pleurae
RadioLoGY
lecture
3
جامعة بغداد
–
كلية الطب
Introduction
ؤيد
م بتكم
MUSTAFA JASIM
Dr Laith
RADIOLOGY
INTRODUCTION: PLEURAE
PAGE 1
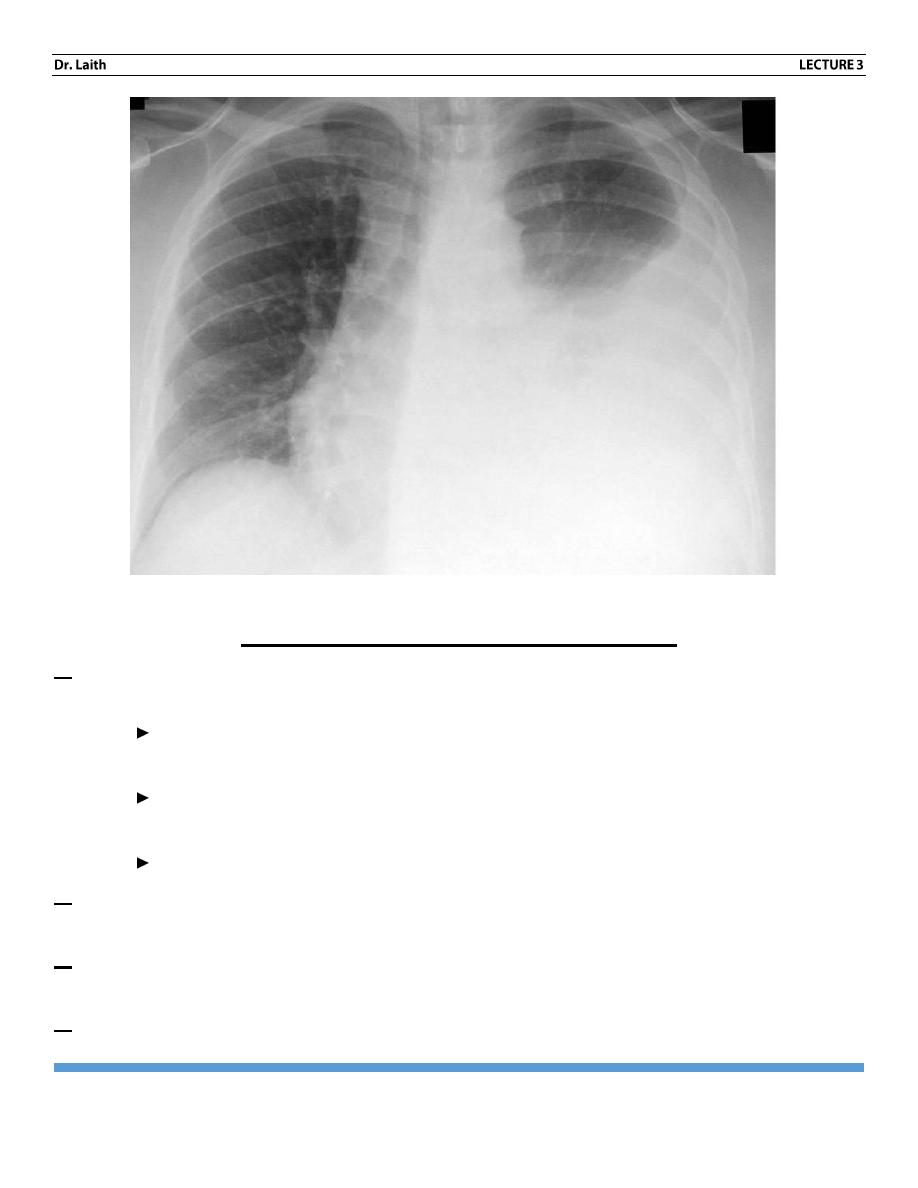
The pleurae
Pleurae effusion the presence of fluid in the pleural cavity, which can to
transudate ,exudates, pus or blood all have same radiographic features.
Pleural fluid free fluid collects in the most dependent part of the pleural cavity and
always fills the costophrenic angles. Free fluid assumes 2 basic shapes usually in
combination.
Usually the fluid surrounds the lung, higher laterally than medically at
also runs in to the fissures particularly in to the lower end of the oblique
fissures.
Sometimes oven with large pleural effusions, little or no fluid is seen
running up the chest wall. The fluid is then known as (subpulmonary
effusion). The upper border of the fluid is mush the some shape as the
normal diaphragm and since the true diaphragm is obscured by the fluid.
