1
4th stage
جراحة بولية
Lec-8
.د
نعمان
11/10/2015
بسم هللا الرحمن الرحيم
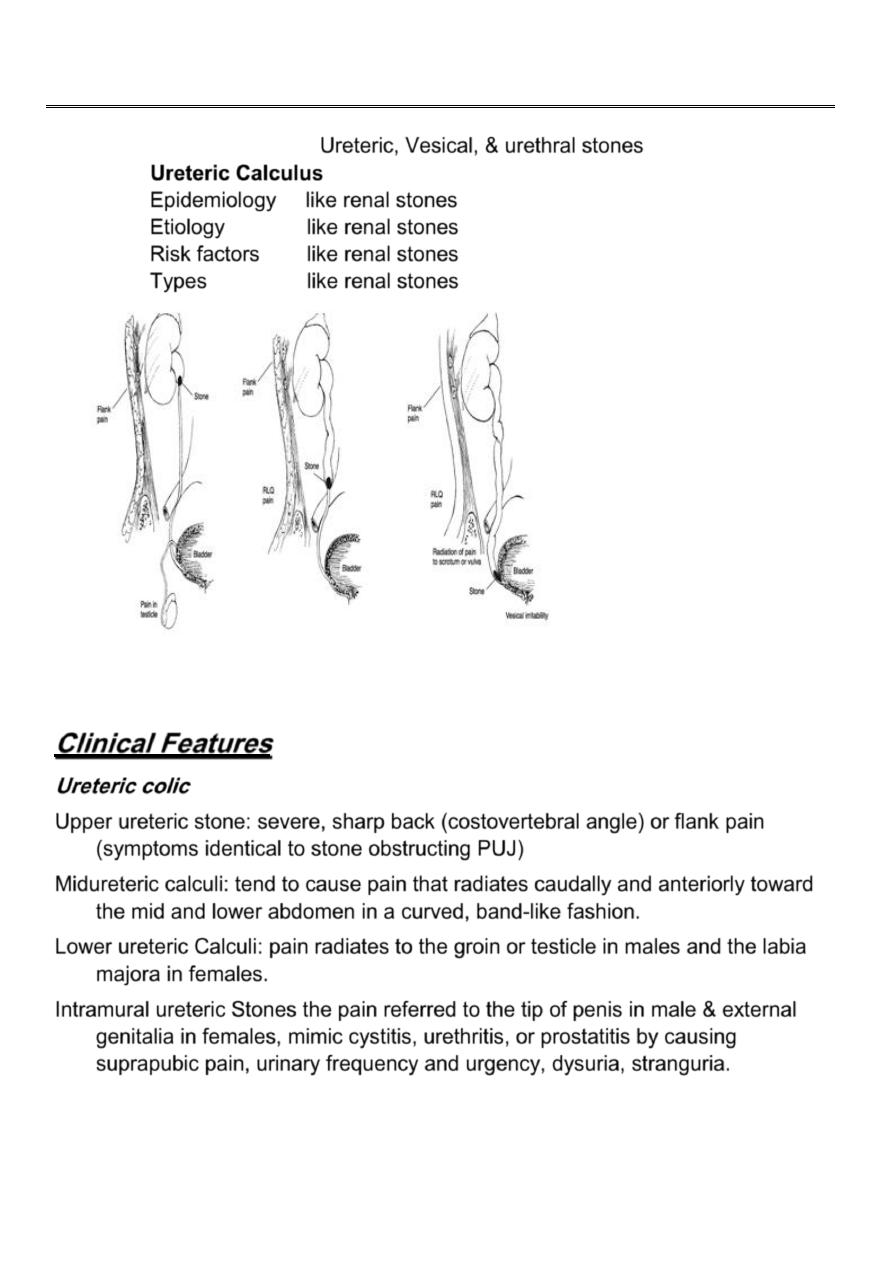
Ureteric, Vesical, & urethral stones
Ureteric Calculus
Epidemiology like renal stones
Etiology like renal stones
Risk factors like renal stones
Types like renal stones
Clinical Features
Ureteric colic
Upper ureteric stone: severe, sharp back (costovertebral angle) or flank pain
(symptoms identical to stone obstructing PUJ)
Midureteric calculi: tend to cause pain that radiates caudally and anteriorly toward
the mid and lower abdomen in a curved, band-like fashion.
