BENIGN TUMOURS OF THE OVARY
Benign ovarian cysts are common, frequently asymptomatic and often resolve spontaneously.They are the fourth commonest gynaecological cause of hospital admission.
By the age of 65 years, 4 per cent of all women will have been admitted to hospital for this reason.
Ovarian tumours may be physiological or pathological, and may arise from any tissue in the ovary.
Most benign ovarian tumours are cystic. The finding of solid elements makes malignancy more likely.
However, fibromas, thecomas, dermoids and Brenner tumours usually have solid elements
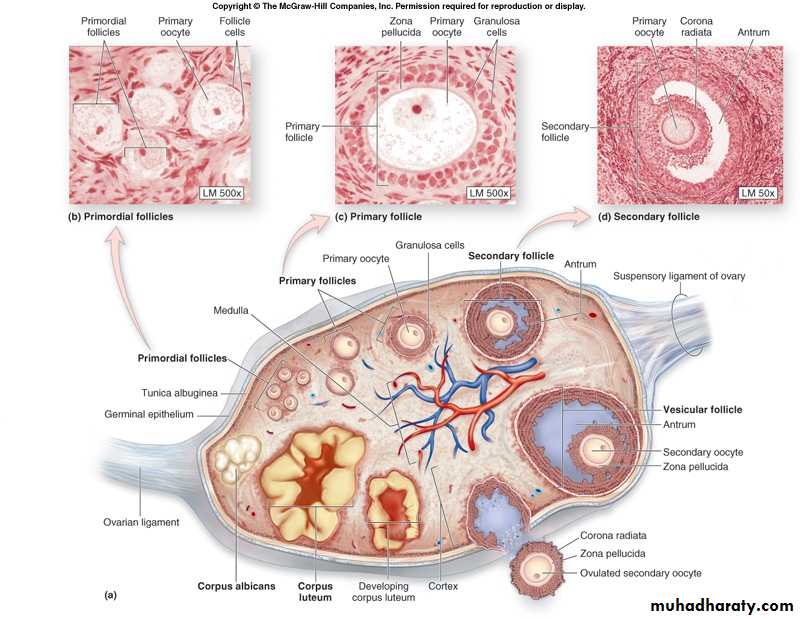
I-Physiological cysts
Physiological cysts are simply large versions of the cystswhich form in the ovary during the normal ovarian
cycle. Most are asymptomatic incidental findings at
pelvic examination or ultrasound scan. Although
they may occur in any premenopausal woman, they
are most common in young women

1-Follicular cyst
Lined by granulosa cells, this is the commonest benign ovarian tumour and is most often found incidentally.It results from the non-rupture of a dominant follicle, or the failure of atresia in a non-dominant follicle
A follicular cyst can persist for several menstrual cycles and may achieve a diameter of up to 10 cm.
Smaller cysts are more likely to resolve, but may require intervention if symptoms develop or if they do not resolve after 8-16 weeks. Occasionally, they may continue to produce
oestrogen, causing menstrual disturbances and
endometrial hyperplasia
2-Luteal cyst
Less common than follicular cysts, these are more likely to present with intraperitoneal bleeding.This is more common on the right side, possibly as a result of increased intraluminal pressure secondary to ovarian vein anatomy
They may also rupture. This usually
happens on days 20-26 of the cycle.Corpora lutea are not called luteal cysts unless they are more than 3 cm
in diameter.
II-Benign germ cell tumours
Germ cell tumours are among the commonest ovarian tumours seen in women less than 30 years of age.
Overall, only 2-3 per cent are malignant, but in
the under-twenties this proportion may rise to a third
1-Dermoid cyst (mature cystic teratoma)
The benign dermoid cyst is the only benign germ cell tumour that is common.It results from differentiation into embryonic tissues.
It accounts for around 40 per cent of all ovarian neoplasms and is most common in young women.
The median age of presentation is 30 years
Dermoid Cyst:
mamillae or
Rokitansky'sprotuberances
It is bilateral in only about 11 per cent of cases. However, if the contralateral ovary is macroscopically normal, the chance of a
concealed second dermoid is very low 0-2 per cent),
particularly if preoperative ultrasound is normal.
A dermoid is usually a unilocular cyst less than
15 cm in diameter, in which ectodermal structures are predominant.
Thus it is often lined with epithelium like the epidermis and contains skin appendages teeth, sebaceous material, hair and nervous tissue.
Endodermal derivatives include thyroid, bronchus
and intestine,
and the mesoderm n ay be represented by bone, cartilage and smooth muscle,
Occasi nally only a single tissue may be present,
in which case the term monodermal teratoma isused.
The classic examples are carcinoid and struma
Ovarii , which contains hormonally active thyroid
tissue.
The term 'struma ovar ii' should be reserved for
tumours composed predominantly of thyroid tissue
and as such comprise only 1.4 per cent of cystic teratomas.
The majority (60 per cent) of dermoid cysts are
asymptomatic.However, 3.5-10 per cent may undergo torsion. Less commonly (1-4 per cent), they may rupture spontaneously, either suddenly, causing an acute abdomen and a chemical peritonitis, or slowly, causing
chronic granulomatous peritonitis
2-Mature solid teratoma
These rare tumours contain mature tissues just like the dermoid cyst, but there are few cystic areas.
They must be differentiated from immature teratomas, which are malignant
Cystic Teratoma

