PATHOLOGY- BLOCK II
NEOPLASIA- ONCOLOGY
DR. MOHANAD ALJANABI MD/PHD
BLOCK OUTLINE
Lectures of Dr. Mohanad Aljanabi / Oncology
Oncology/ Dr. Mohanad Aljanabi/ 2021
•
Definitions
•
Nomenclature
•
Types of neoplesia
•
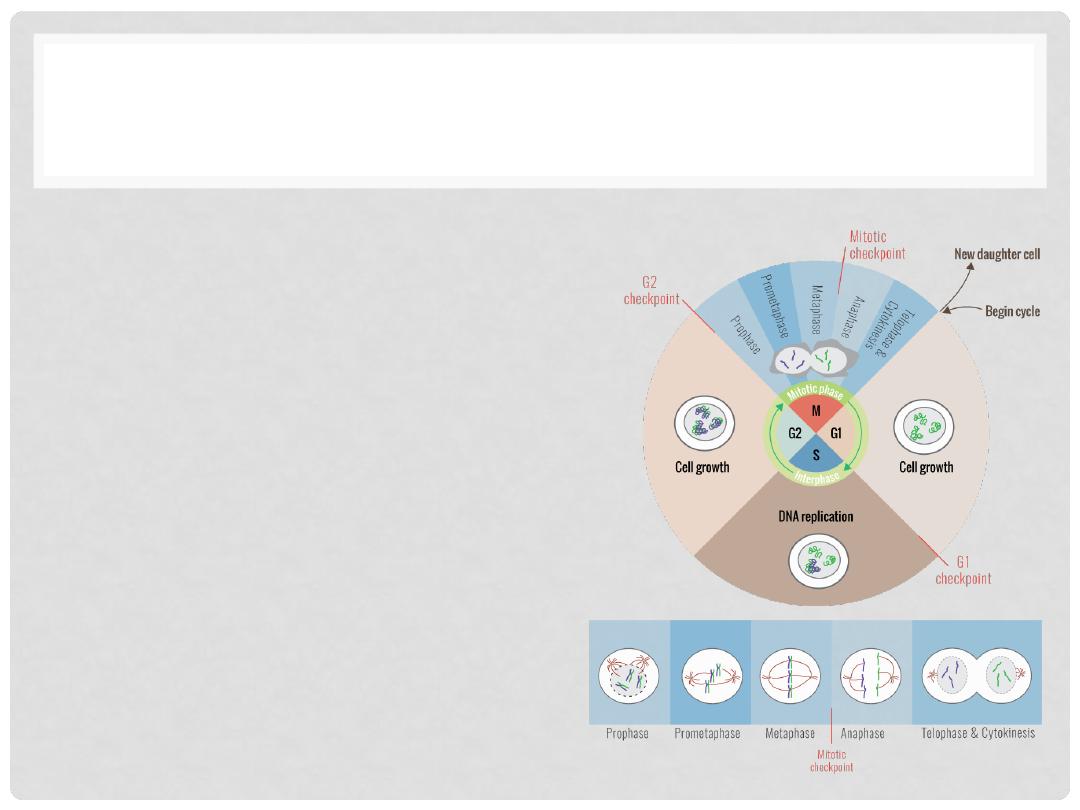
How do Tumor grow?!
•
Epidemiology
•
Molecular Basis of Cancer and Carcinogenesis
•
Cause of cancer
•
Immune defense against cancer
•
Clinical Features of cancer
•
Cancer diagnosis and treatment
WHAT IS A “NEOPLASM”?
•
Lay term of “tumor” conveys usual connotations
– i.e. a
new growth or mass
•
Definition revolves around these features:
•
Monoclonal proliferation
of cells with specific mutations
•
Excessive
and
unregulated growth
of these cells, often at
the expense of surrounding normal tissue
Lectures of Dr. Mohanad Aljanabi / Oncology
TUMOR OR CANCER
•
Tumor
- synonymous with neoplasma
•
Cancer
- common term for malignant neplasma
•
Neoplasma have parenchyma and stroma
•
Benign and malignant tumors have their own
nomenclature
Lectures of Dr. Mohanad Aljanabi / Oncology
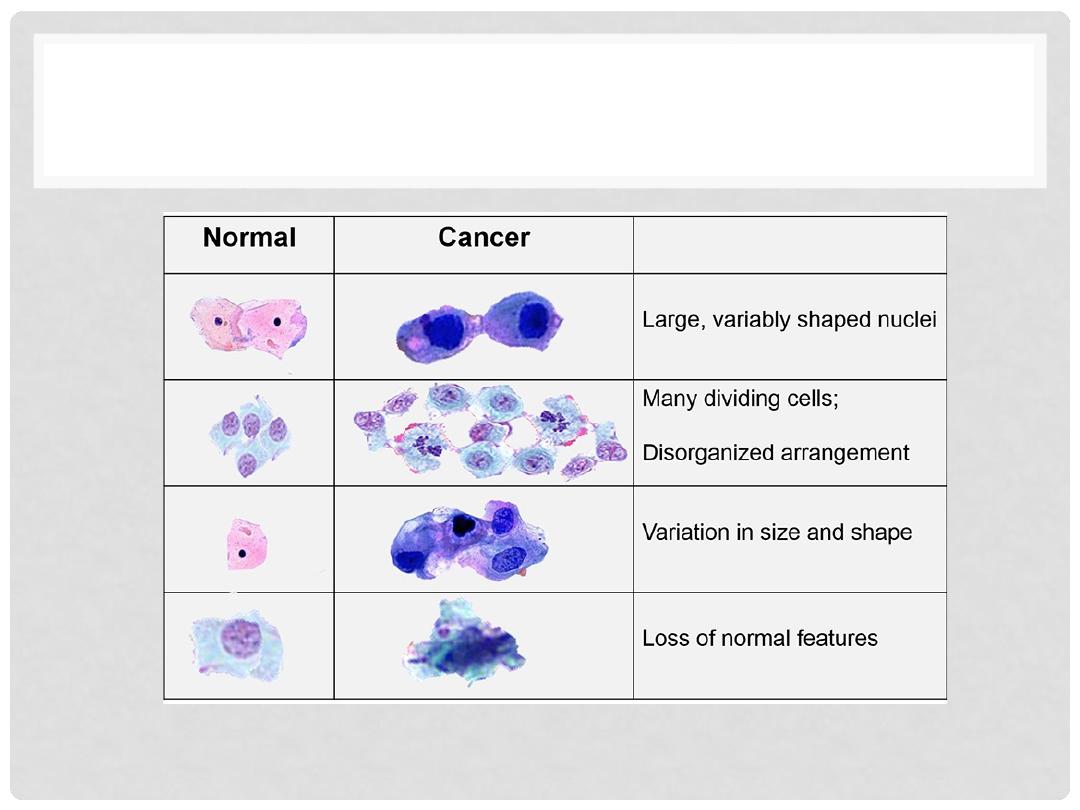
NORMAL VS CANCER CELLS
Lectures of Dr. Mohanad Aljanabi / Oncology
PRECURSORS OF NEOPLASIA
•
Hyperplasia
•
Metaplasia
•
Dysplasia