Lower ureteric Calculi: pain radiates to the groin or testicle in males and the labia
majora in females.
Intramural ureteric Stones the pain referred to the tip of penis in male & external
genitalia in females, mimic cystitis, urethritis, or prostatitis by causing
suprapubic pain, urinary frequency and urgency, dysuria, stranguria.
2
When the stone becomes impacted the attack of colic give way to a
more consistent dull pain often felt in the iliac fossa.
Distension of the renal pelvis due to obstruction may cause pain &
discomfort in the loin.
Severe renal pain persisting for 1-2 days then subsiding suggest that
ureter is completely obstructed by the stone.
Hematuria
Intermittent gross hematuria or occasional tea-colored urine (old blood).
Most patients will have at least microhematuria.
Rarely (in 10-15% of cases), complete ureteral obstruction presents
without microhematuria.
Almost every attack of colic is associated with microscopic Hematuria.
Profuse bleeding is uncommon & may be associated with passage of
clots.
Fever: when there is associated infection.
(urologic emergency).
Sweating.
Nausea and Vomiting.
Investigations
Laboratory
Investigations:
-
GUE (general urine examination)
-
C&S (urine culture &sensitivity)
-
KFT (kidney function test)
- CBC
(complete blood count)
Radiologic Investigations
U/S (Ultrasound Scanning)
KUB (kidney, ureter, &bladder): 90% of urinary stones are radioopaque.
