Visceral Leishmaniasis
(Kala‐Azar; Black Fever)
P R O F E S S O R A B D E L G H A N I A L R A W I
©
2
0
0
9

The causative agent is
Leishmania donovani
from Leishmania
species. Disseminated hematogenously and infect the
reticuloendothelial system. It is a diseases characterized by
irregular fever, emaciation & splenomegaly. It is a zoonotic
disease in which dogs & other carnivores are the reservoir.
Leishmania has two morphological forms
promastigote
(flagellated from) &
amastigote
(aflagellated form).
February 27, 2009
2
Kala Azar

Life cycle:
Flagellar
promastigote
are introduced by the feeding female sand
fly. Sand fly saliva helps Leishmania evade immunity.
The promastigote are taken up by macrophages where they lose
their flagellae and transform into
amastigotes
. These multiply,
ultimately causing lysis of macrophages and infection of another
cell.
Sand flies pick up amastigotes when feeding on infected patient or
animal reservoirs.
In the sand fly, the parasite transform into falgellar promastigote
which multiplies by binary fission in the gut of the vector (sandfly)
and migrates to the mouth part to infect a new host.
February 27, 2009
3
Kala Azar
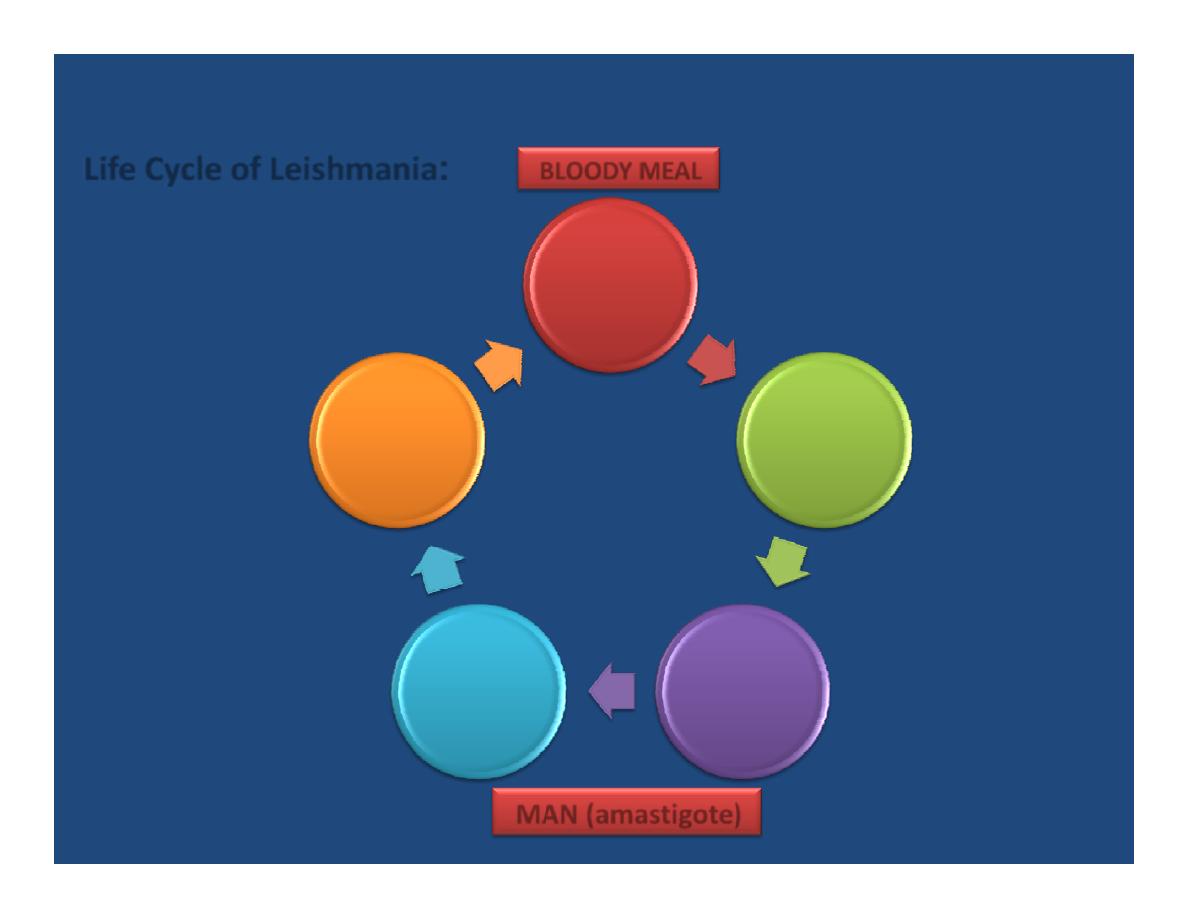
Female
Sandfly
Replication
within the
gut
(Promastig
ote)
Salivary
gland of
sandfly
after 10
days
Mammals
reservoir
(dogs)
Reticuloe
ndothelial
system of
mammals
BLOODY MEAL
MAN (amastigote)
:
Life Cycle of Leishmania
February 27, 2009
4