II-Benign epithelial tumours
The majority of ovarian neoplasia, both benign and malignant, arise from the ovarian surface epithelium1-Serous cystadenoma
This is the most common benign epithelial tumourand is bilateral in about 10 per cent.
It is usually a unilocular cyst with papilliferous processes on the inner surface and occasionally on the outer surface.
The epithelium on the inner surface is cuboidal or columnar and may be ciliated
Psammoma bodies are concentric calcified bodies which occur occasionally
in these cysts,but more frequently in their malignant
counterparts.
The cyst fluid is thin and serous.
They are seldom as large as mucinous tumours
Serous Cystadenoma

2-Mucinous cystadenoma
These constitute 15-25 per cent of all ovariantumours and are the second most common epithelial
tumour.
They are typically large, unilateral, multilocular
cysts with a smooth inner surface.
The lining epithelium consists of columnar mucus secreting cells.
The cyst fluid is generally thick and glutinous.
Mucinous Cystadenoma:

Myxoma peritonei
This occurs if the tumour bursts spontaneously or during surgery so the cells seed on the surface of the peritoneum &grow continue secret mucin so abdominal&pelvic cavities slowly filled with mucin&tumor.when this occur it may be a borderline malignant potential.
3-Endometrioid cystadenoma
Benign endometrioid cysts are difficult to differentiate
from ovarian endometriosis
4-Brenner tumours
These account for only 1-2 per cent of all ovarian tumours, and are bilateral in 10-15 per cent of cases.They probably arise from Wolffian metaplasia of the surface epithelium.
The tumour consists of islands of transitional epithelium ( Walthard nests) in a dense fibrotic stroma , giving a largely solid appearance
The vast majority are benign, but borderline or malignant specimens have been reported. Almost three-quarters occur in women over the age of 40 and about half are
inciden tal findings, being recognized only by the
pathologist.
Although some can be large, the majority
are less than 2 cm in diameter.
5-Clear cell (mesonephroid) tumours
These arise from serosal cells showing little differen tiation, and are only rarely benign. The typical histological appearance is of clear or 'hobnail' cells arrangedin mixed patterns
III-Benign sex cord stromal tumours
Sex cord stromal tumours represent only 4 per cent of benign ovarian tumours.They occur at any age, from prepubertal children to elderly, postmenopausal
women.
Many secrete hormones and present with the
results of inappropriate hormone effects.
1-Granulosa cell tumours
These are all malignant tumours but are mentioned
here because they are generally confined to the ovary
when they present and so have a good prognosis.
However, they do grow very slowly and recurrences
are often seen 10-20 years later.
They are largely solid in most cases.
Call-Exner bodies are pathognomonic but are seen in less than half of granulosa cep tumours
Granulosa Cell Tumor:

