Small & Large Intestine
Oct. 11. 2015SMALL/LARGE INTESTINE
NORMAL: Anat., Vasc., Mucosa, Endocr., Immune, Neuromuscular.PATHOLOGY:
CONGENITAL
ENTEROCOLITIS: DIARRHEA, INFECTIOUS, OTHER
MALABSORPTION: INTRALUMINAL, CELL SURFACE, INTRACELL.
(I)IBD: CROHN DISEASE and ULCERATIVE COLITIS
VASCULAR: ISCHEMIC, ANGIODYSPLASIA, HEMORRHAGIC
DIVERTICULOSIS/-IT IS
OBSTRUCTION: MECHANICAL, PARALYTIC (ILEUS) (PSEUDO)
TUMORS: BENIGN, MALIGNANT, EPITHELIAL, STROMAL
SMALL/LARGE INTESTINE ANATOMY
SI = 6 meters,LI = 1.5 meters
Serosa/ adv.
Muscle
Submucosa
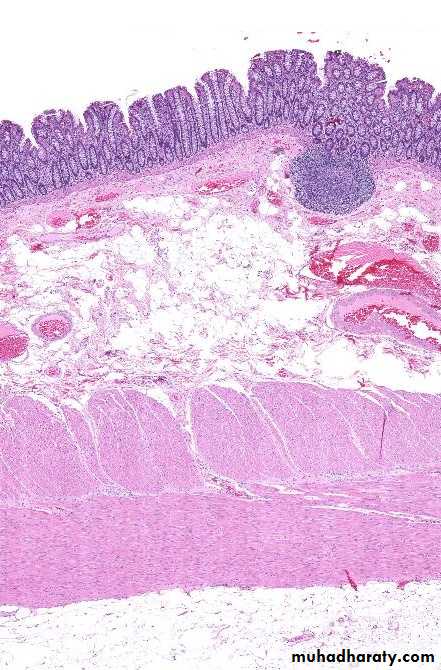
Mucosa
MALT
MUCOSA
Small Intestine
Large IntestineCONGENITAL
DUPLICATIONMALROTATION
OMPHALOCELE
GASTROSCHISIS
ATRESIA/STENOSIS SPECTRUM
MECKEL (terminal ileum, “vitelline” duct)
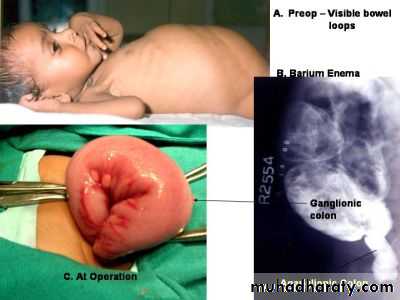
AGANGLIONIC MEGACOLON (HIRSCHSPRUNG DISEASE)
Omphalocele occurs when closure of the abdominal musculature is incomplete and the abdominal viscera herniate into a ventral membranous sac.