•
Chronic inflammations
Lectures of Dr. Mohanad Aljanabi / Oncology
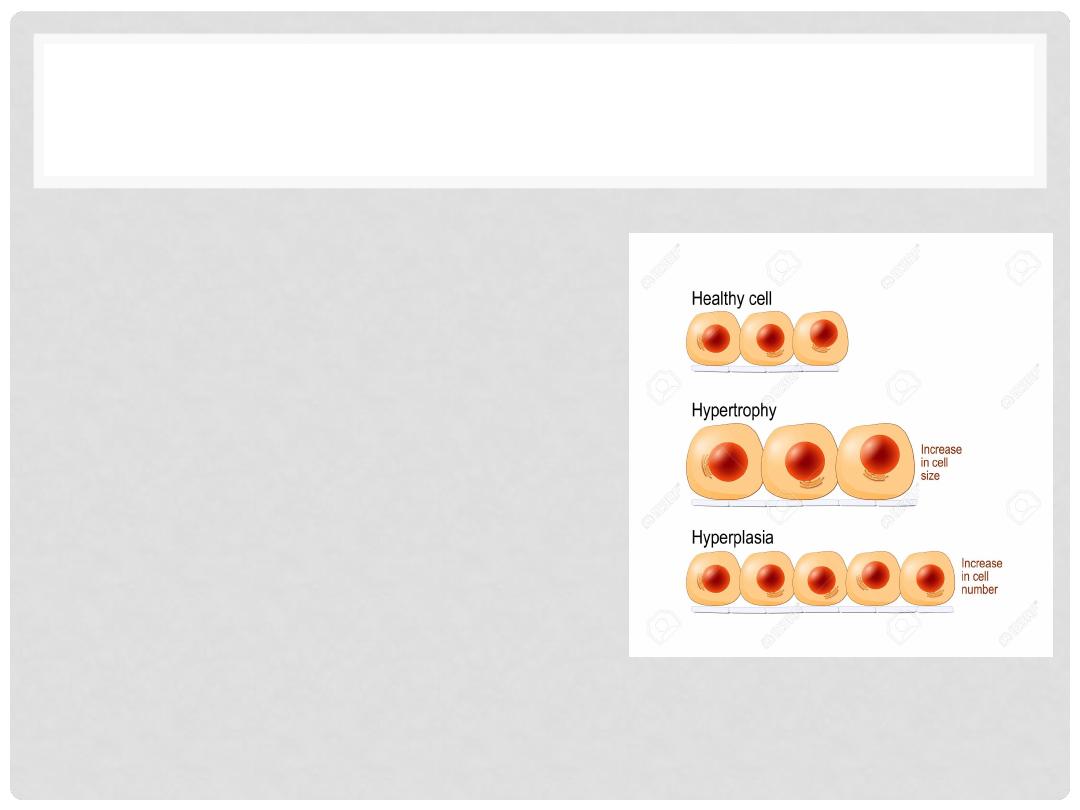
HYPERPLASIA
•
Increase in number of cells
•
Regulated by cell signaling
and growth factors
•
Can be normal or abnormal
•
Some hyperplasia can lead to
tumor
Lectures of Dr. Mohanad Aljanabi / Oncology
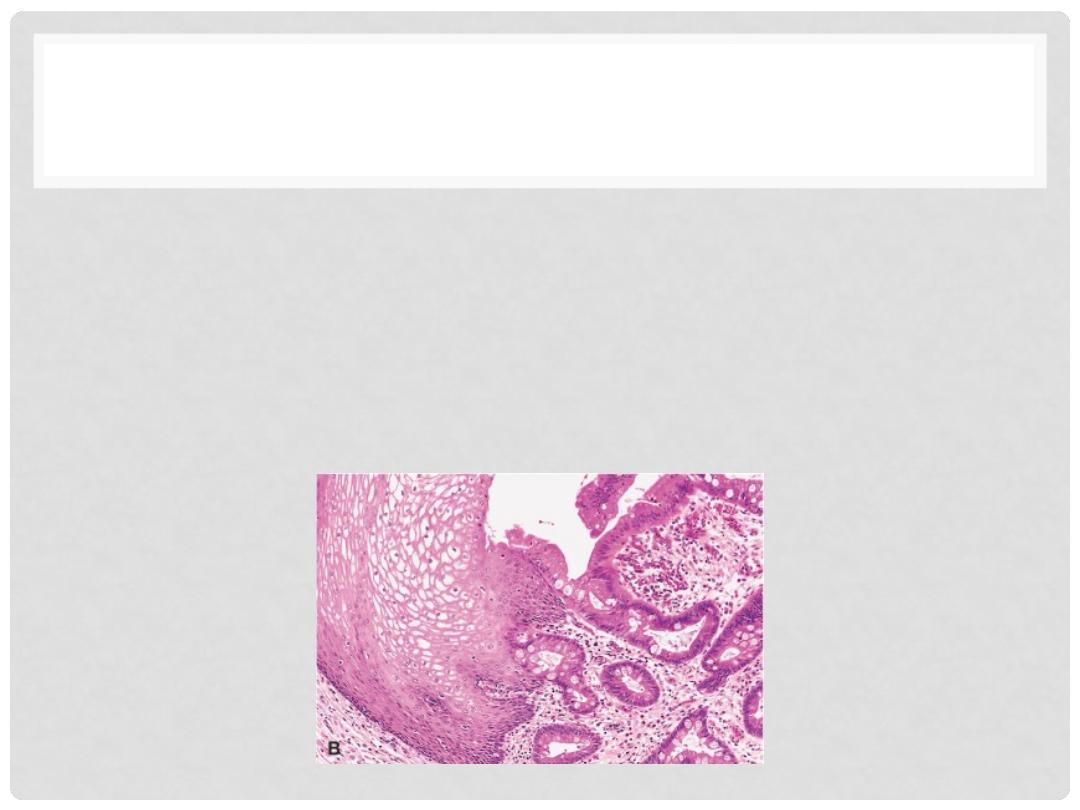
METAPLASIA
An
adaptive change
in differentiation, reversible, no mutations
necessary.
•
Eg- change of esophageal mucosa from squamous to gastric type
in the setting of acid reflux (heartburn). Better able to withstand the
corrosive effects of the acid
•
Metaplasia is fertile ground for development of
“
dysplasia”(disordered growth)
Lectures of Dr. Mohanad Aljanabi / Oncology
ANAPLASIA (PRE CANCER)
•
Pleomorphism
•
Size
•
Shape
•
Abnormal nuclear morphology
•
Hyperchromasia
•
High nuclear cytoplasmic ratio
•
Chromatin clumping
•
Prominent or even multiple nucleoli
•
Mitoses
•
Mitotic rate
•
Location of mitoses
•
Loss of “polarity”
Lectures of Dr. Mohanad Aljanabi / Oncology
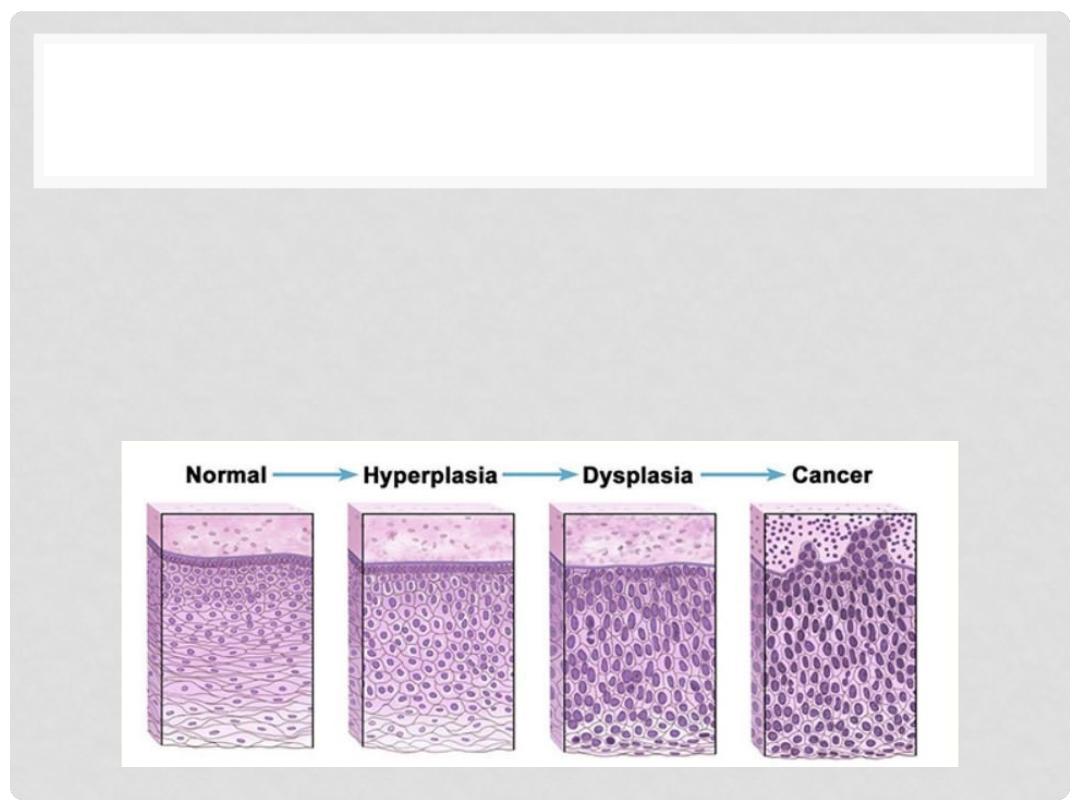
DYSPLASIA (ABNORMAL GROWTH)
•
Malignant transformation is a multistep process, the visual
appearances may parallel the genetic mutations