It may be very difficult or even impossible to tell from the standard erect
film if any fluid is present all , so take the film the patient on his side
(lateral decubitus view).
Loculated pleural fluid – pleural effusion may become loculated by pleural
adhesion, although loculations occur in all types of effusion, it is a particular
feature of empyema .
RADIOLOGY
INTRODUCTION: PLEURAE
PAGE 2
The role of U/S in pleural effusion
1. Infection pleural effusion due to pneumonia is usually small and pneumonia is
usually the dominant feature on CXR
Large loculated is usually the dominated with pneumonia often indicates
empyema formation.
Also large effusion can be present with TB and it may be the only visible
abnormality.
Sub phrenic abscess nearly always produce a pleural effusion.
2. Malignant neoplasm: malignant effusion are frequently large. They occur with
pleural metastasis, but the pleural deposits themselves are not seen by CXR.
3. Pulmonary infarction: effusion are usually small and accompanied by the lung
shadow caused by pulmonary infection.
4. Cardiac failure: effusions are usually bilalateral , often larger on the RT than Lt.
RADIOLOGY
INTRODUCTION: PLEURAE
PAGE 3
5. Collagen vascular disease: pleural effusion, either unilateral or bilateral are
common in collagen vascular disease.
6. Nephrotic syndrome, renal failure and ascites are all associated with pleural
effusion.
Pleural thickening (pleural fibrosis)
Fibrotic pleural thickening (scarring), especially in the costophrenic angles may
follow resolution of a pleural effusion it may be difficult on CXR so US or CT
resolve the problem.
Pleural tumors
The commonest Pleural tumor is metastatic. Primary pleural tumor for example
mesothelioma are uncommon pleural tumor produce lobulated musses bused on
pleura.
malignant pleural tumors (both primary and secondary frequently produce
pleural effusion)
Pleural
calcification
Either unilateral (due to old empyema or old hemothorax) or bilateral (often
related to asbestos exposure).
RADIOLOGY
INTRODUCTION: PLEURAE
PAGE 4
Note: asbestos exposure is associated with pulmonary fibrosis pleural thickening,
pleural
calcification
and
mesothelioma.
Pleural calcification due to TB
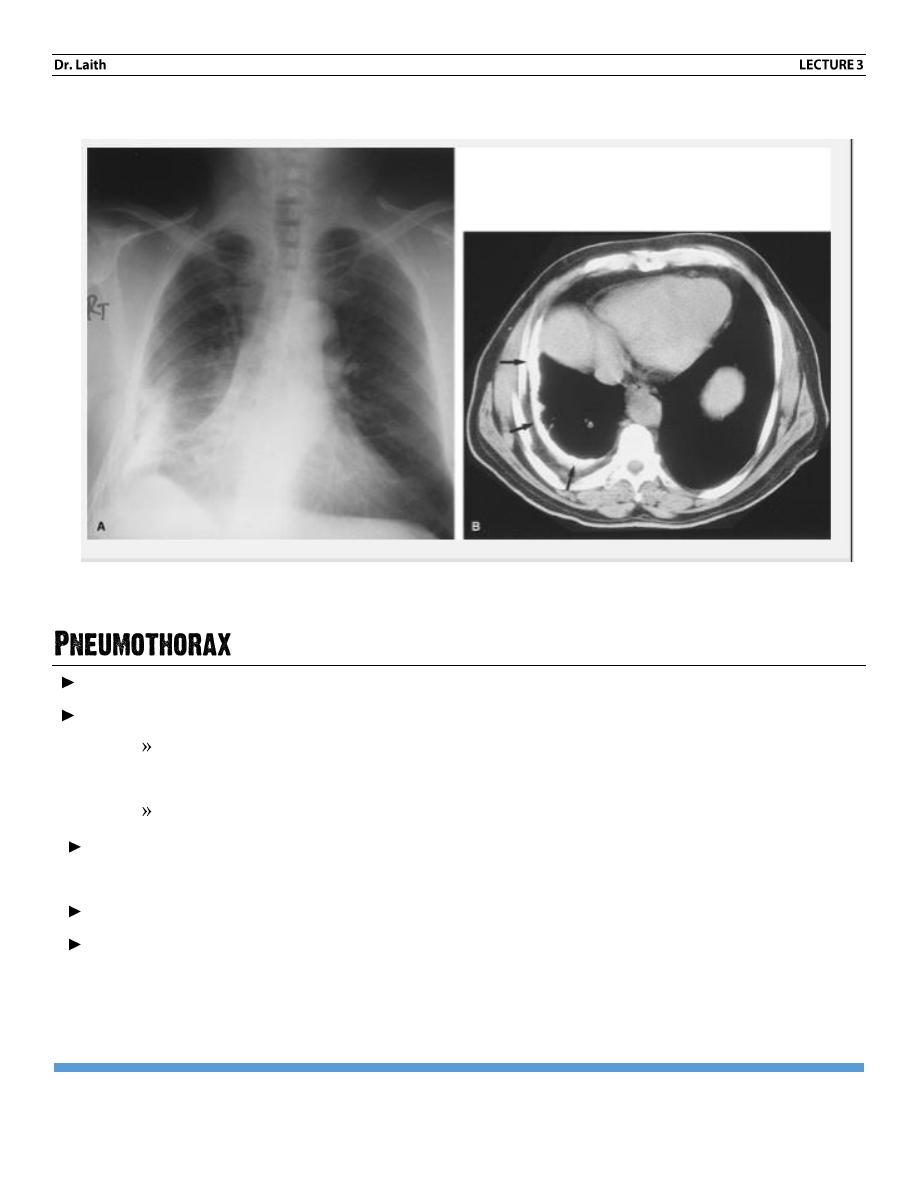
Air within the pleural cavity.
