1
Gynecology
.د
ه
ب
ة
Lec-3-4
Pelvic organ prolapse
Definition
A prolapse is a protrusion of an organ or structure beyond its normal anatomical
confines.
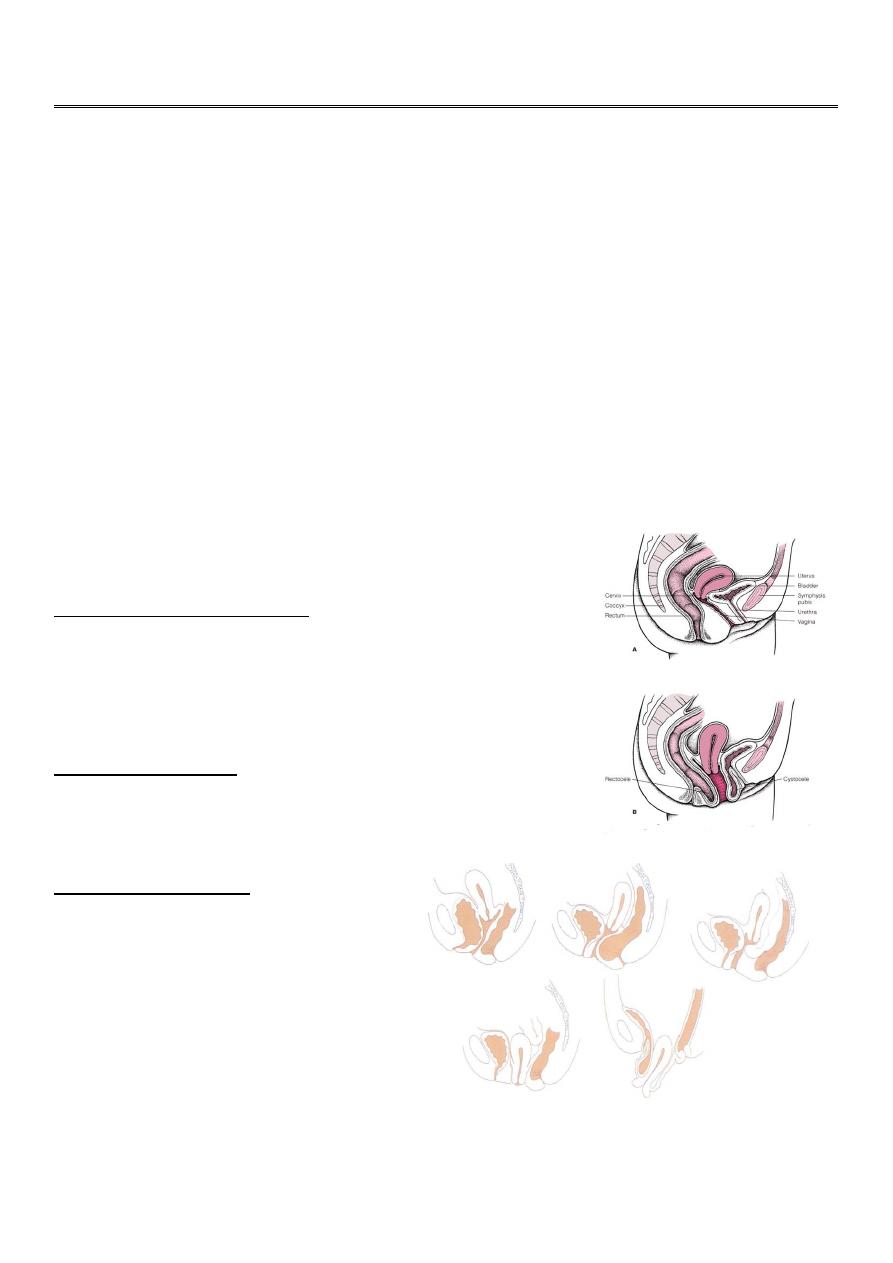
The pelvis is devided into three compartments
• Anterior :contain urethra and bladder