•
In dysplasia
some but not all
of the features of malignancy
are present, microscopically
•
Dysplasia
may
develop into malignancy (Uterine cervix
&Colon polyps)
•
Graded as low-grade or high-grade, often prompting
different clinical decisions
•
Dysplasia may
NOT
develop into malignancy
Lectures of Dr. Mohanad Aljanabi / Oncology
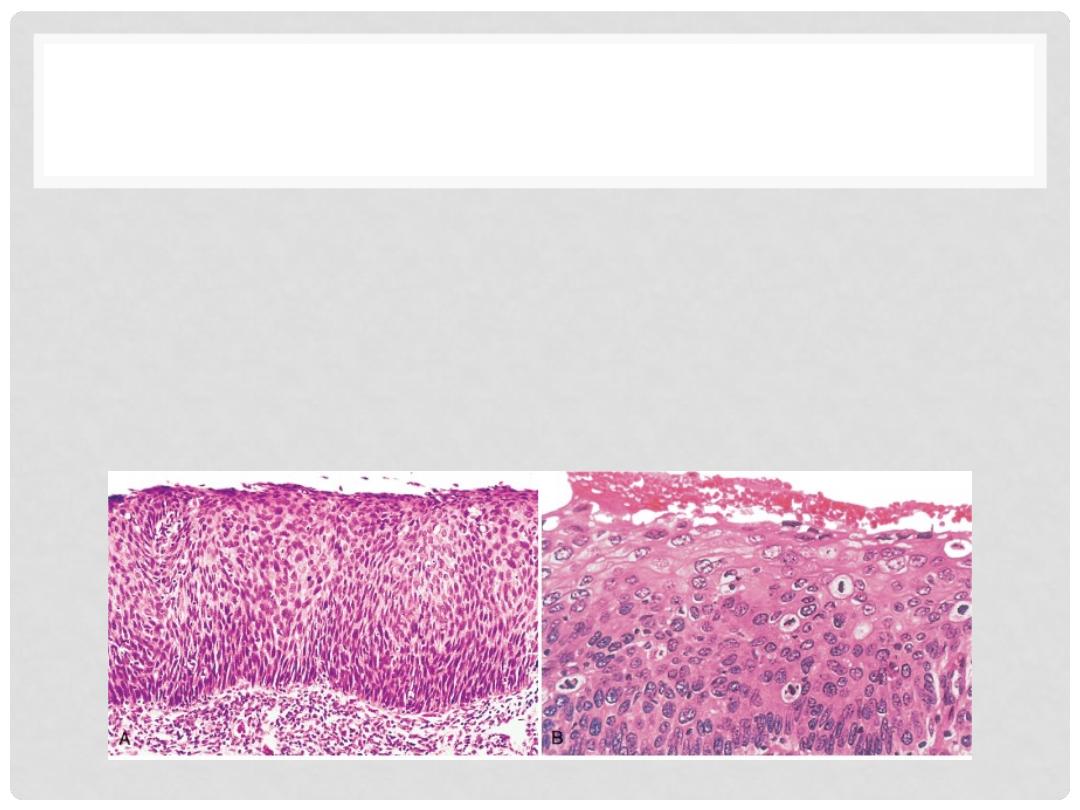
DYSPLASIA
•
Dysplasia
refers to recognizable morphologic changes in cells
that indicate the presence of genetic mutations beginning the
development of a neoplasm
•
Often graded, e.g. PAP smears for uterine cervical cancer are
low and high grade
Lectures of Dr. Mohanad Aljanabi / Oncology
NEOPLASIA
•
It means “
new growth
”. Referred as tumor/cancer
•
Uncontrolled proliferation of cells
•
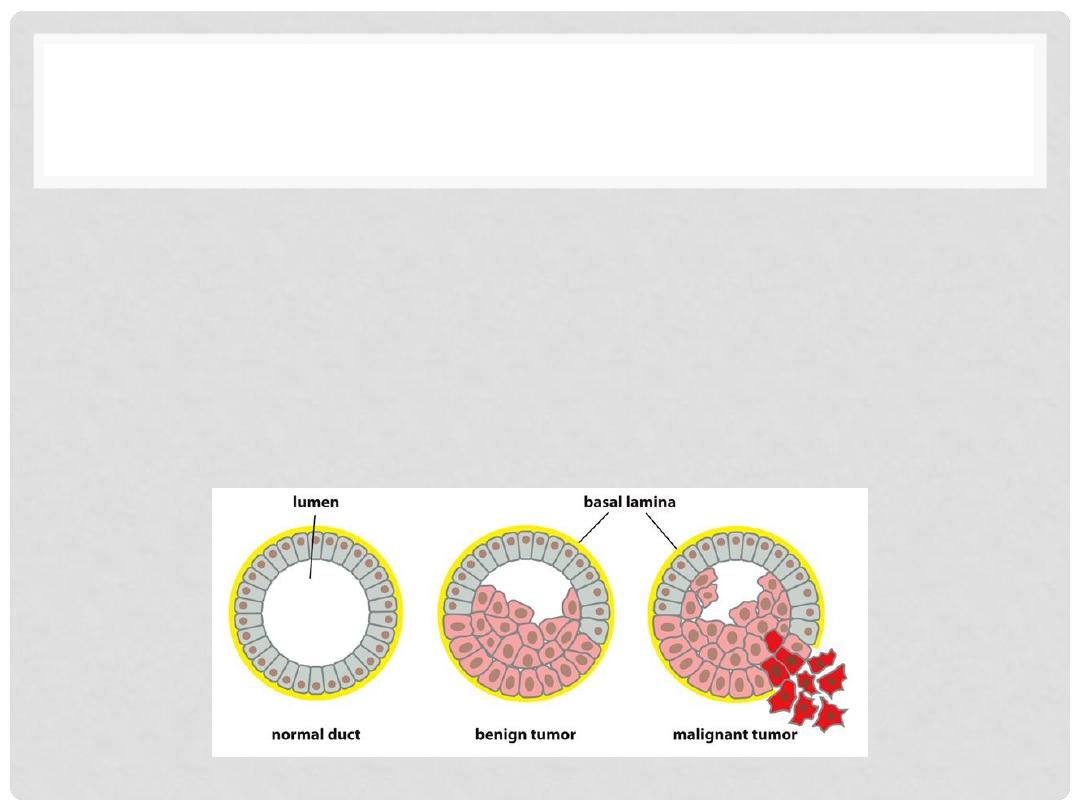
Can be normal “benign” or abnormal “malignant”
•
Benign
: Cells grow as a compact of cells the remain at their
site of origin
•
Malignant
: growth of cells is uncontrolled and can spread
into surrounding tissue and distant sites
Lectures of Dr. Mohanad Aljanabi / Oncology
BENIGN VS MALIGNANT
•
Benign
–tumors incapable of metastasis and having a good
clinical outcome (prognosis)
•
Malignant