Excretory Urography (intravenous Urography IVU, intravenous
pyelograpgy IVP)
Retrograde Pyelography
Computed Tomography
(CT scan)
Magnetic Resonance Imaging (MRI)
Nuclear Scintigraphy
3
Treatment
Pain (Renal Colic):
the first line treatment drugs are NSAID as
Diclofenac…. Opiates as pethidine could be used, The value of
smooth muscle relaxant as propantheline is debatable.
Removal of the Stone
Expectant treatment
is appropriate for small stones.
Spontaneous passage depends on stone size, shape, location, and associated
ureteral edema (which is likely to depend on the length of time that a stone has
not progressed). Ureteral calculi 4-5 mm in size have a
40-50% chance of spontaneous passage. In contrast, calculi > 6 mm have a
less than 5% chance of spontaneous passage.
Indications for Surgical Removal of a ureteric calculus
1.
Repeated attacks of pain &the stone is not progressing.
2.
Stone is enlarging with time.
3.
Complete obstruction of the kidney.
4.
Symptoms & signs of infection.
5.
Stone is too large to pass.
6.
Stone is obstructing solitary kidney or there is bilateral obstruction.
7.
Impaired renal function( elevated urea & creatinine).
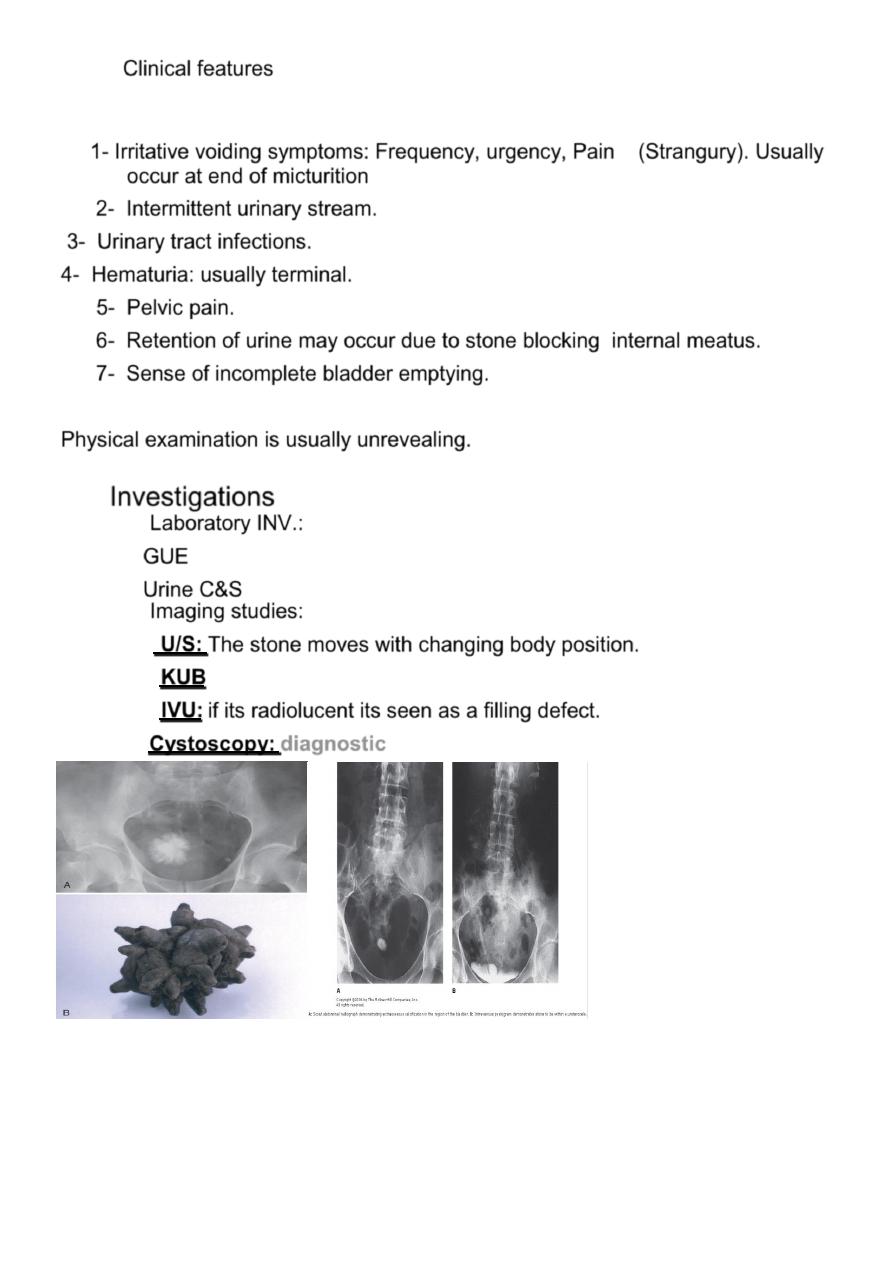
Surgical Removal of a ureteric calculus
Endoscopic
Laparoscopic ureterolithotomy
Open ureterolithotomy
ESWL
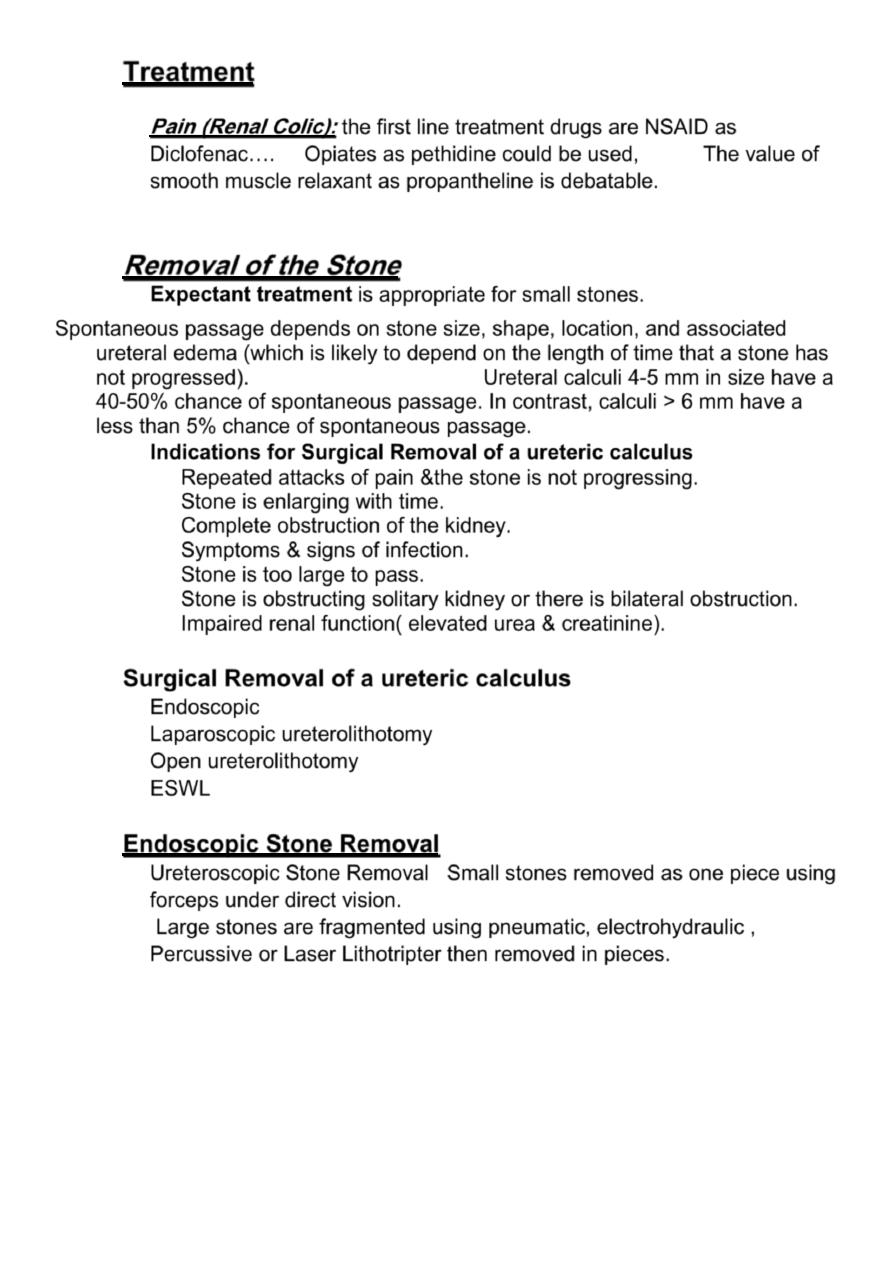
Endoscopic Stone Removal
Ureteroscopic Stone Removal Small stones removed as one piece using