The diagnosis of pneumothorax depends on recognizing
A line of pleura separated by air from the chest wall. Mediastinum or
diaphragm.
Lack of vessels beyond this line-
Unless the pneumothorax is very large, there may be no appreciable increase
density of the underlying lung.
Sometimes pneumothorax is more obvious on expiratory film.
With tension pneumothorax, there will be mediastinal shift with Flattening of
diaphragm and the pneumothorax is usually large.
RADIOLOGY
INTRODUCTION: PLEURAE
PAGE 5
Causes of pneumothorax:
The majority occur in young people with no recognizable lung disease, these
patients have small blebs or bullae at the Periphery of the lung that burst.
Emphysema
Certain forms of pulmonary fibrosis
Pneumocystis carinii pneumonia.
Metastases (rarely).
TB
Trauma
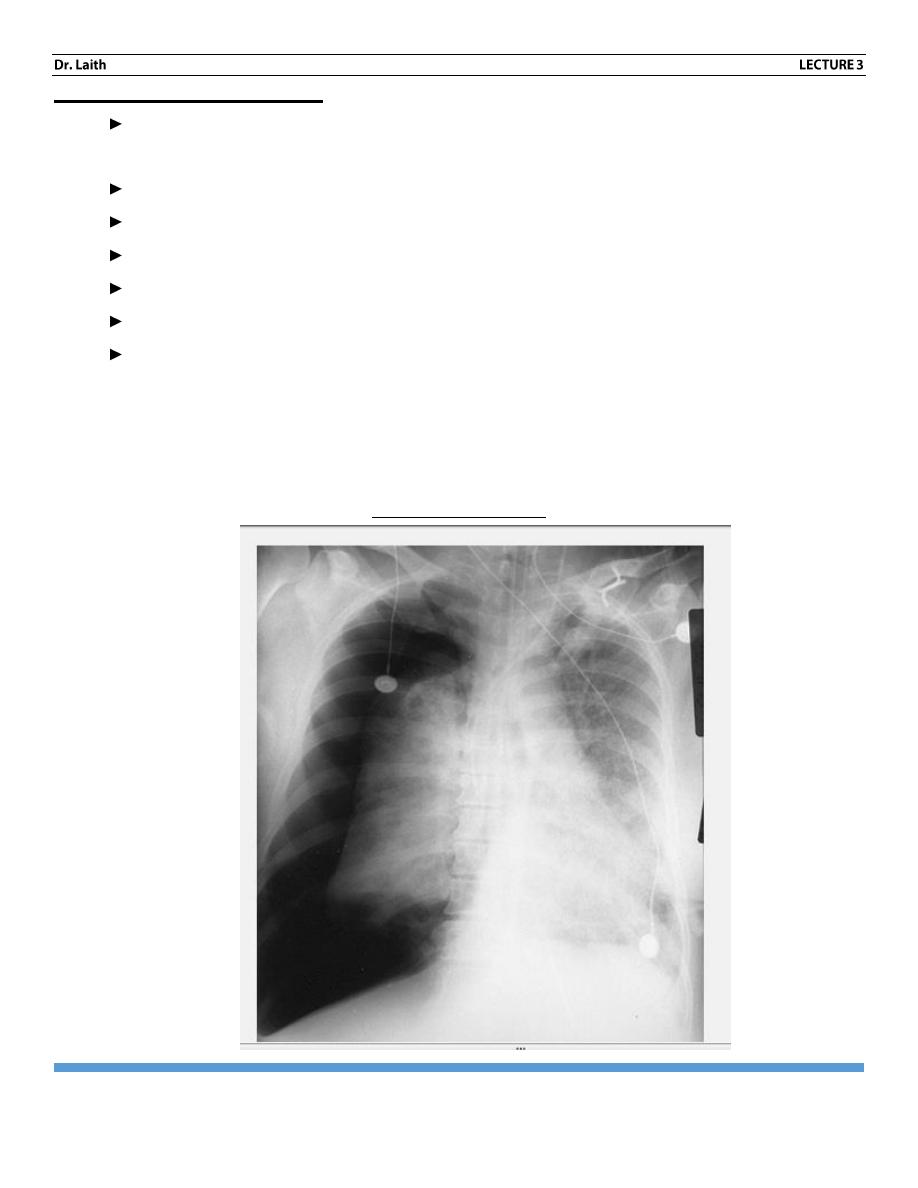
Hydropneumothorax, haemothorax and pyopneumothorax fluid in the pleaural cavity
(pleural effusion, blood, pus) assume different shape in the presence of pneumthorax,
the diagnostic feature is air fluid level.
Tension pneumothorax
RADIOLOGY
INTRODUCTION: PLEURAE
PAGE 6
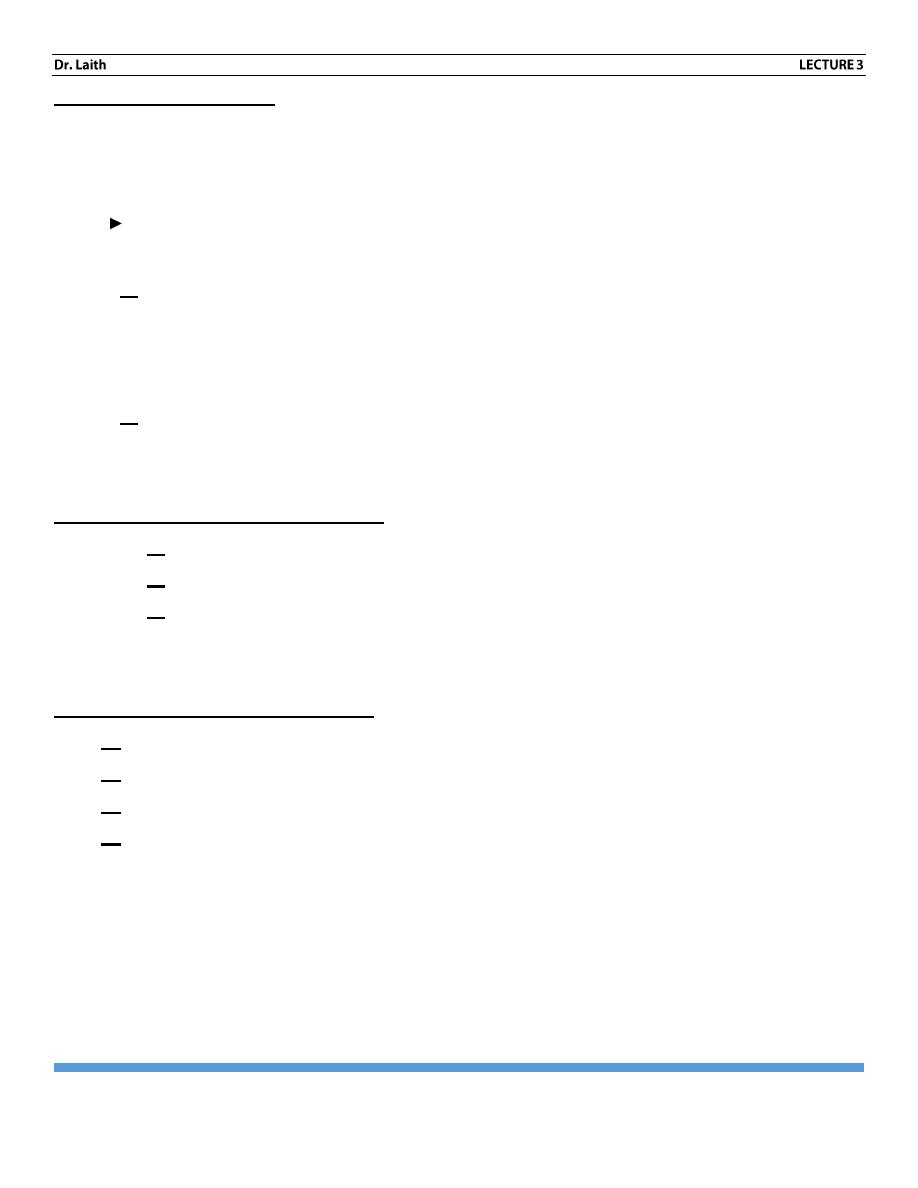
Hilar enlargement:
The normal hilar shadow are composed of pulmonary arteries and veins , the hilar
LN are too small to be seen when normal ,and the walls of the central bronchi are
too thin to contribute to hilur shadows.