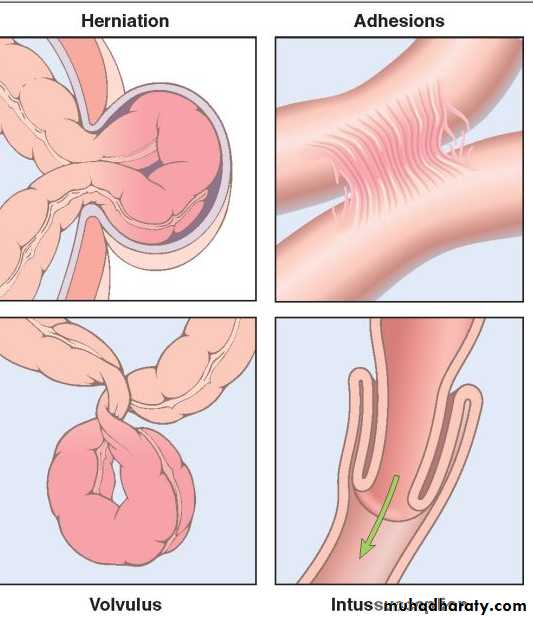
Intestinal Obstruction
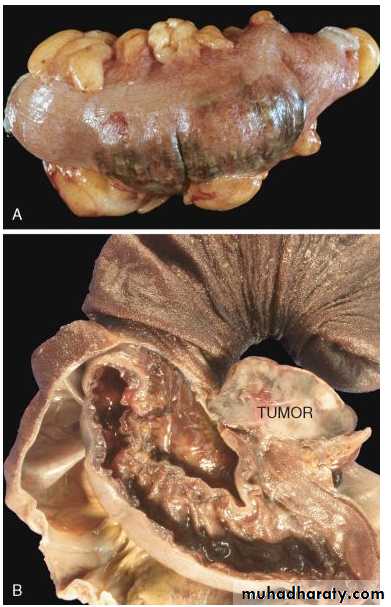
Infarction
Tumor20%
80%
OBSTRUCTION
ILEUS, esp. postsurgicalINFARCTION
MOTILITY DISEASES, esp., HIRSCHSPRUNG DISEASE.
Ileus is a disruption of the normal propulsive GIT motor activity from NON-mechanical mechanisms
Congenital defect in colonic innervation
M>F1/5000
Failure of migration of neural crest cells from cecum to rectum.
Functional Intest obstraction
Rectum and sigmoid
Complications; (Colitis, perfor. Peritonitis).
Hirschsprung diseaseCong. Aganglionic Megacolon
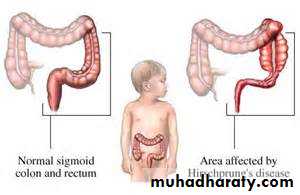
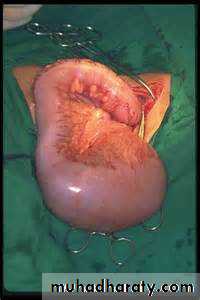
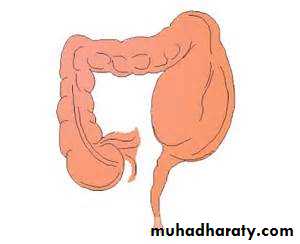

The aganglionic region may have normal or narrow appearance, while the normally innervated proximal colon undergo progressive dilation.
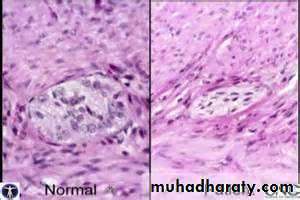
Dx; Distal intestinal segment lacks both the Meissner (submucosal) & Auerbach (myenteric) plexus (“aganglionosis”).
• Hirschsprung diseaseCong. Aganglionic Megacolon
Hirschsprung disease
VASCULAR DISEASES
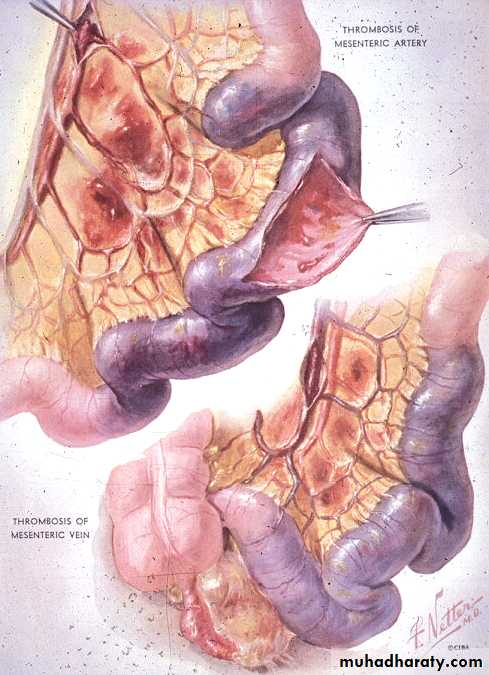
• ISCHEMIA/INFARCTION
HemorrhagicVenous
Arterial
• ANGIO-”DYSPLASIA”*
• HEMORRHOIDS
• Septic shock
• painful
ISCHEMIA/INFARCTION
HEMORRHAGE is the main HALLMARK of ischemic bowel disease
ARTERIAL THROMBUS
ARTERIAL EMBOLISM
VENOUS THROMBUS
CHF, SHOCK
INFILTRATIVE, MECHANICAL
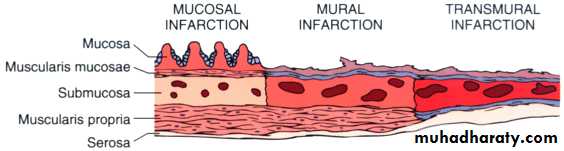
MUCOSAL TRANSMURAL
Ischemic Bowel DiseaseArterial (85%) Vs. venous (15%)
Oclusive or non- oclusive
Acute (severe atherosclerosis, Ar. thrombosis)
chronic hypoperfusion (watershed zones, splenic flexure), (cardiac failure, shock, dehydration, or vasoconstrictive drugs, vasculitis), Low flow.Miscellaneous: RTx, Volvolus, Herniation, truma
Effect:
Severity of vascular involvementAc or ch.
The vessels affected


