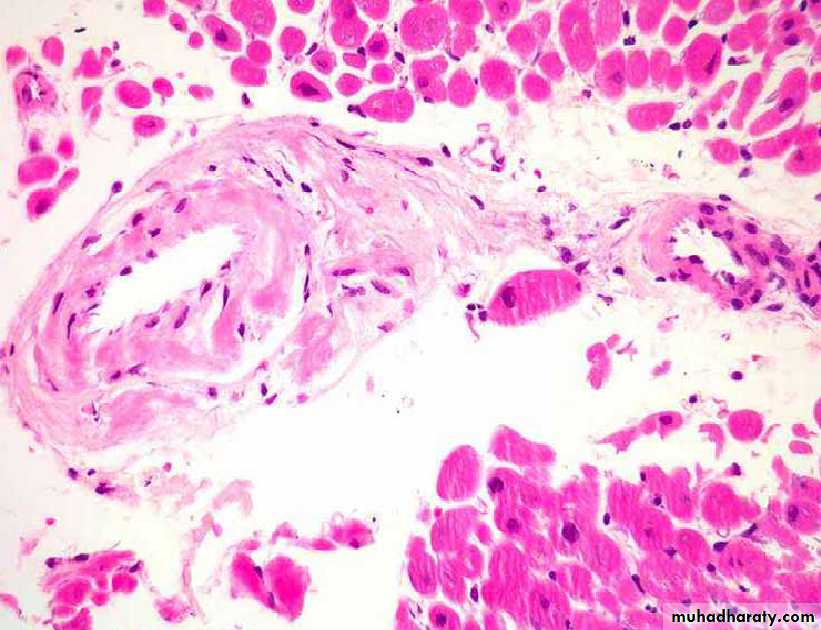
H&E stain
Congo red stainIn the kidney the amyloid is deposited primarily in the glomeruli, interstitial peritubular tissue, arteries & arterioles as amorphous eosinophilic areas by H&E.
A section of liver stained with congo red reveals pink-red deposits of amyloid in the wall of blood vessels & along the sinusoids
Note the yellow green birefringence of the deposits in the wall of blood vessels & sinusoids when observed by polarizing microscope
In adrenal gland the amyloid is deposited in the interglandular tissues & the wall of arterioles as an amorphous eosinophilic material as seen by H&E