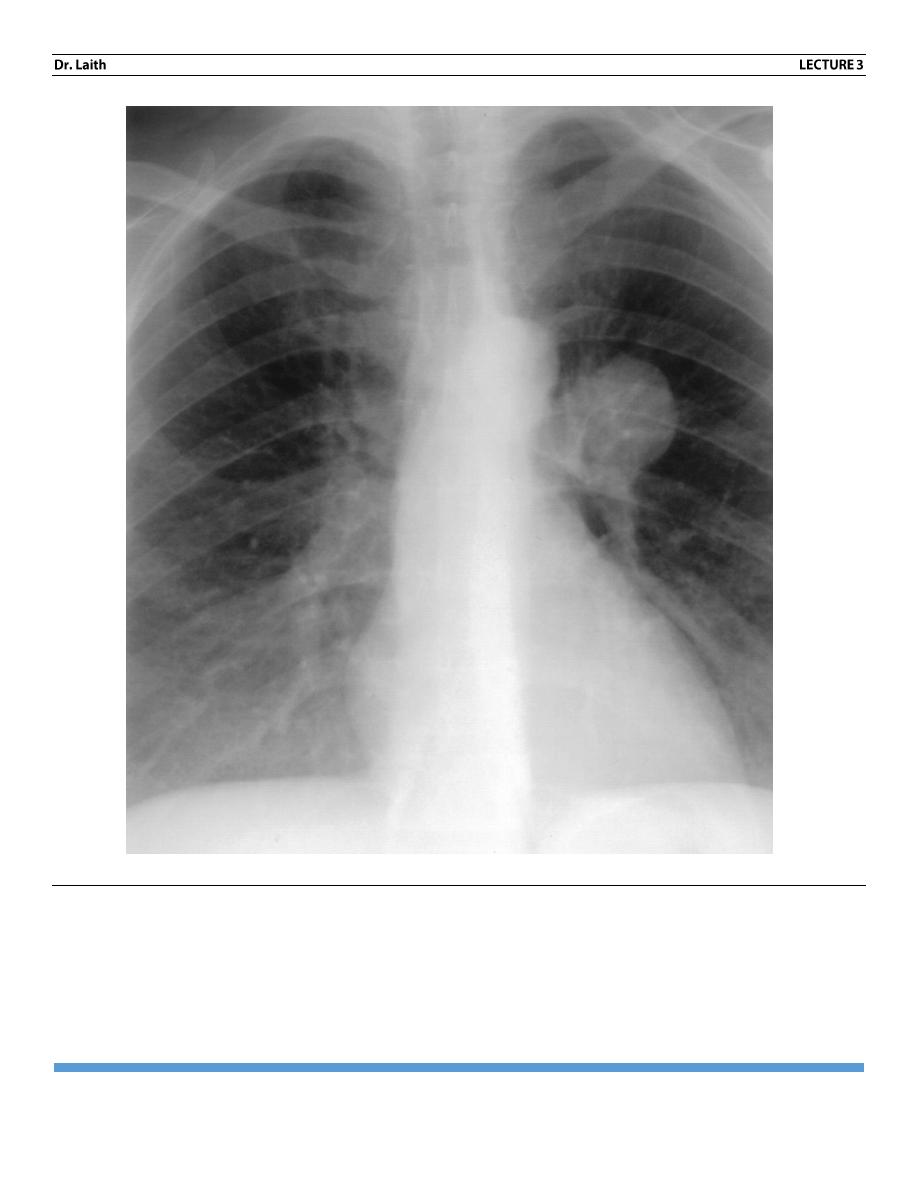
Enlarged hilum is either large blood vessels or mass. Hilar mass is either an
enlarged LN or CA bronchus. To differentiate between the two:
1. Enlargement of pulmonary arteries Is usually bilateral, and both hila
show a branching pattern and accompanied by enlargement of main
pulmonary artery and heart. Same causes of pulmonary artery enlargement
are pulmonary artery hypertension, increase pulmonary blood flow.