forceps under direct vision.
Large stones are fragmented using pneumatic, electrohydraulic ,
Percussive or Laser Lithotripter then removed in pieces.
4
5
A stone in the middle & upper part of the ureter can be pushed back into the kidney
using ureteric catheter.. put double j stent ..refer to ESWL.
ESWL in situ
6
Bladder Stones
Most bladder calculi are seen in men.
In developing countries, they are frequently found in prepubescent boys.
A solitary bladder stone is the rule, but there are numerous stones in 25%
of patients.
Classification
Primary Bladder stone
: occur in sterile urine , often originate in a kidney
&pass down to the bladder (migratory bladder stone).
Secondary Bladder Stone
: occur in the presence of Infection , bladder out
flow obstruction , Impaired bladder emptying or foreign body as suture
materials, neglected Foleys catheter, forgotten double-J ureteral catheters
can serve as nidi for stones.
Stone analysis
- Ammonium urate
-Uric acid
-Calcium oxalate stones
7
Clinical features
1- Irritative voiding symptoms: Frequency, urgency, Pain (Strangury). Usually
occur at end of micturition
2- Intermittent urinary stream.
3- Urinary tract infections.
4- Hematuria: usually terminal.
5- Pelvic pain.
6- Retention of urine may occur due to stone blocking internal meatus.
7- Sense of incomplete bladder emptying.
Physical examination is usually unrevealing.