2-Theca cell tumours
Almost all are benign, solid and unilateral, typically presenting in the sixth decade.Many produce oestrogens in sufficient quantity to have systemic effects such as precocious puberty, postmenopausal bleeding,
endometrial hyperplasia.
3-Fibroma
These unusual tumours are most frequent around50 years of age.
Most are derived from stromal cells and are similar to thecomas.
They are hard, mobile and lobulated with a glistening white surface. Less than 10 per cent are bilateral. While ascites occur with many of the larger fibromas,
Meig's syndrome -
ascites and pleural effusion in association with a
fibroma of the ovary - is seen in only 1 per cent of
cases.
Age distribution of ovarian tumours
In younger women, the most common benign ovarian neoplasm is the germ cell tumour; amongst older women, it is the epithelial cell tumour
The percentage of ovarian neoplasms that are benign also changes with the age of the woman
Presentation
The presentation of benign ovarian tumours is as follows.• Asymptomatic
• Pain
• Abdominall swelling
• Pressure effects
• Menstrual disturbances
• Hormonal effects
• Abnormal cervical smear
Asymptomatic
Many benign ovarian tumours are found incidentally in the course of investigating another un related problem or during a routine examinationAbout 50 per cent of simple cysts less than 6 cm in diameter will resolve spontaneously if observed over a period of 6 months.
A further 25 per cent regress in the following 2 years.
Pain
Acute pain from an ovarian tumour may result fromtorsion, rupture, haemorrhage or infection.
Torsion usually gives rise to a sharp, constant pain caused by ischaemia of the cyst.
Areas may become infarcted.
Haemorrhage into the cyst may cause pain as the capsule is stretched
This happens most frequently with a luteal
cyst.
Chronic lower abdominal pain sometimes
results from the pressure of a benign ovarian tumour,
but is more common if endometriosis or infection is present.
Abdominal swelling
Patients seldom note abdominal swelling until the tumour is very large.A benign mucinous cyst may occasionally fill the entire abdominal cavity.
The bloating of which women complain so often is rarely due to an ovarian tumour
Miscellaneous
*Gastrointestinal or urinary symptoms may resultfrom pressure effects.
*In extreme cases, oedema of the
legs, varicose veins and haemorrhoids may result.
*Sometimes uterine prolapse is the presenting complaint in a woman with an ovarian cyst.
*Occasionally patients complain of menstrual disturbances, but this may be coincidence rather thandue to the tumour.
*Rarely, sex cord stromal tumours
present with oestrogen effects such as precocious
puberty, menorrhagia and glandular hyperplasia,
breast enlargement or postmenopausal bleeding
*Secretion of androgens may cause hirsutism and acne initially, progressing to frank virilism with deepening of the voice or clitoral hypertrophy.
*Very rarely indeed, thyrotoxicosis may result from ectopic secretion of thyroid hormone.
InvestigationsUltrasound
Transabdominal and transvaginal ultrasound candemonstrate the presence of an ovarian mass it cannot distinguish reliably between benign and malignant tumours, solid ovarian masses are more likely to be malignant than their cystic counterparts
The use of colour-flow Doppler may increase the reliability of ultrasound.
Neither computerized tomographicscanning nor magnetic resonance imaging
has significant advantages over ultrasound in this situation, and both are more expensive
Radiological investigations
*Occasionally an abdominal X-raymay show calcification, suggesting the possibility of a benign teratoma.
*An intravenol s urogram is often
performed but is seldom useful.
*A barium enema is
indicated only if the mass is irregular r fixed, or if
there are bowel symptoms.
Blood test and serum markers
It is always sensible to measure the haemoglobin, and
an elevated white cell count would suggest a raised *serum CA 125 is strongly suggestive of ovarian
carcinoma, especially in postmenopausal women.
Women with extensive endometriosis may also have
elevated levels, but the concentration is usually not as
high as is seen with malignant disease.
*The beta-human chorionic gonadotrophin W-hCG) concentration might be measured to exclude an ectopic pregnancy but trophoblastic tumours and some germ cell tumours secrete this marker.infection
*Oestradiol levels maybe elevated in
some women with physiological follicular cysts and sexcord stromal tumours.
*Androgen concentrations may
be increased by Sertoli-Leydig tumours.
*Raised alphafetoprotein
levels suggest a yolk sac tumour
ManagementThe asymptomatic patient
*The older womanWomen over 50 years of age are far more likely to have a malignancy and have little to gain from the conservative management of a pelvic mass more than 5 cm in diameter
laparoscopy may be useful to confirm that the ultra sound lesion is ovarian, but the open approach is still recommended if the ovary is to be removed
*Premenopausal women
Young women aged less than 35 years are both more
likely to wish to have the option of further children
and less likely to have a malignant epithelial tumour.
However, ovarian cysts more than 10 cm in diameter
are unlikely to be physiological or to resolve spontaneously
A clear unilocular cyst of 3-10 cm identified by ultraso und should be re-examined 12 weeks later for evidence of diminution in size
The use of a combined oral contraceptive
is unlikely to accelerate the resolution of afunctional cyst and
hormonal treatment of endometriosis does not usually
benefit an endometrioma.
If the cyst does enlarge,
laparoscopy or laparotomy may be indicated
Criteria for observation of an asymptomatic ovarian tumour
• Unilateral tumour• Unilocular cyst without solid elements
• PremenopalJ sal women - tumour 3-10 cm in diameter
• Postmenopausal women - tumour 2-6 cm in diameter
• Normal CA 125
• No free fluid or masses
The patient with symptoms
The pregnant patient
An ovarian cyst in a pregnant woman may undergo
torsion or may bleed
If an asymptomatic cyst is discovered, it is prudent
to wait until after 14 weeks' gestation before removing it.
This avoids the risk of removing a corpus luteal
cyst upon which the pregnancy might still be dependent
Cysts less than 10 cm in diameter that have a simple appearance on
ultrasound are unlikely to be malignant or to result in a cyst accident, and may therefore be followed ultrasonographically:many will resolve spontaneously
If the cyst is unresolved
6 weeks postpartum, surgery may be undertaken
then.
The prepubertal girl
Ovarian cysts are uncommon and often benign.Teratomata and follicular cysts are the most common.
Theca and granulosa cell tumours may secrete hormones.
Presentation may be with abdominal pain or
distension, or precocious puberty, either isosexual or
heterosexual
Management depends upon
* the relief of symptoms,
* exclusion of malignancy and
*conservation of maximum ovarian tissue without jeopardizing fertility.