– tumors capable of invasive growth and/or
metastasis, often fatal if not treated effectively
•
Metastasis
- spread of a malignant tumor from one site to
another via blood or lymph
Lectures of Dr. Mohanad Aljanabi / Oncology
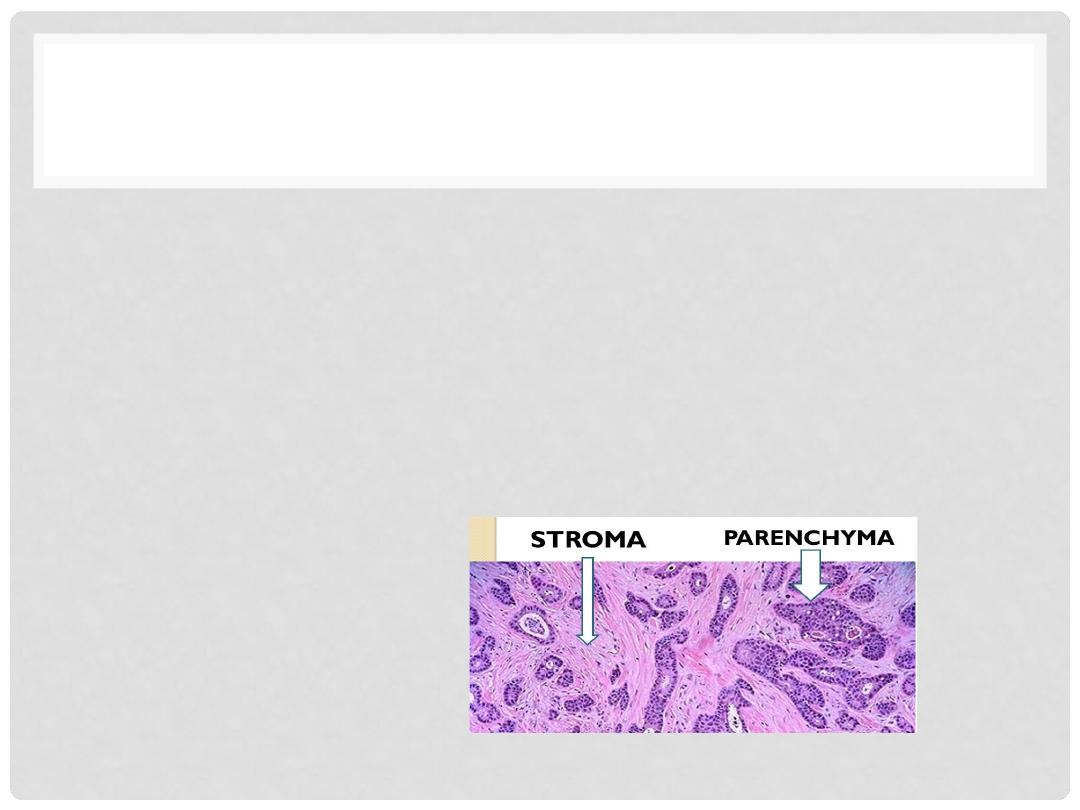
PARENCHYMA AND STROMA
•
Parenchyma
– these are the tumor cells themselves,
usually referring to epithelial cells in organs.
•
Stroma
– connective tissue cells that support the
parenchymal cells – not actually tumor cells, but are
stimulated to grow by the tumor via growth factors,
e.g. angiogenesis
Lectures of Dr. Mohanad Aljanabi / Oncology
CHARACTERISTICS OF MALIGNANT
TUMORS!
•
Cellular features
•
Local invasion
•
Capsule
•
Basement membrane
•
Metastasis
•
Unequivocal sign of malignancy
•
Seeding of body cavities
•
Lymphatic
•
Hematogenous
Lectures of Dr. Mohanad Aljanabi / Oncology
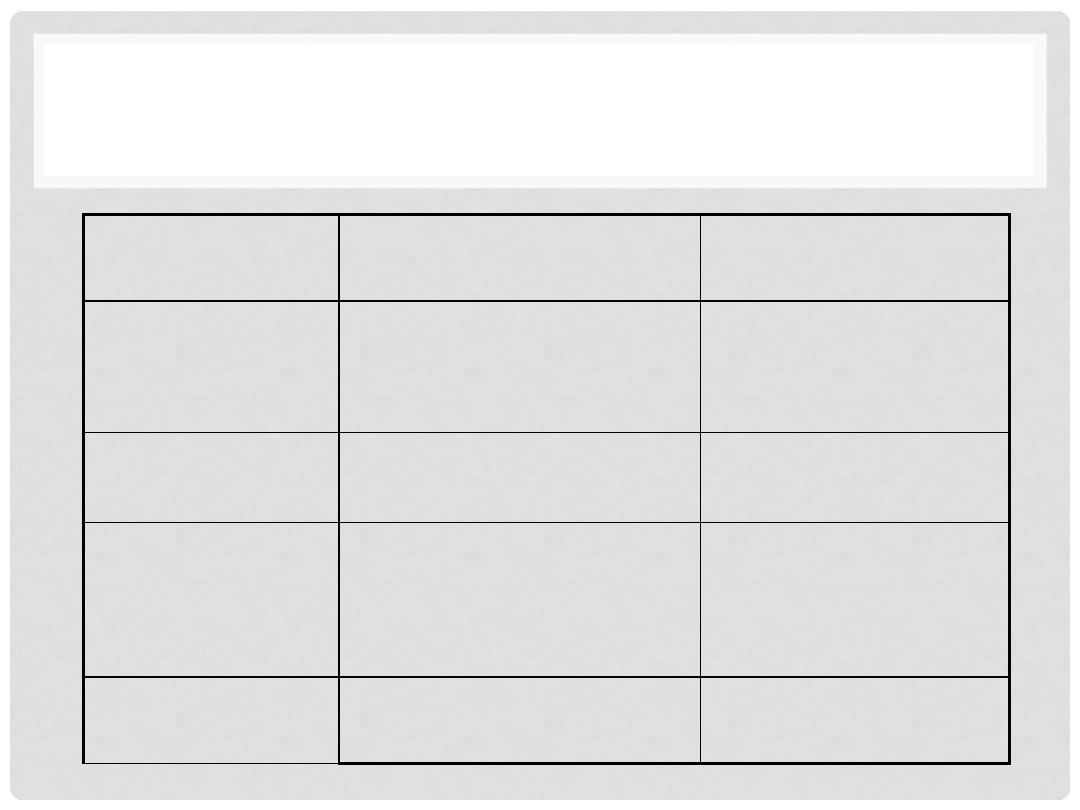
BENIGN VS MALIGNANT FEATURES
Feature
Benign
Malignant
Rate of growth
Progressive but slow.
Mitoses few and normal
Variable. Mitoses
more frequent and
may be abnormal
Differentiation
Well differentiated
Some degree of
anaplasia
LOCAL INVASION
Cohesive growth.
Capsule & BM not
breached
Poorly cohesive and
infiltrative!