• Middle :contain utrerine or vault descent and enterocele
• Posterior :contain rectum
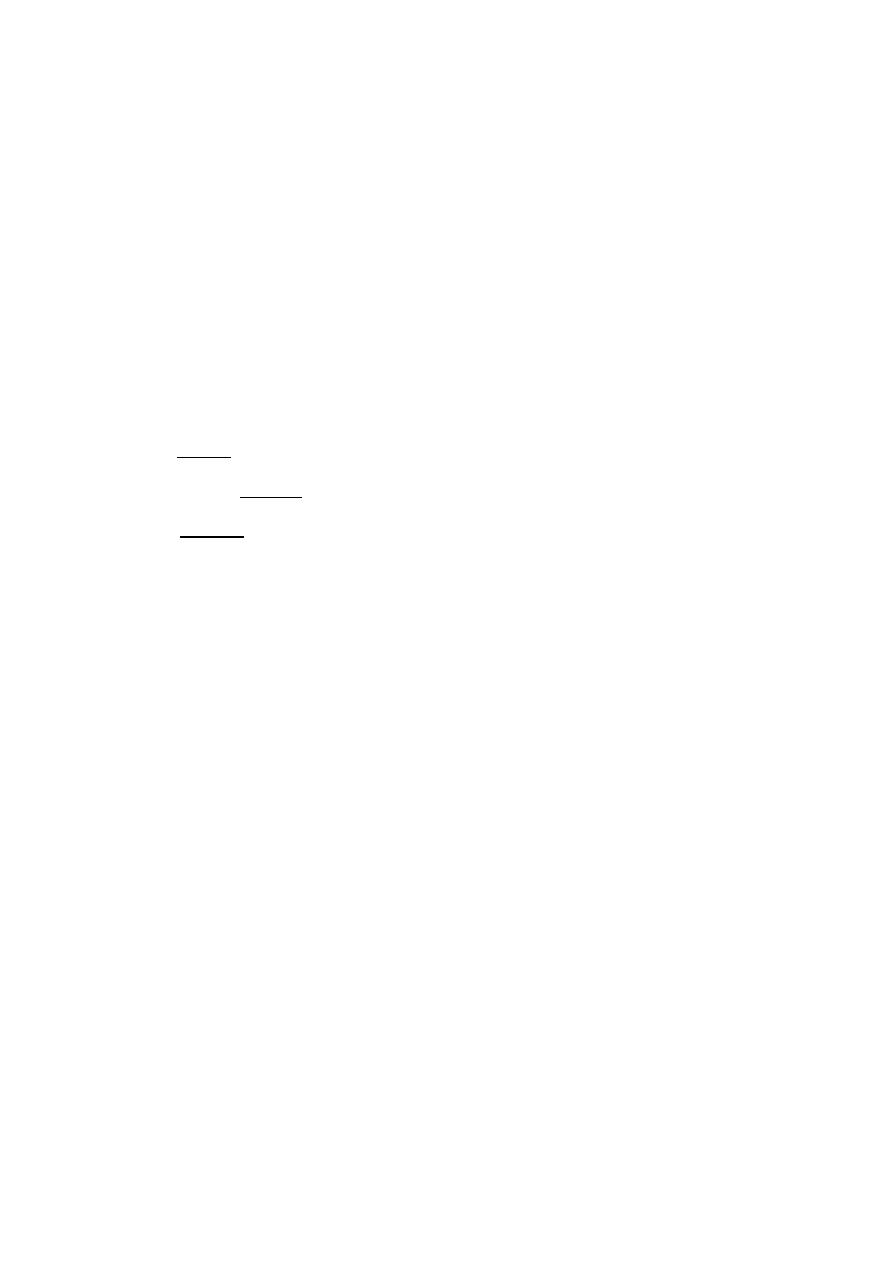
Classification
Anterior vaginal wall prolapse
• Urethrocele: urethral descent
• Cystocele: bladder descent
• Cystourethrocele: descent of bladder and urethra .