2. Hilar LAP: usually more than ONE lymph node is enlarged, so the hilum
appears lobulated on outline, it is ether unilateral or bilateral.
Unilateral hilar enlargement
: may be due to
1. Metastasis from CA Bronchus
2. Malignant lymphoma.
3. Infection (TB, histoplasmosis)
TB is the commonest cause of unilateral hilar enlargement in children
Bilateral hilar enlargement
: may be due to
1- Sarcoidosis
2- TB
3- Lymphoma
4- Fungal disease.
Neoplasm – primary CA broaches frequently present, if lobar collapse
consolidation or narrowing of the adjacent bronchus is visible, the diagnosis of CA
is virtually certain.
RADIOLOGY
INTRODUCTION: PLEURAE
PAGE 7
Hilar Mass
The END
RADIOLOGY
INTRODUCTION: PLEURAE
PAGE 8
تصحيح
في
محاضرة رقم
-
1
-
في
( الصفحة رقم
5
( ) في النقطة
2
)
bony structures
الفقرة
(
a
)
increase bone
disease
تغيير
المرض الثاني
porosis
osteo
إلى
PETROSIS
osteo
.
البوروسيس
هو هشاشة العظام لهذا تقل كثافة العظم
وتبين على بياض خفيف
بينما
المرض الثاني هو
األوستيوبيتروسس
وهو
تصخر العظام
وبي تزداد كثافة العظام لهذا تبين باألشعة بياض أكثر ألن بي كالسيوم
أكثر فيمتص أشعة
سينية
أكثر
ويبين أكثر
.
صور
توضيحية قد تفيدكم
RADIOLOGY
INTRODUCTION: PLEURAE
PAGE 9
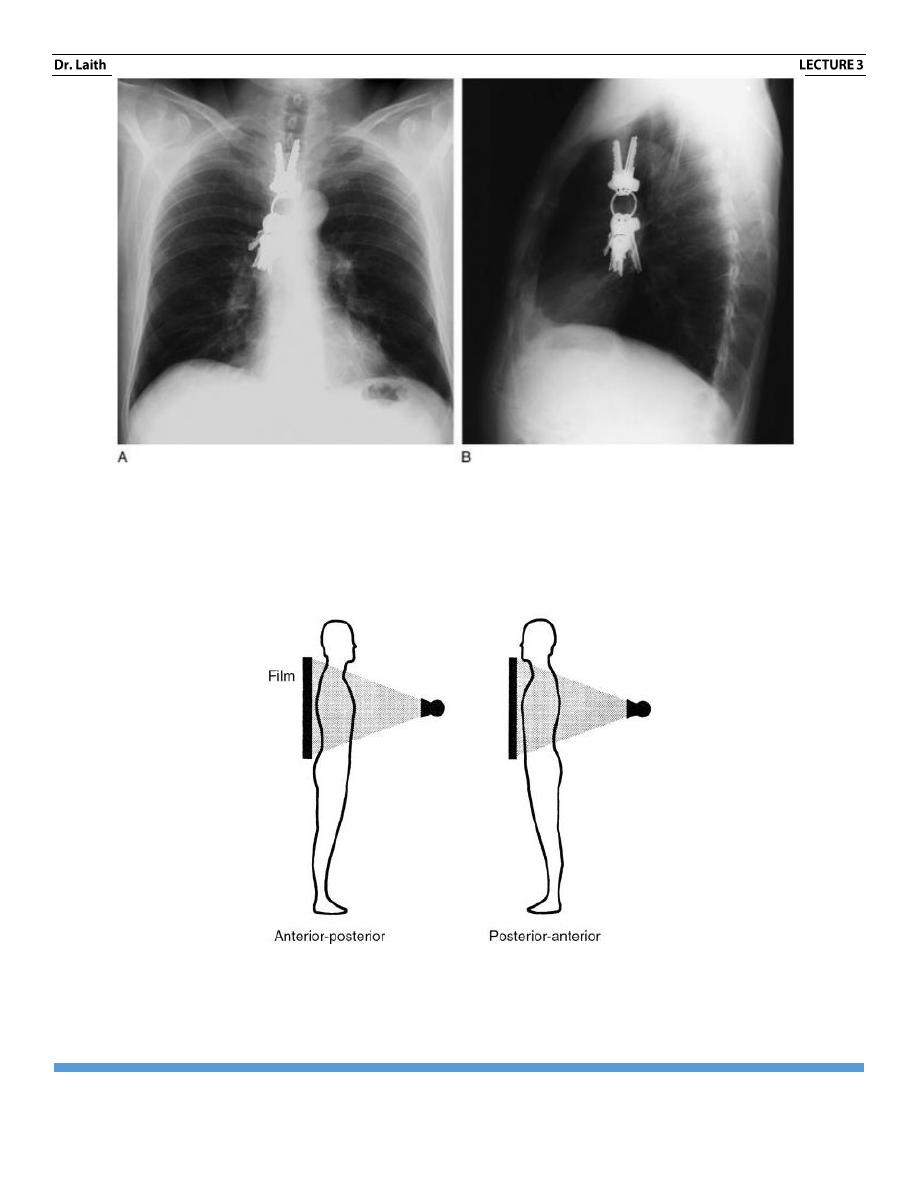
What is the location of the keys? On both the posteroanterior (PA) view of the chest (A) and the
lateral view (B), the keys seem to be within the center of the chest. Actually if you look
carefully, you will notice that the keys do not change position at all, even though the patient has
rotated 90 degrees. The keys are located on the receptor cassette and are not in the patient.