Metastasis
Absent
May occur
Lectures of Dr. Mohanad Aljanabi / Oncology
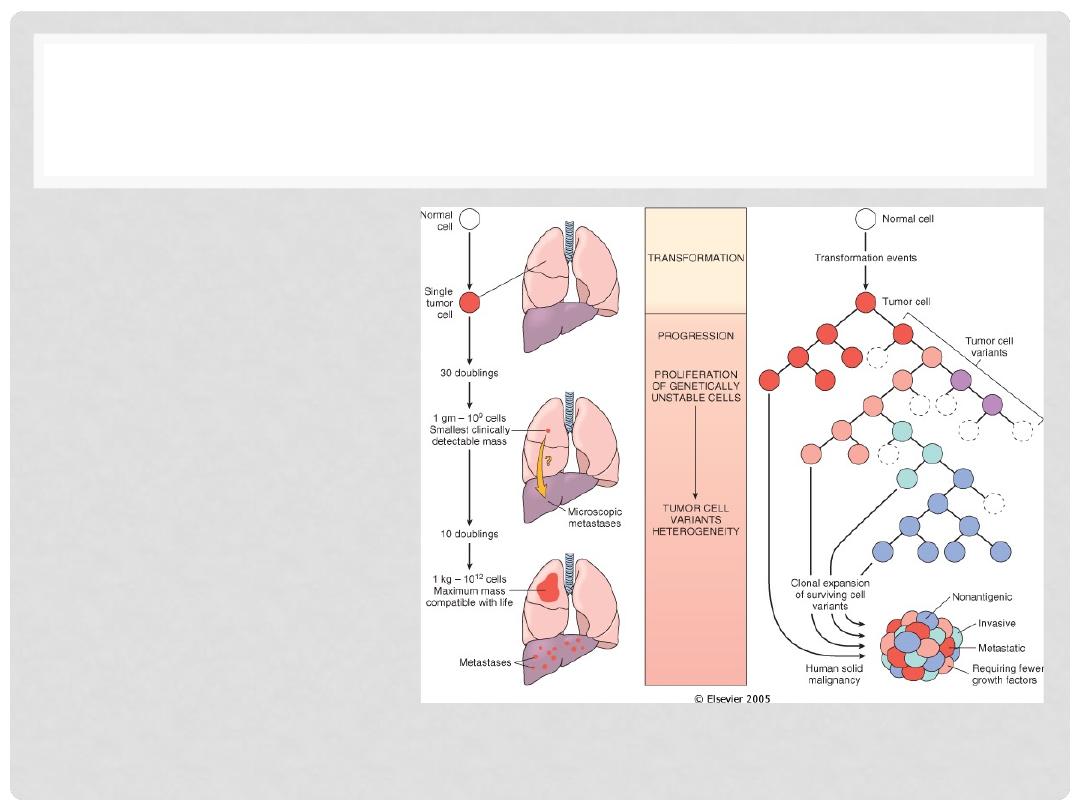
HOW TUMOR GROW?!
•
Malignant Change
in target cells
(
transformation
)
•
Growth of the
transformed cells
•
Local invasion
•
Distant metastases
Lectures of Dr. Mohanad Aljanabi / Oncology
CLASSIFICATION OF TUMOR
•
Epithelial tumors
•
Benign forms – adenoma , papilloma
•
Malignant forms – carcinoma, eg adenocarcinoma,
squamous cell carcinoma
•
Mesenchymal tumors
•
Benign forms – fibroma, leiomyoma,
•
Malignant forms – sarcoma, eg fibrosarcoma,
leiomyosarcoma
Lectures of Dr. Mohanad Aljanabi / Oncology
CLASSIFICATION OF TUMOR
•
Tumors of lymphocytes are always malignant –
called
lymphoma
•
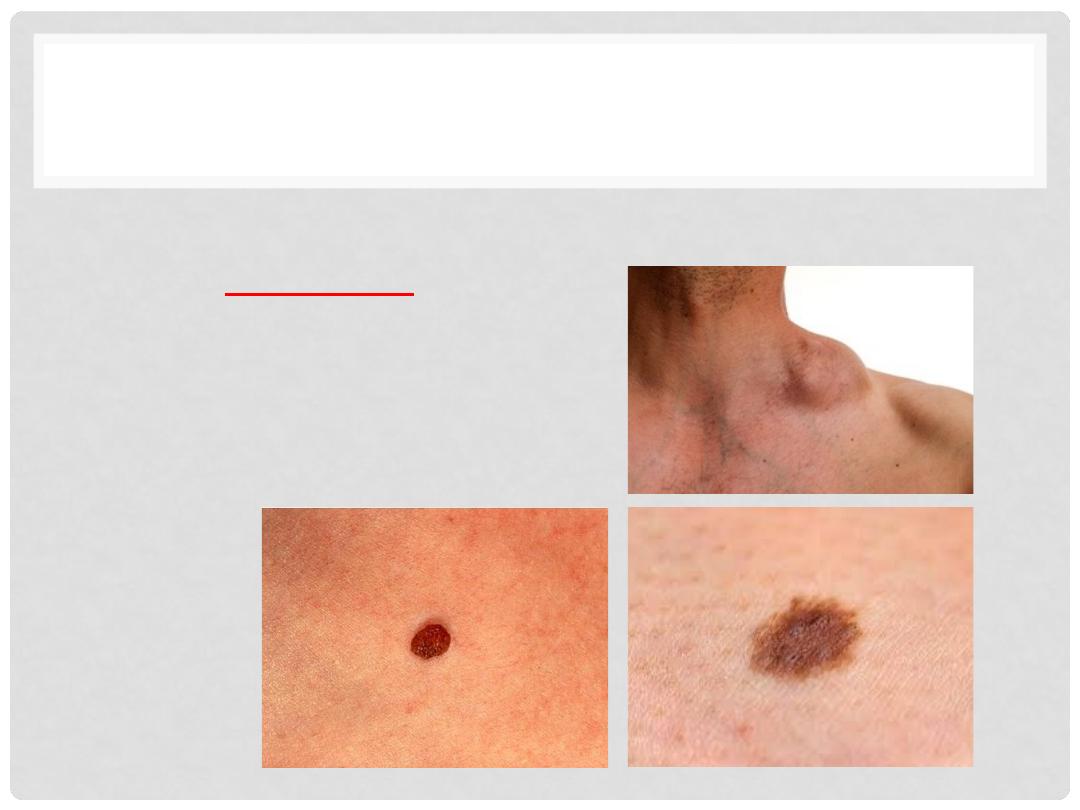
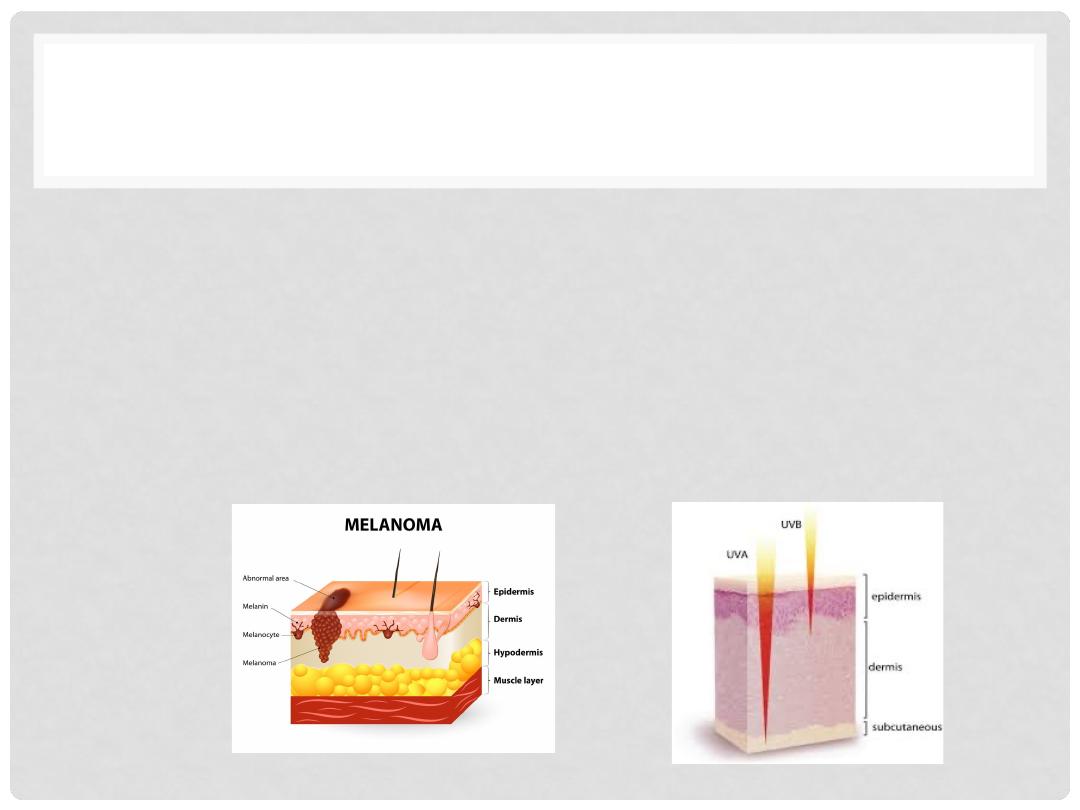
Tumors of melanocytes
•
Benign – nevus
•
Malignant - melanoma
Lectures of Dr. Mohanad Aljanabi / Oncology
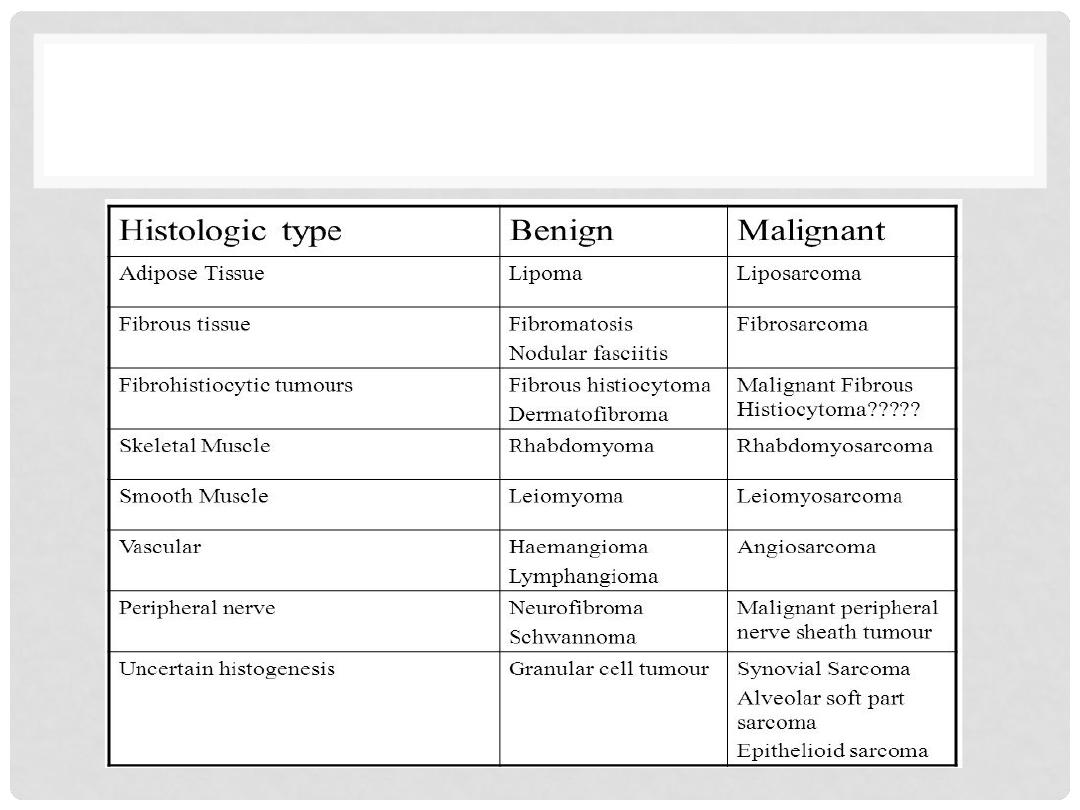
CLASSIFICATION OF TUMOR
Lectures of Dr. Mohanad Aljanabi / Oncology
Classification/Nomenclature
Classification by tissue type:
• carcinoma
epithelial cell
90% of all tumours
derived from ectoderm (mostly) or
endoderm (some)
• sarcoma
connective tissue
2% of all tumours
derived from mesoderm
• leukaemia
circulatory or lymphatic
8% of all tumours
derived from mesoderm
Classification by the type of cells:
• Adenomatous cells
ductal or glandular cells
• Squamous cells
flat cells
• Myeloid
blood cell