• Ischemic Bowel Disease
MucosalMural infarction
Mucosal, Mural infarction or Transmural infarction
Intestinal responses to ischemia
in 2 phases
1. Hypoxia
2.Rreperfusion injury



• ISCHEMIA/INFARCTION
Bowel infarction
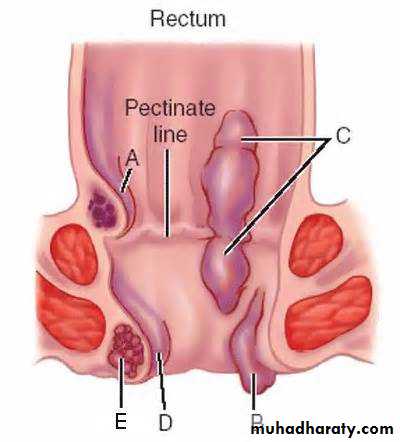
Hemorrhoids
Diletation of anal & perianal col. Ves. That connect portal & syst veins.External Vs. internal hemorrhoids
Complication;C.P.
Rx


Internal Hemorrhoids
External Hemorrhoids• Constipation
• Pregnancy
• Portal hypertension

Diarrheal Dis
DiarrheaSteatorrhea
Dysentery
Cystic Fibrosis
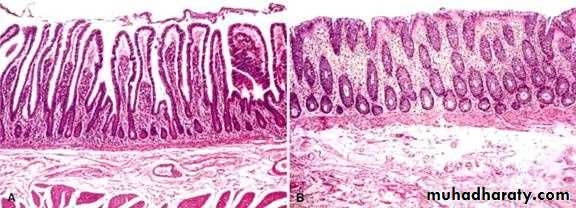
GLUTEN-SENSITIVE ENTEROPATHY
Sensitivity to GLUTEN, protein
in wheat oat, barley, rye
Progressive mucosal “atrophy”,
i.e. villous flattening
Relieved by gluten withdrawal
class II HLA-DQ2 or HLA-DQ8
with other immune diseases.
Both histologic and serologic findings is most specific for diagnosis of celiac disease.
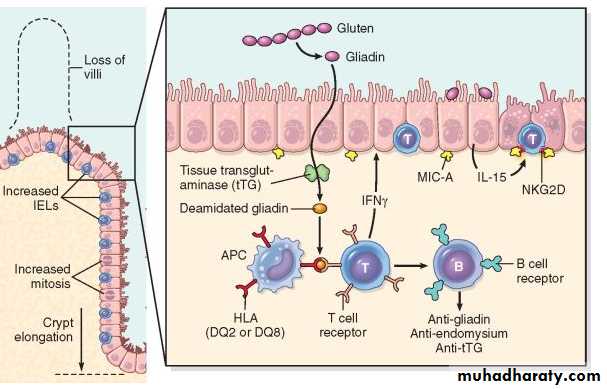
Antigliadin (IgG or IgA) Abs
Endomysial (IgA) AbsAnti -tissue transglutaminase (tTG) Abs.