Geographical Distribution
:
All continents except Australia.
It is most commonly found in India, Sudan, Bangladesh & Brazil.
Other affected regions include Mediterranean, East Africa,
China, Saudi Arabia, Turkey & other countries.
February 27, 2009
5
Kala Azar
Clinical presentation:
The
incubation period
is 2‐6 months.
In child, there is
fever
which is irregular & not associated with
toxemia (the child plays and is not locking ill).
While in infants there is fever, toxemia & the infant locks ill.
Marked splenomegaly
(palpable spleen after 2 weeks of fever), the
spleen is initially soft then it become harder in late stages of the
disease and increase in size (about 1 inch/month).
Severe
cachexia
occurring 6 months after the onset of illness if
untreated.
Hepatomegaly
.
Anemia
.
Bleeding episodes
(when the bone marrow is invaded by the
parasite this will lead to thrombocytopenia).
February 27, 2009
6
Kala Azar
In terminal stages:
Massive hepatosplenomegaly.
Gross wasting.
Pancytopenia.
Lymphadenopathy.
Jaundice (which is usually a dangerous sign).
Edema & ascitis may be found (due to malnutrition or heart
failure caused by anemia).
February 27, 2009
7
Kala Azar
Post Kala‐Azar dermal Leishmaniasis:
Usually occurring after months or even years, but could be seen
during the course of treatment.
We notice hyperpigmented area and nodules in the face (especially
the area around chin and nose) & the trunk. The face often appears
erythematous. It is thought to be caused by treatment and
incomplete eradication of the parasite in the circulation resulting in
its escaping to the tissue and causing this reaction.
February 27, 2009
8
Kala Azar
Diagnosis:
From the
clinical presentation
(fever, hepatosplenomegaly etc).
From the
blood picture
(Pancytopenia & hypergammaglobulinemia)
But
demonstration of the amastigote in tissue specimen
is the
diagnostic method. The specimen (aspirate, biopsy or smear) is
taken from the spleen, bone marrow, lymph node, blood or from
soft tissue and can be cultured in NNN media (Nicole‐Novy‐McNeal).
Another diagnostic method is by
serology
e.g. ELISA, or using a
recombinant K39 agent which is considered a highly sensitive &
specific diagnostic method (approximately 100%). A false ‐ve result
may be due to immune deficient patient (e.g. patient with AIDS).
February 27, 2009
9
Kala Azar
1. Malaria.
2. Tuberculosis.
3. Brucellosis.
4. Typhoid.
5. Amebic liver disease.
6. Lymphoma.
7. Hepatosplenic schistosomiasis.
8. Infectious mononucleosis
Differential diagnosis:
Treatment:
In addition to the supportive measures (that deals with the anemia, infection,
bleeding & malnutrition), specific anti‐leishmaniasis therapy is needed:
1. Pentavalent antimonial compounds:
sodium‐stibogluconate (pentostam ®)
20mg/kg/day for 4 weeks given IM or IV, the cure rate is 80 ‐100%. Side effects:
fatigue, arthralgia, elevated liver enzymes, Hematological manifestations &
cardiac toxicity.
2. Amphotericin B Deoxycholate
: 0.5‐lmg/kg/day for 2‐3 weeks, cure rate is
close to 100%. Side effects: hypotension, fever & nephrotoxicity.
3. Pentamidine isethionte
(Diamidine compounds): effective alternative, less
efficient than Amphotericin B given in 4mg/kg/day for 2weeks IM or IV.
Side effects: hypotension hypoglycemia, cardiac arrhythmia & nephrotoxicity.
February 27, 2009
11
Kala Azar
1.
Avoidance of exposure (insect repellent, insect
sprays & mosquito netting).
2.
Control of infectious reservoir.
3.
Treatment of patients.
Prevention:
February 27, 2009
12
Kala Azar

THANK YOU
powerpoint arranged by: dr. abd el‐ salam dawood
©
2
0
0
9