
1
4th stage
جراحة بولية
Lec-4
.د
نعمان
5/10/2015
بسم هللا الرحمن الرحيم
Urology
Trauma & Injuries of
Upper Urinary
Tract
Renal Injury
About 10% of all injuries in the emergency room include the genito- urinary system.
Renal injuries are the most common type of urinary system injury.
In 80% of high grade renal injury there is associated abdominal visceral injury.
Mechanism
11.Closed: A diseased kidney ( hydronephrosis, tumor or cyst) are more readily injured with
minimal trauma.
Blunt trauma , Fracture ribs
: 2.Penetrating
Sharp object , stab
Blast shrapnel's
Bullets, High & low velocity missiles
33.
Surgical and Endoscopic causes
.
: caused by blows, falls (FFH), RTAs & stab injuries, fights .
In civil life
: bullet & blast injuries
In wars
Penetrating injuries
Almost always other organ affection
Almost always needs surgical exploration
Absence of hematuria does not rule out renal injury
Vascular injury should not be missed
Blunt injuries
Usually the injury is extraperitoneal, very occasionally (in children) there is peritoneal
injury & escape of urine in to the peritoneal cavity
Clinical features
Pain: Local pain, tenderness
Hematuria is the most important symptom of renal injury. microscopic or
:
gross, early or late.
The degree of hematuria does not reflects the severity of renal injury.
In severe hematuria
may occur.
clot retention
Absence of hematuria does not exclude renal injury
Meteorism : abdominal distensionoccurs
after injury, due to
24 – 48hr
retroperitoneal hematoma implicating splanchnic nerves
The hemodynamic status depends on the extent of the injury & other organ
involvement
2
Signs of renal injuries
Ecchymosis, bruises in the flank, shell inlet and outlet, acute abdomen, palpable loin
masses of hematoma or urinoma.