Ig A Anti endomysial
Ig G if Ig A is deficienttTG more accurate (screening test).
Clinical Features
Adults, celiac disease 30 and 60 Yearsilent celiac disease,
anemia (due to iron deficiency, less, B12 and folate deficiency), diarrhea, bloating, and fatigue.
Pediatric celiac disease, 6 and 24 months
classic symptoms
dermatitis herpetiformis


Dermatitis Herpitiformis (DH)
T cell lymphoma,S Int Ca.
Sq cell ca. esophagus
DIVERTICULOSIS/-ITIS
Pseudo diverticuli; (Colonic diverticuli);– composed of only mucosa on the luminal side and serosa externallyMucosa/submucosa herniates through muscle wall
Assoc. w.:
INCREASED LUMINAL PRESSURE
AGE
LR
FIBER
Weakening of wall
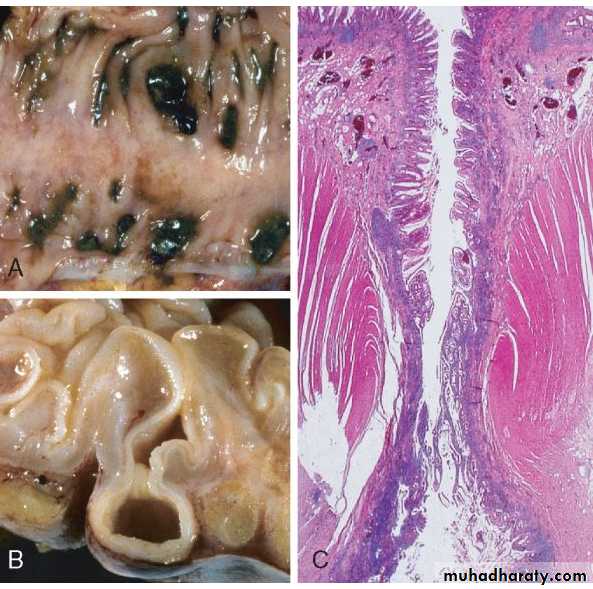
Sigmoid diverticular disease. A, Stool-filled diverticula are regularly arranged. B. the outpouching of mucosa beneath the muscularis propria. C. protrusion of the mucosa and submucosa through the muscularis propria
DIVERTICULOSIS
Sigmoid colon
Asymptomatic unless complicated (infected (“diverticulitis”)), (“appendicitis” syndrome)PERFORATE Peritonitis, local, diffuse
BLEED, silently, even fatally
OBSTRUCT
EXTREMELY EXTREMELY COMMON
NOT assoc w. neoplasm
Diverticulosis
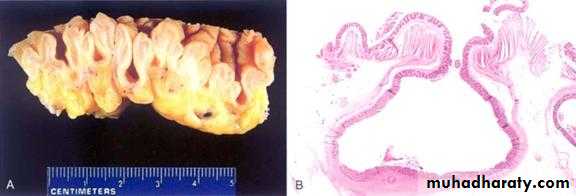
Meckle’s Diverticulum
Congenital diverticulum of the distal small bowel.2 feet from the ileocecal valve.
2 inches in size.
Twice as common in males


Meckel diverticulum,
infant or child, with painless rectal bleeding.ileum, within 2 feet of the ileocecal valve,
present in 2% of normal persons.
results from failure of the vitelline duct to close and is found on the antimesenteric border of the intestine.
Heterotopic gastric or pancreatic tissue may be present in about one-half of cases.
Complications include; perforation, ulceration, intestinal obstruction, intussusception, and neoplasms, including carcinoid tumors.