• Lymphoid
lymphocytes or macrophages
Cancer is many diseases with one commonality
Lectures of Dr. Mohanad Aljanabi / Oncology
GRADING/STAGING
•
GRADING
: HOW “DIFFERENTIATED” ARE THE CELLS?
•
STAGING
: HOW MUCH ANATOMIC EXTENSION?
TNM
Which one of the above do you think is more
important?
Lectures of Dr. Mohanad Aljanabi / Oncology
CELLULAR
DIFFERENTIATION/GRADING
•
Tumors are often“
graded
”
as to how closely they
resemble the normal parent tissue that they are
derived from
•
Well-differentiated means the cells are very similar in
appearance and architectural arrangement to
normal tissue of that organ
Lectures of Dr. Mohanad Aljanabi / Oncology
TYPES OF TUMOR DIFFERENTIATION
•
Well differentiated neoplasm
•
Resembles mature cells of tissue of origin
•
Poorly differentiated neoplasm
•
Composed of primitive cells with little differentiation, does NOT
resemble tissue of origin
•
show only minimal resemblance to the normal parent tissue they are
derived from
•
Undifferentiated or
“
anaplastic
”
tumor
•
shows no obvious similarity to its parent tissue, usually associated with
aggressive behavior
•
Correlation with biologic behavior
•
Benign tumors are well differentiated
•
Poorly differentiated malignant tumors usually have worse prognosis
Lectures of Dr. Mohanad Aljanabi / Oncology
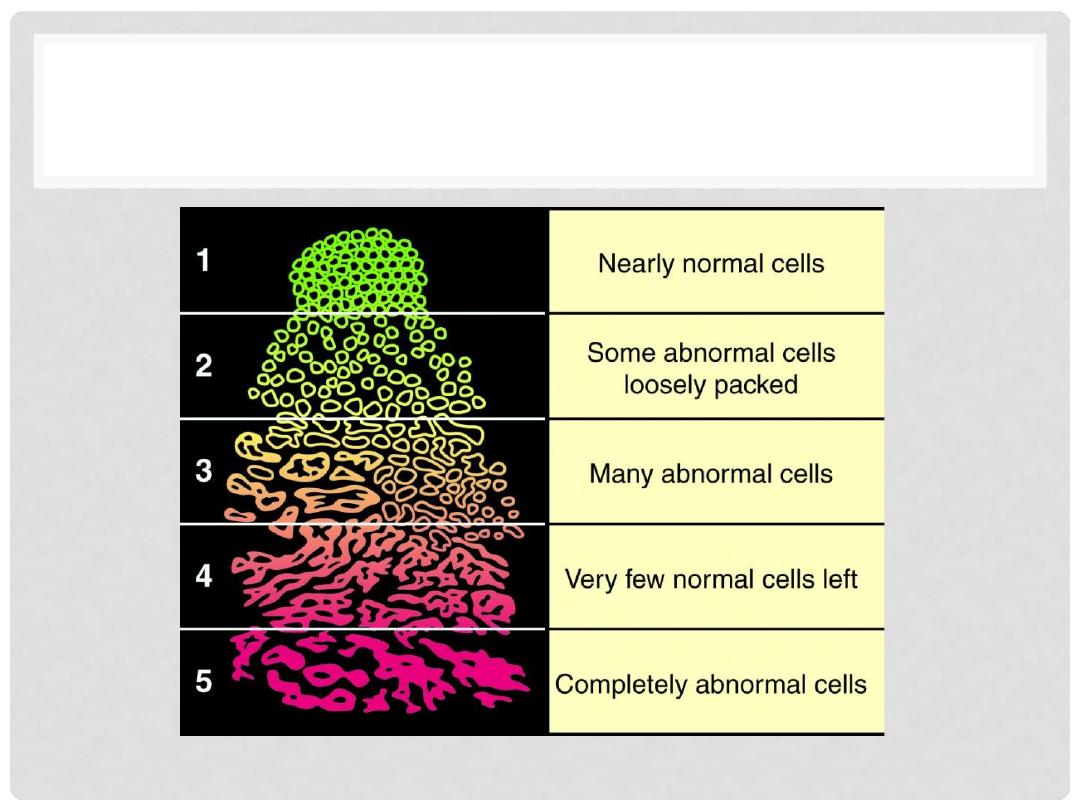
TUMOR GRADING
Lectures of Dr. Mohanad Aljanabi / Oncology
WHY DOES DIFFERENTIATION
MATTER?!