Intra-peritoneal leak may cause ileus.
Fracture lower ribs and transverse processes are indirect signs of renal injury.
Investigations
GUE, CBC ,Blood Grouping, cross matching, renal function test.
Imaging Studies
: retroperitoneal collection (Hematoma, urinoma).
Ultrasonography
Fracture rib or vertebral transverse process, and soft tissue shadow of blood or
KUB :
urine collection.
IVU :
normal, contrast leak (extravasation), or non-functioning kidney (avulsion), if non
excreting kidney check other kidney function
Arteriography
The preferred imaging study is
If the patient condition is
contrast-enhanced CT-scan
stable
shows the extent of renal parenchymal laceration, urinary extravasation and extent of
retroperitoneal hematoma, (staging).
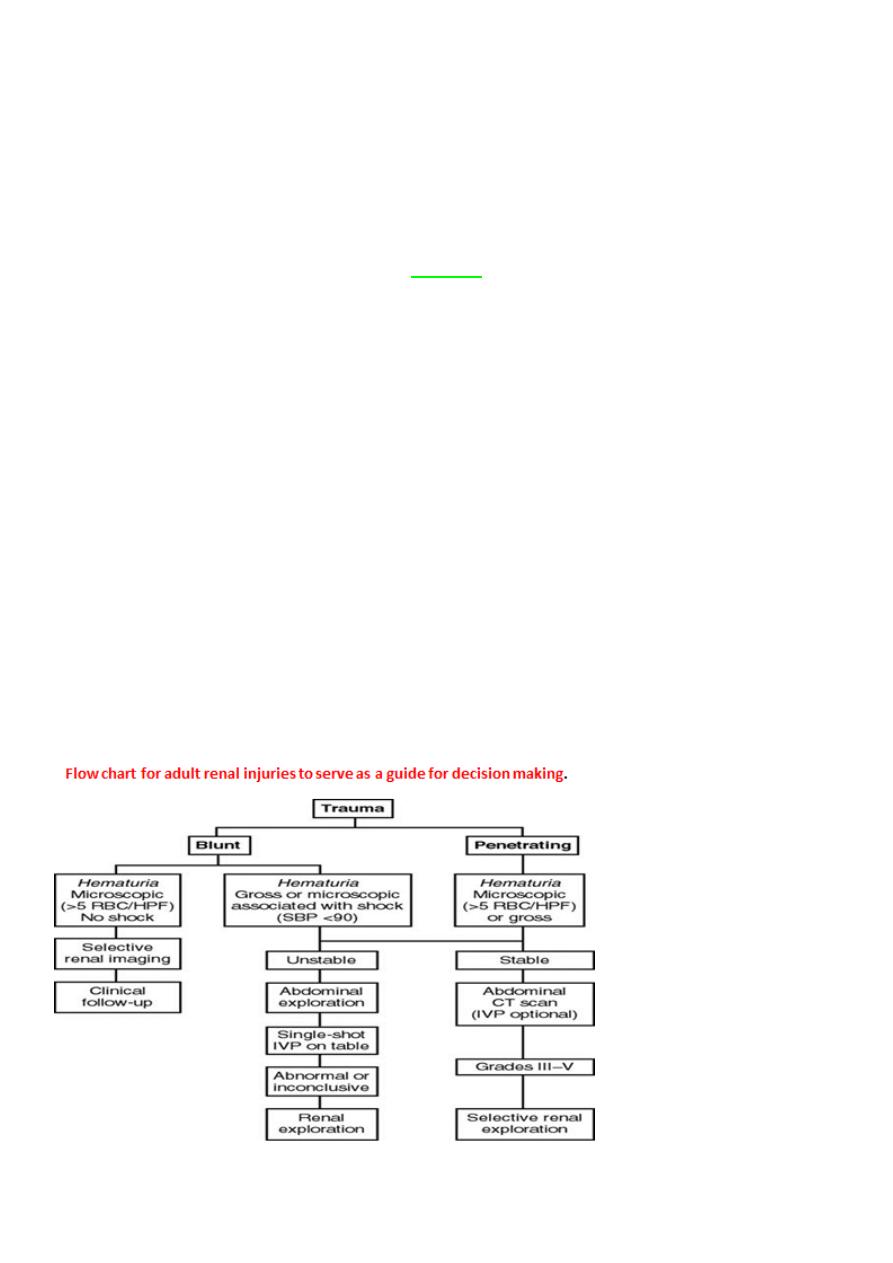
Indications for Renal Imaging
Hematuria is the best indicator of renal injury, and most authors accept