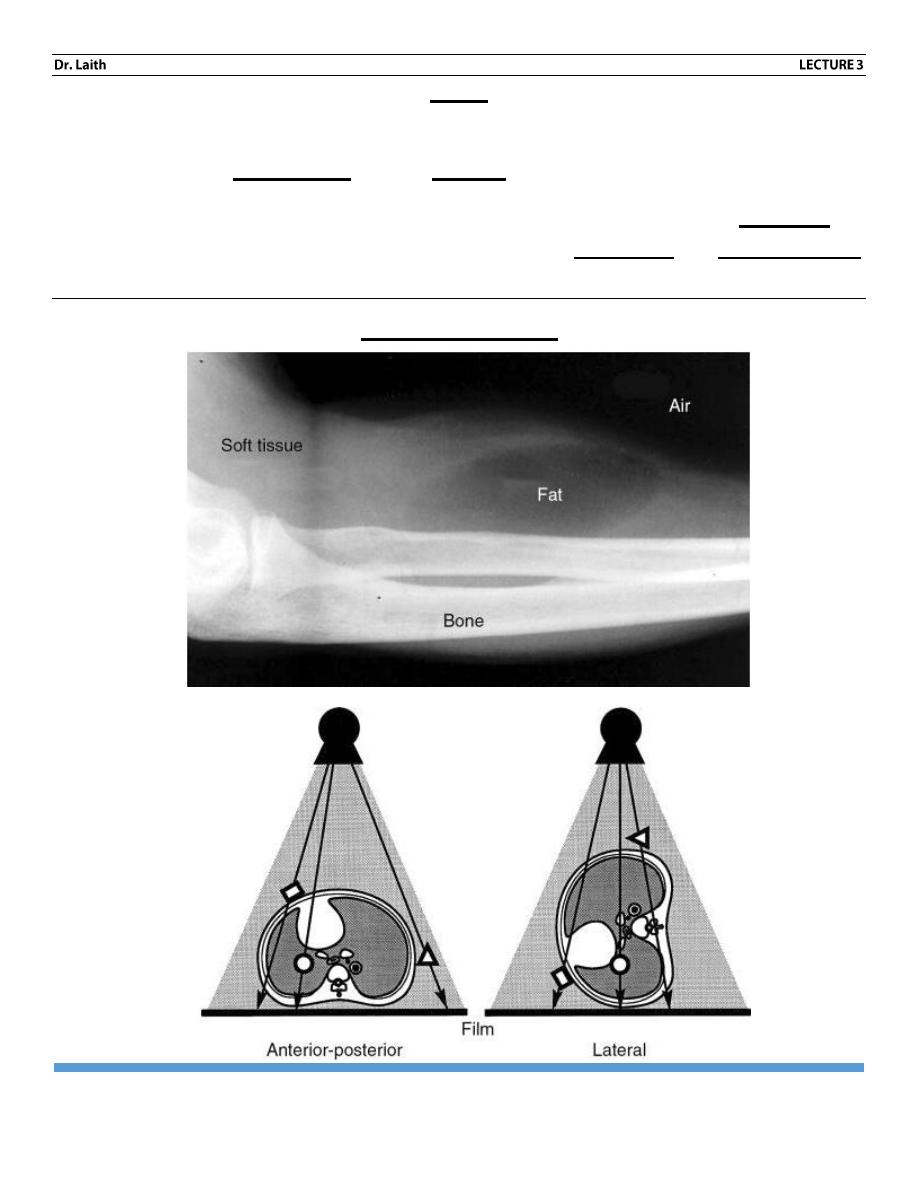
Figure 1-4 Typical x-ray projections. X-ray projections are typically listed as AP or PA. This
depends on whether the x-ray beam passed to the patient from anterior to posterior (AP) or the
reverse. Lateral (LAT) and oblique (OBL) views also are commonly obtained.