Posterior vaginal wall
• Rectocele: rectal descent
• Enterocele: small bowel descent
Apical vaginal prolapse
• Uterovaginal: uterine d
escent with
inversion of vaginal apex occur when the
lateral cervical ligaments become
weakened .
• Vault prolapse: post-hysterectomy
inversion of vaginal apex ,due to
inadequate support by lateral cervical
ligaments
2
Prevalence
Uterovaginal prolapse is extremely common.
prolapse affects 12-30 per cent of multiparous
2 per cent of nulliparous women.
A woman has an 11 per cent lifetime risk of having an operation for prolapse.
Grading
Three degrees of prolapse are described and the lowest or most dependent portion
of the prolapse is assessed whilst the patient is straining (in the uterovaginal
prolapse, the most dependent portion of the prolapse is the cervix)
• 1st: descent within the vagina
• 2nd: descent to the introits
• 3rd: descent outside the introits.
Aetiology
The vital structures for the maintenance of position of the pelvic organs are:
The connective tissue lining the pelvic wall
levator ani
intact nerve of the levator ani
Intact cardinal and uterosacral ligaments
These are influenced by pregnancy childbirth and ageing(acquired ) or congenital
connective tissue defects
1- Congenital factor
Two per cent of symptomatic prolapse occurs in nulliparous women,implying that
there may be a congenital weakness of connective tissue.
2- Racial variation
A decrease in prevalence of prolapse among black women may be due to to better
connective tissue or lumber lordosis that encourage divertion of abdominal forces
towards abdominal wall rather than pelvis

3
3- Childbirth and raised intra - abdominal pressure
The single major factor leading to the development of genital prolapse appears to be
vaginal delivery which lead to pelvic support damage ( nerve ,muscles and connective
tissue ) .
prolapse increases with the increasing parity which was up to seven times more common
in women who had more than seven children compared to those who had one.
Prolapse occurring during pregnancy is rare but is mediated by:
the effects of progesterone and relaxin.
In the increase in intra-abdominal pressure will put an added strain on the pelvic
floor .
a raised intra-abdominal pressure outside of pregnancy ( e.g. chronic cough or
constipation ) is also a risk factor.
4- Ageing
The process of ageing can result in loss of collagen and weakness of fascia and connective
tissue.
These effects are noted particularly during the postmenopause as a consequence of
oestrogen deficiency.
5- Postoperative
Poor attention to vaginal vault support at the time of hysterectomy leads to vault
prolapse .
Mechanical displacement as a result of gynaecological surgery such as
colposuspension may lead to the development of a rectocele or enterocele.
6- Others
Vitamine defeciency
Smoking
steroid therapy
Clinical features
History
@ Women usually present with non-specific symptoms.

4
@Specific symptoms may help to determine the type of prolapse.
@ Risk factors should be looked for .
Symptoms of prolapse depends on the type &site of prolapse
Non - specific :
• Feeling of a lump in the vagina which usually worse towards the end of the day&
relieved by lying down .
• Local discomfort
• Backache
• Bleeding/infection if ulcerated
• Dyspareunia ..
Specific
A-Uterine descent cause low backache,protrusion of cervix and blood stained discharge.
B-Enterocele &vault prolapse may produce vague symptoms of discomfort
C- Rectocele: incomplete bowel emptying, digitation,
D-Cystocele may lead to
1- Discomfort & urinary symptoms:
2- Stress incontinance if there is descent of urethrovesical junction.
3- Voiding difficulty can occur if cystocele is present & bladder neck is normal in
position so the woman has to reduce the mass digitally in order to pass urine .
4- Over flow incontinence with incomplete emptying of bladder
5- Alarge cystocele may lead to increased frequency due to persistant residual urine or
recurrent urinary tract infection because of stasis.