as
5 RBC/HPF
a significant level.
All blunt trauma patients with gross hematuria
Those patients with microscopic hematuria and shock (systolic blood pressure of less than 90
mm Hg any time during evaluation and resuscitation) should undergo renal imaging, usually
CT-scan with intravenous contrast.
Penetrating injuries with any degree of hematuria should be imaged
3
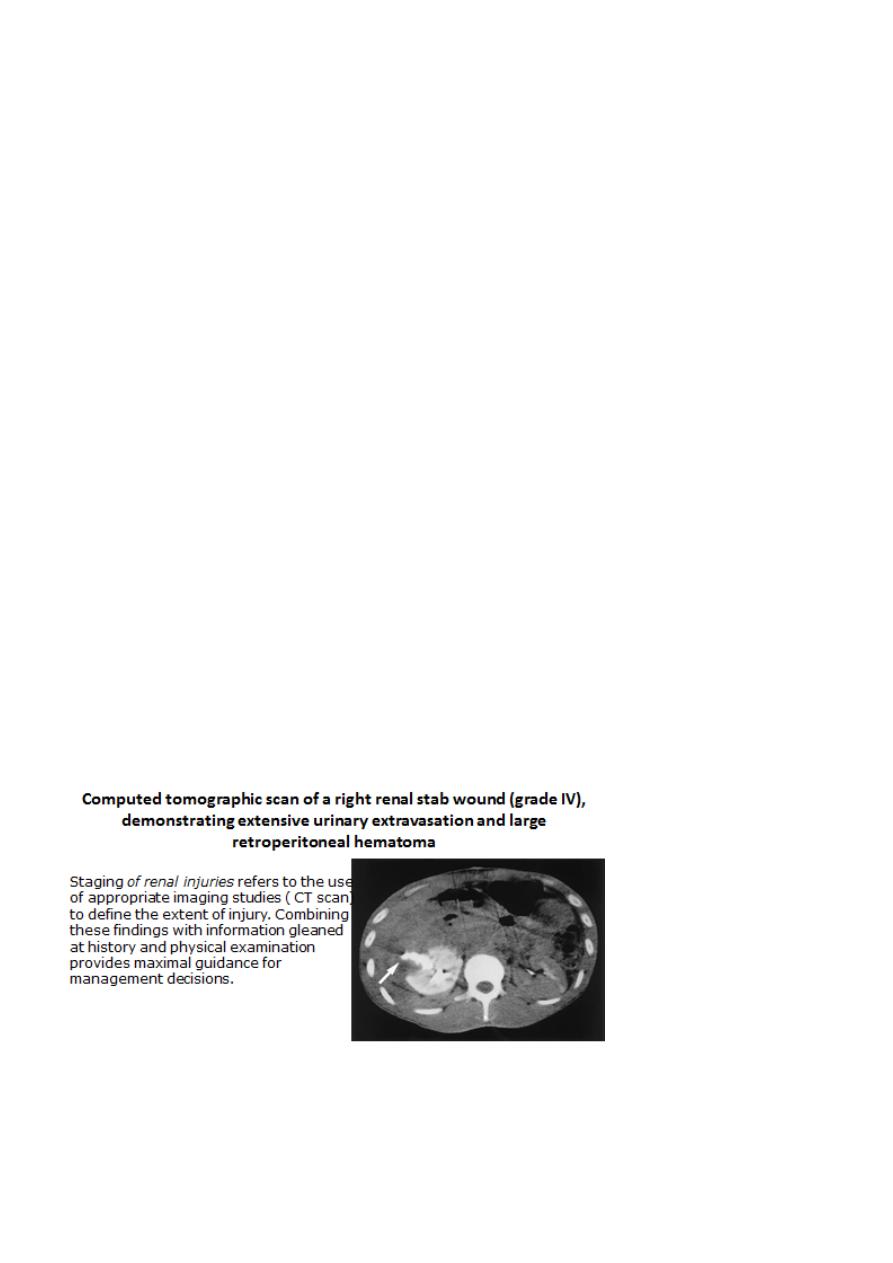
Computed tomographic scan of a right renal stab wound (grade IV), demonstrating
extensive urinary extravasation and large retroperitoneal hematoma
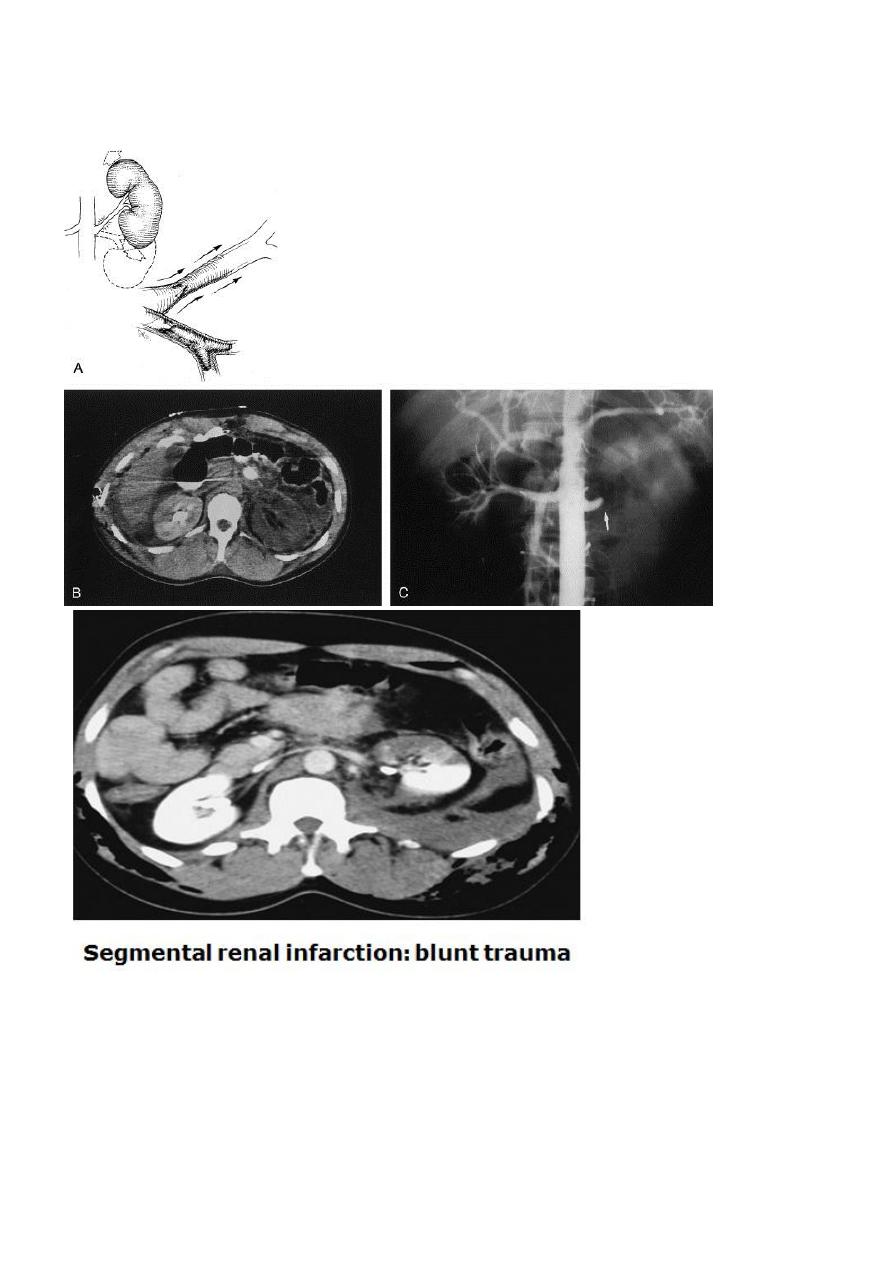
Movement of the kidney from blunt trauma (deceleration injury) causes stretch on the renal
artery, resulting in rupture of the arterial intima and formation of a thrombus
.

4
5
6
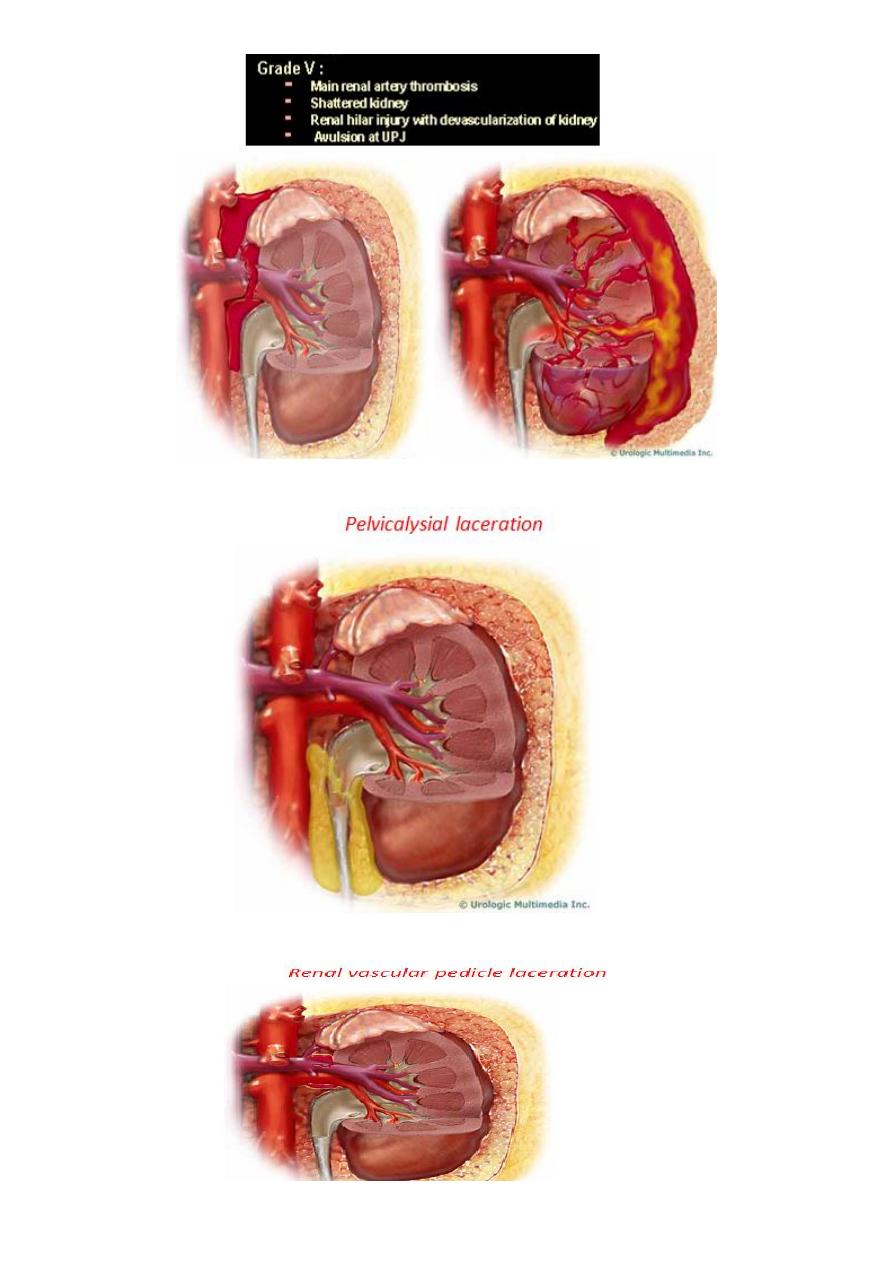
7
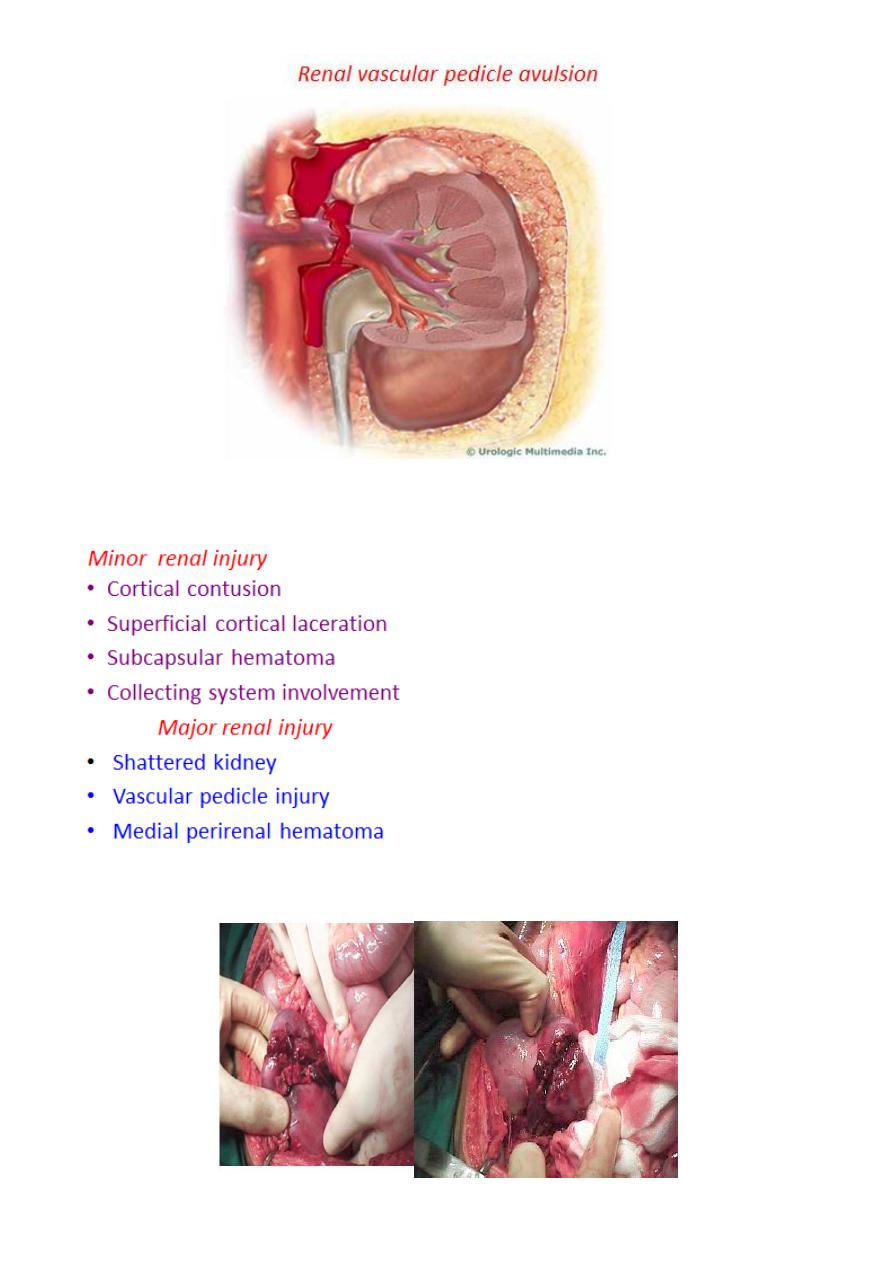
8
9
Management