RADIOLOGY
INTRODUCTION: PLEURAE
PAGE 10
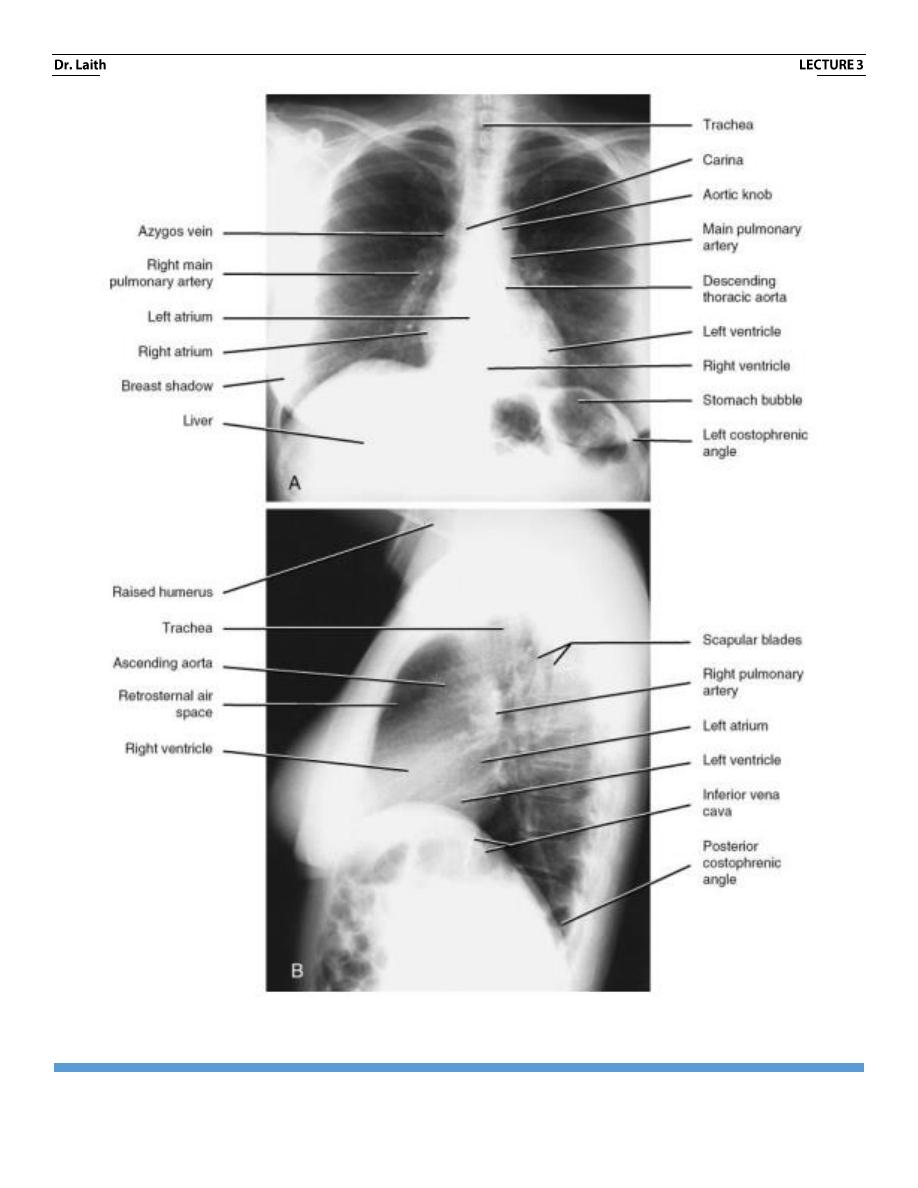
Normal anatomy of chest in PA view and lateral view
RADIOLOGY
INTRODUCTION: PLEURAE
PAGE 11
WHEN I’M EDITING THE LECTURE AND SO MANY CORRECT WORDS