6- Urgency & frequency are found in association with cystocele which may
developed as self induced habit to keep the bladder empty
.
Abdominal examination
Abdominal examination should be performed to exclude organomegaly or
abdominopelvic mass that lead to increase intra abdominal pressure .

5
Vaginal examination
@Prolapse may be obvious when examining the patient in the dorsal position if it protrudes
beyond the introitus; ulceration and/or atrophy may be apparent.
The anterior and posterior vaginal walls and cervical descent should be assessed with the
patient straining in the left lateral position , using Sims' speculum.
@Bi manual pelvic examination should be performed to exclude pelvic mass .
@Combined rectal and vaginal digital examination can be an aid to differentiate rectocele
from enterocele
Differential diagnosis
Congenital or inclusion vaginal dermoid cyst
Urethral diverticulum.
large uterine polyp.
Secondary from the uterine tumor
Investigations
* If urinary symptoms are present, urine microscopy, cystometry and cystoscopy is
considered
* If urination difficulty present and renal failure be suspected , serum urea and
creatinine should be evaluated
* Ultrasound performed to diagnosed abdominopelvic mass
* Pap smear
Prevention
• Shortening the second stage of delivery
• Reducing traumatic delivery may result in fewer women developing a prolapse.
• Women should avoid smoking ,constipation and heavy work.
• The benefits of episiotomy and hormone replacement therapy at the menopause
have not been substantiated.

6
Treatment
The choice of treatment depends on
@ the patient's wishes.
@level of fitness .
Prior to specific treatment
• attempts should be made to correct obesity, chronic cough or constipation.
• If the prolapse is ulcerated, a 7-day course of topical oestrogen should be
administered
• If infection present a course of antibiotics .
Medical (conservative )
# Silicon-rubber-based ring pessaries , they are inserted into the vagina and need
replacement at annual intervals.
# Shelf pessaries are rarely used but may be useful in women who cannot retain a
ring pessary.
Indications for conservative treatment :
• Patient's wish
• As a therapeutic test
• Childbearing not complete
• Medically unfit
• During and after pregnancy (awaiting involution)
• While awaiting surgery.
Complications of conservative treatment:
#vaginal ulceration and bleeding .
# infection.
#Incarceration .
#Fistula formation
7
Surgery :
#Is the main stay in the treatment of prolapse .
#The aim of surgical repair is to restore anatomy and function.
# Approach : the vaginal , abdominal and laparoscopic.
@Anterior colporraphy(cystourethrocele )
Anterior repair (colporrhaphy) is the most commonly performed surgical procedure but
should be avoided if there is concurrent stress incontinence.
An anterior vaginal wall incision is made and the fascial defect allowing the
bladder to herniate through is identified and closed . With the bladder position
restored , any redundant vaginal epithelium is excised and the incision closed.
@Posterior colporraphy (rectocele )
Is common performed procedure. A posterior vaginal wall incision is made and the fascial
defect allowing the rectum to herniate through is identified and close with the rectal
position restored , any redundant vaginal epithelium is excised and the incision closed.
@Enterocele
The surgical principles are similar to those of anterior and posterior repair but the
peritoneal sac containing the small bowel should be excised..
@Uterovaginal prolapse
• Vaginal hysterectomy with adequate support of the vault to the uterosacral
ligaments is sufficient If the woman does not wish to conserve her uterus for
fertility
• If uterine conservation is required , the Manchester operation and
sacrohysteropexy
1-. The Manchester operation involves partial amputation of the cervix .
2- Sacrohysteropexy is an abdominal procedure and involves attachment of a
synthetic mesh from the uterocervical junction to the sacrum.
@Vault prolapse
Sacrocolpopexy is an abdominal procedure in which a mesh is used to attached the
vaginal vault to the sacrum .
Sacrospinous ligament fixation is a vaginal rocedure in which the vault of the vagina is
sutured to one or other sacrospinous ligament

8