The minor grades =
of the cases = conservative treatment
85%
of renal injuries can be managed non operatively
98%
!
need surgical intervention
0-15%
The
needs urgent surgical care.
renal vascular injuries
more often require
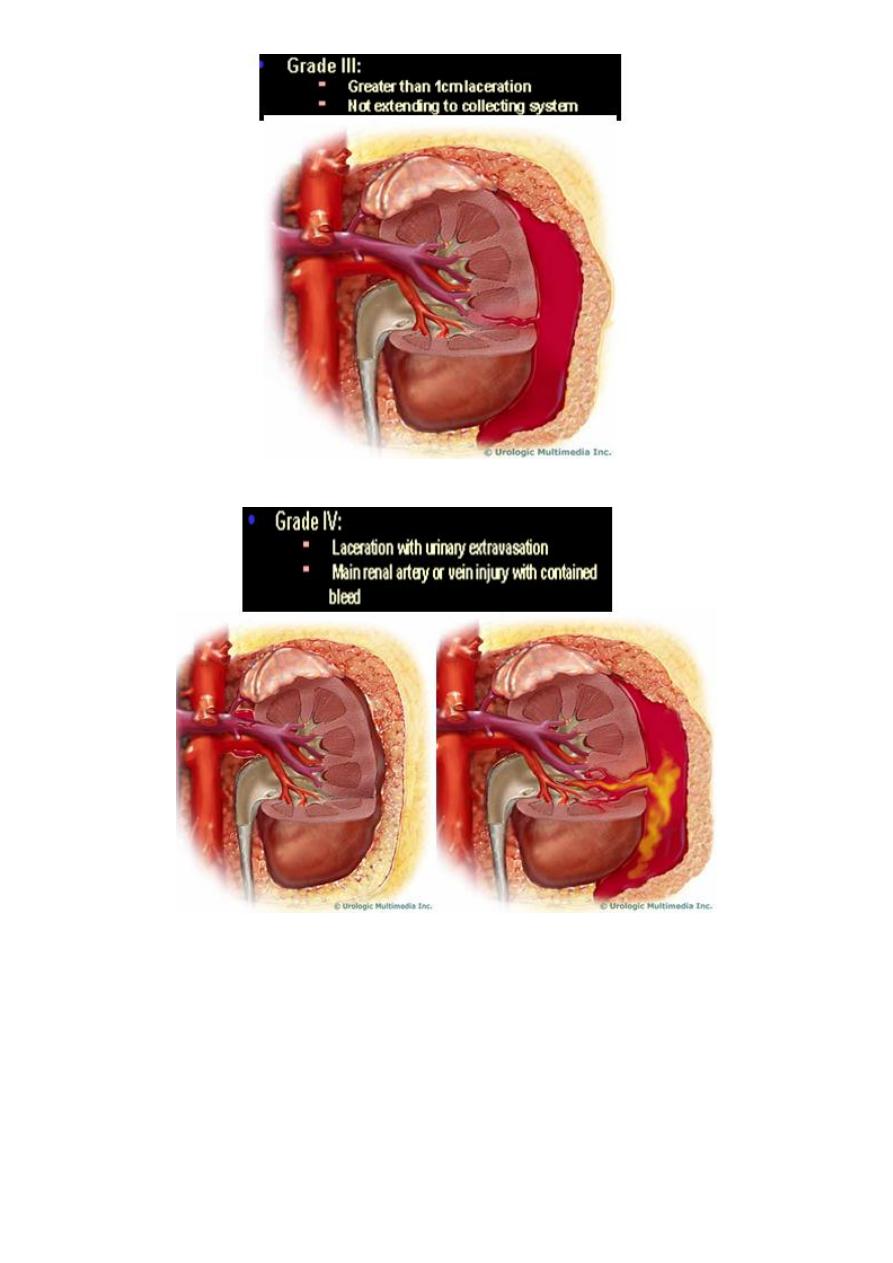
Grade IV and V injuries
surgical exploration
Management
ABCDE
A:
Airway & cervical spine protection
.
B:
Breathing.
C:
Circulation & control of external bleeding.
D:
Disability or neurological status.
E:
Exposure (undress) & environment (temperature control)
Conservative care
Hospital admission & complete Bed rest : Once the gross hematuria clears ambulation is
allowed, should gross hematuria recur, bed rest is reinstated. Ambulation without any sequel
allows hospital discharge with close clinical follow-up.
Correct & maintain the hemodynamic status, Repeated clinical assessment (Continuous vital
signs check ).