•
Differentiation
provides clues
as to the clinical aggressiveness of
the tumor
•
Tumors
lose differentiation
features over time as they become
more “malignant”; they acquire more
cumulative genetic
mutations
•
Predicts responsiveness to certain therapies, e.g. estrogen
receptors and Tamoxifen in breast cancers
Lectures of Dr. Mohanad Aljanabi / Oncology
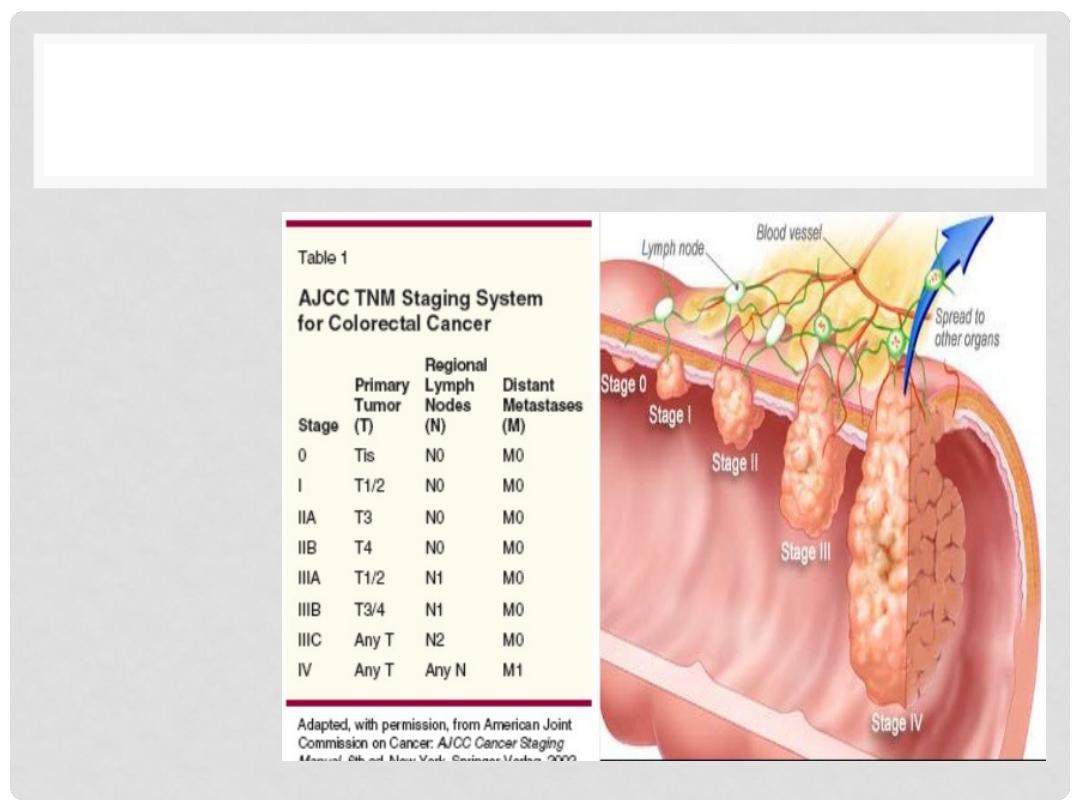
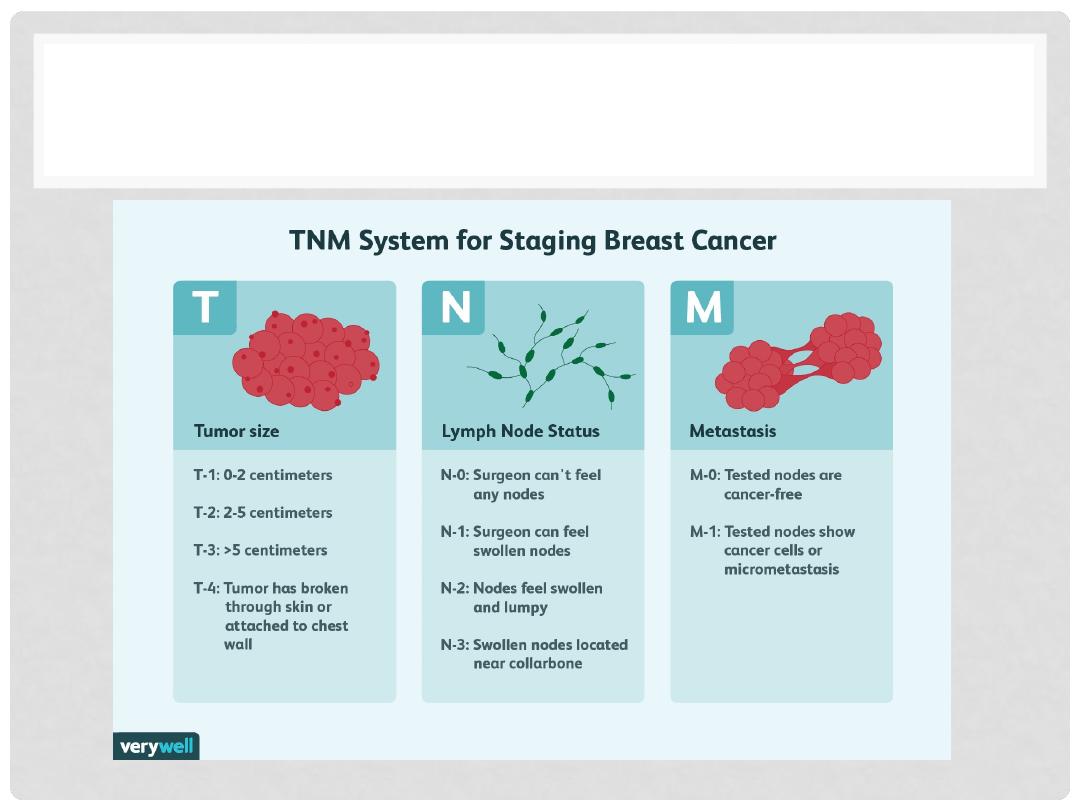
TUMOR STAGING
•
TNM
system
•
Size
•
Lymph
Node
•
Metastasis
Lectures of Dr. Mohanad Aljanabi / Oncology
TUMOR STAGING
Lectures of Dr. Mohanad Aljanabi / Oncology

MOLECULAR BASIS OF CANCER
•
NON-lethal
genetic damage, “usual” suspec.
•
A tumor is formed by the clonal expansion of a single
precursor cell (
monoclonal
)
•
Four classes
of normal regulatory genes
•
PROTO-oncogenes
•
Oncogenesà Oncoproteins
•
DNA repair genes
•
Apoptosis genes
•
Carcinogenesis is a
multistep
process
Lectures of Dr. Mohanad Aljanabi / Oncology
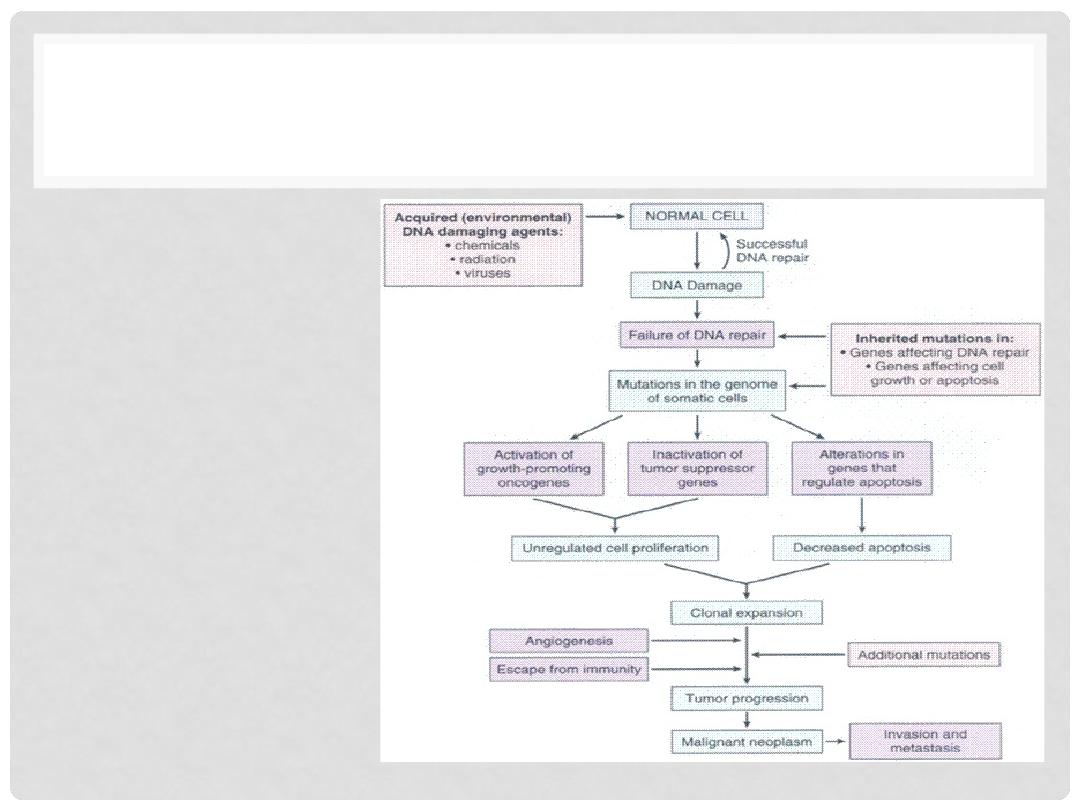
MOLECULAR BASIS OF CANCER
•
DNA damage
•
Somatic mutation
•
Activating growth
promoting genes
•
Decrease apoptosis
•
Clonal expansion
•
Tumor transformation
•
Tumor progression
Lectures of Dr. Mohanad Aljanabi / Oncology

THE 6 HALLMARKS OF CANCER!