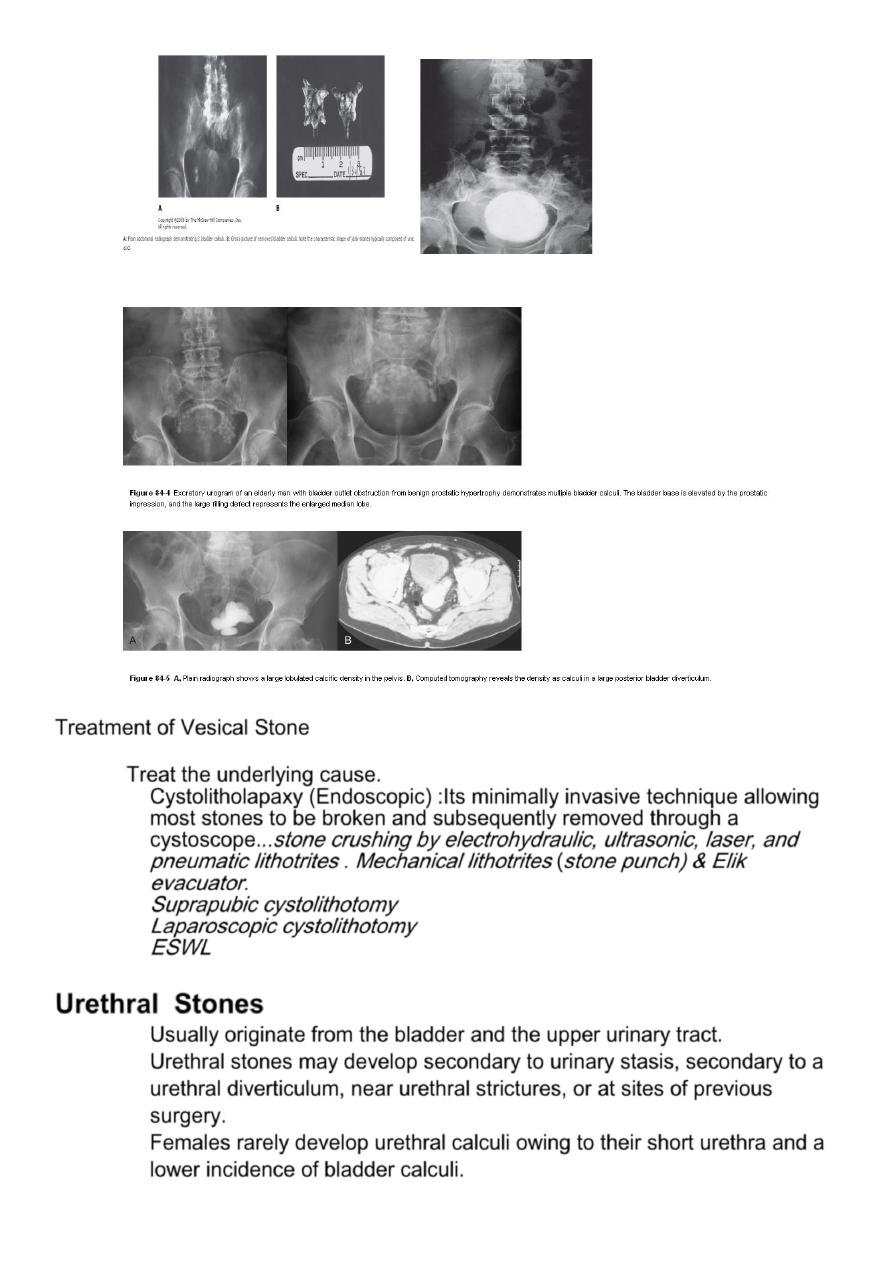
Investigations
Laboratory INV.:
GUE
Urine C&S
Imaging studies:
U/S:
The stone moves with changing body position.
KUB
IVU:
if its radiolucent its seen as a filling defect.
Cystoscopy:
diagnostic
8
Treatment of Vesical Stone
Treat the underlying cause.
Cystolitholapaxy (Endoscopic) :Its minimally invasive technique allowing
most stones to be broken and subsequently removed through a
cystoscope.
..stone crushing by electrohydraulic, ultrasonic, laser, and
pneumatic lithotrites
. Mechanical lithotrites
(
stone punch) & Elik
evacuator.