Conservative care ( Cont.)
Analgesia
IV fluid hydration & blood replacement (Blood group & cross matching).
Antibiotics to prevent secondary infection of the hematoma or urinoma.
Watch the urine for the depth of hematuria. ( Save last urine sample to compare it with
previous sample regarding hematuria).
11
Indications for Exploration
Absolute indications
- progressive blood loss
- expanding perinephric hematoma
- pulsatile perirenal hematoma
- perirenal infection
- Hemodynamically is not recoverable
- The renal vessels are injured
- other organ involvement cannot be excluded.
Relative indications
-urinary extravasation
-nonviable tissue -
delayed diagnosis of arterial injury
-segmental arterial injury
-incomplete staging.
A radiologist may be able to stop the haemorrhage by embolisation if a bleeding vessel can
be identified.
The possibility of damage to other abdominal organs is checked during a
transperitoneal approach.
Release of the tamponading effect of the perirenal haematoma can result in massive
haemorrhage and the surgeon must be fully prepared for this.
When the kidney is irretrievably ruptured or avulsed from its pedicle, nephrectomy is
the only course
11
complications
Early complications :
1-Bleeding. Hematuria or retroperitoneal bleeding. (resolve in >85%).
2-Urine extravasation resulting in urinoma.
3-Infection (Urinoma or infected hematoma) resulting in perinephric abscess formation.
4- Loss in renal function.
5- Clot retention

12
Late complications
1- Hypertension after 3 months, due to renal scarring.
2- Hydronephrosis.
3- Arteriovenous fistula
4- Delayed renal bleeding can occur several weeks after injury, but it usually occurs within
21 days
5- Aneurysm of the renal artery
6- Calculus formation, repeated UTI