Suprapubic cystolithotomy
Laparoscopic cystolithotomy
ESWL
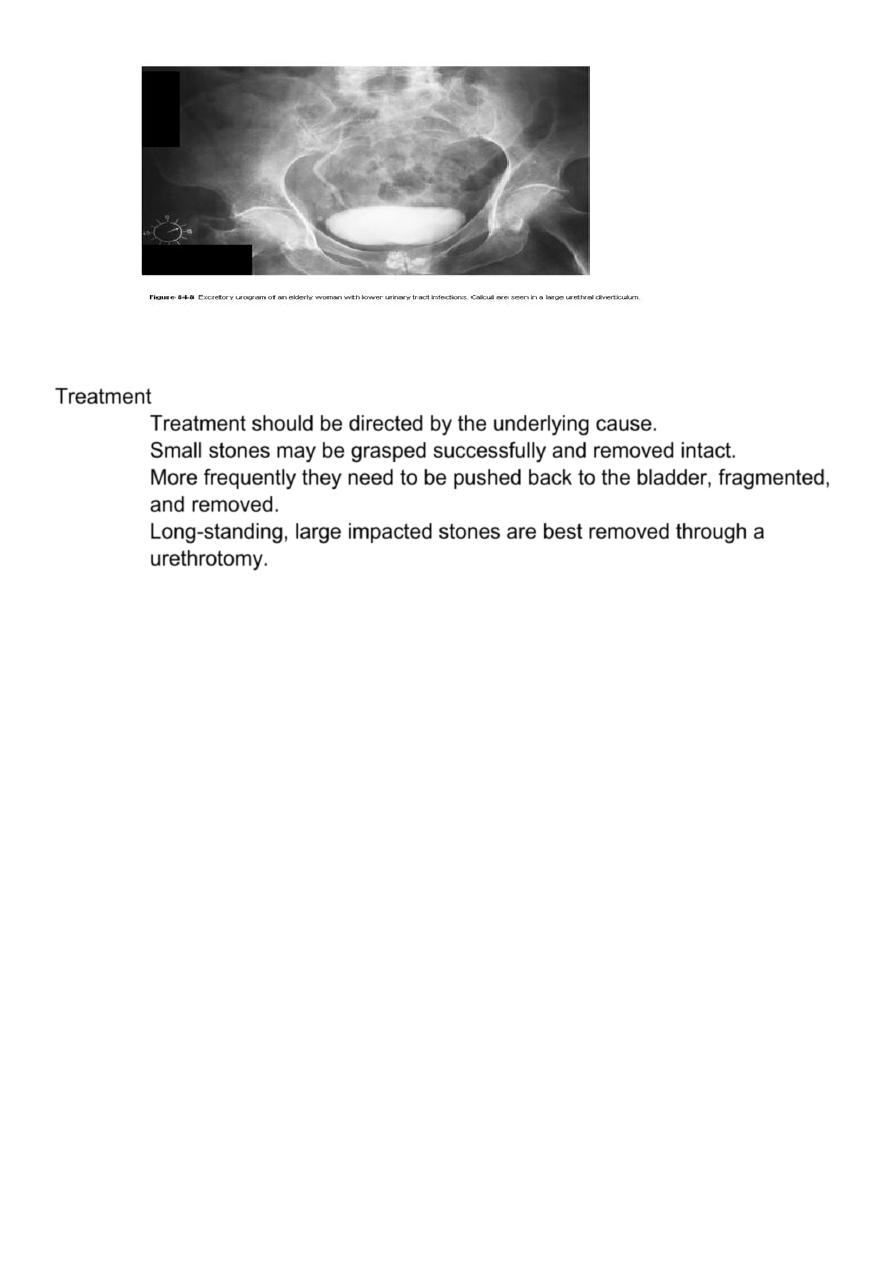
Urethral Stones
Usually originate from the bladder and the upper urinary tract.
Urethral stones may develop secondary to urinary stasis, secondary to a
urethral diverticulum, near urethral strictures, or at sites of previous
surgery.
Females rarely develop urethral calculi owing to their short urethra and a
lower incidence of bladder calculi.

9
Clinical features
Intermittent urinary stream.
Terminal hematuria.
Infection
.
The stones may present with dribbling.
. Acute urinary retention.
On Examination:
The diagnosis may be confirmed by palpating the stone in the urethra.
Investigations
Radiographic study.
pelvic x-ray including the genitalia
Endoscopic visualization
(urethroscopy)
.
11
Treatment
Treatment should be directed by the underlying cause.
Small stones may be grasped successfully and removed intact.
More frequently they need to be pushed back to the bladder, fragmented,
and removed.
Long-standing, large impacted stones are best removed through a
urethrotomy.