Lectures of Dr. Mohanad Aljanabi / Oncology
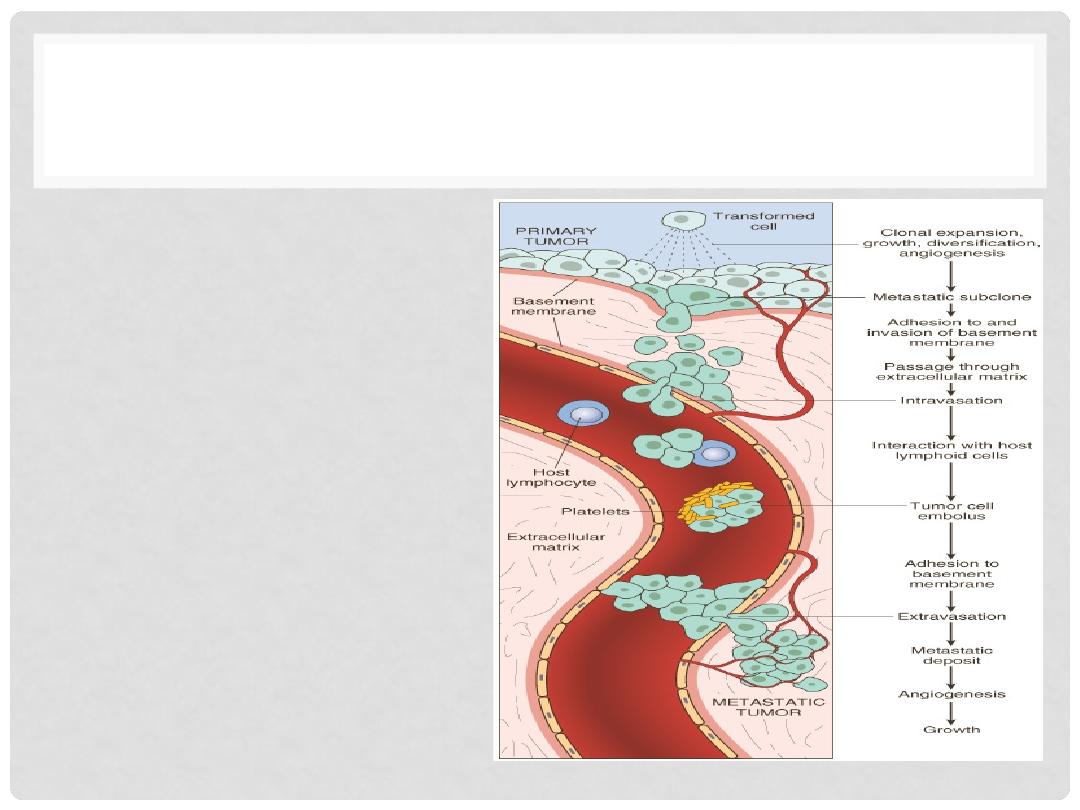
HOW CAN TUMOR CELL METASTASIZE?
TRANSFORMATIONà
GROWTHà
BM INVASIONà
ANGIOGENESISà
INTRAVASATIONà
EMBOLIZATIONà
ADHESIONà
EXTRAVASATIONà
METASTATIC GROWTHà
etc.
Lectures of Dr. Mohanad Aljanabi / Oncology
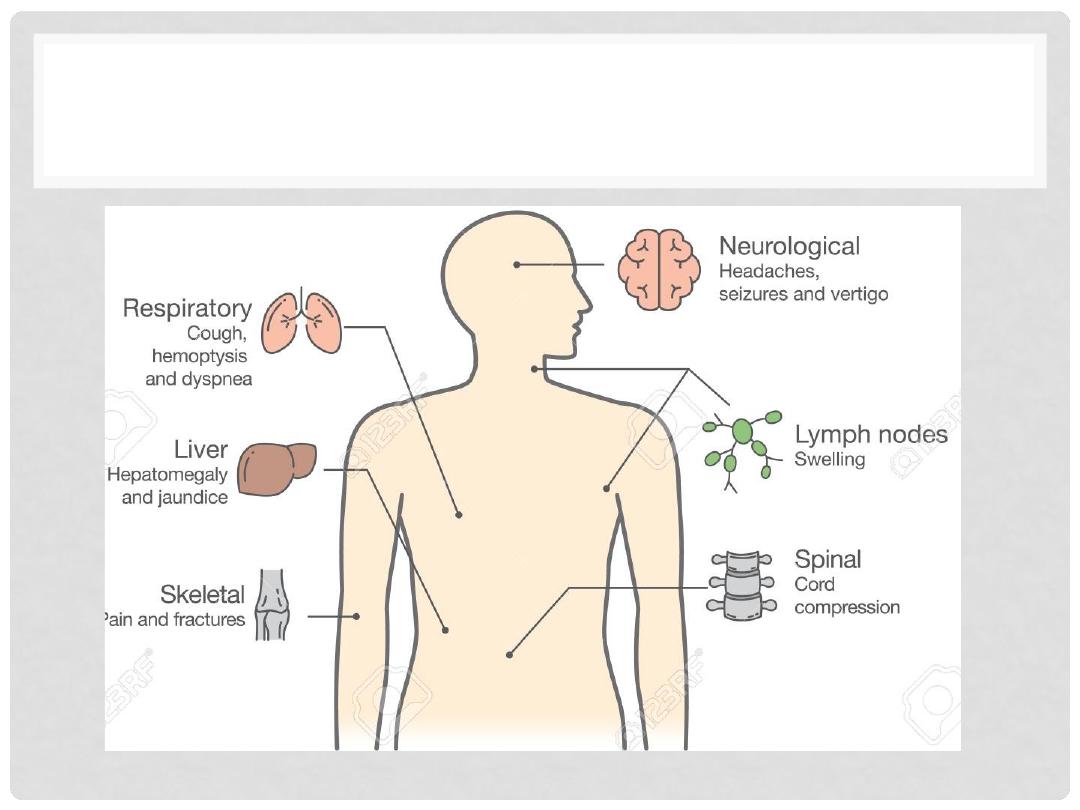
COMMON SITE OF METASTASIS
Lectures of Dr. Mohanad Aljanabi / Oncology
CANCER IMMUNITY
•
Screen unhealthy
cells
•
Eliminate cancer
cells
•
Provide specific
defense
•
Most cancers
have escaped
the screening
Lectures of Dr. Mohanad Aljanabi / Oncology
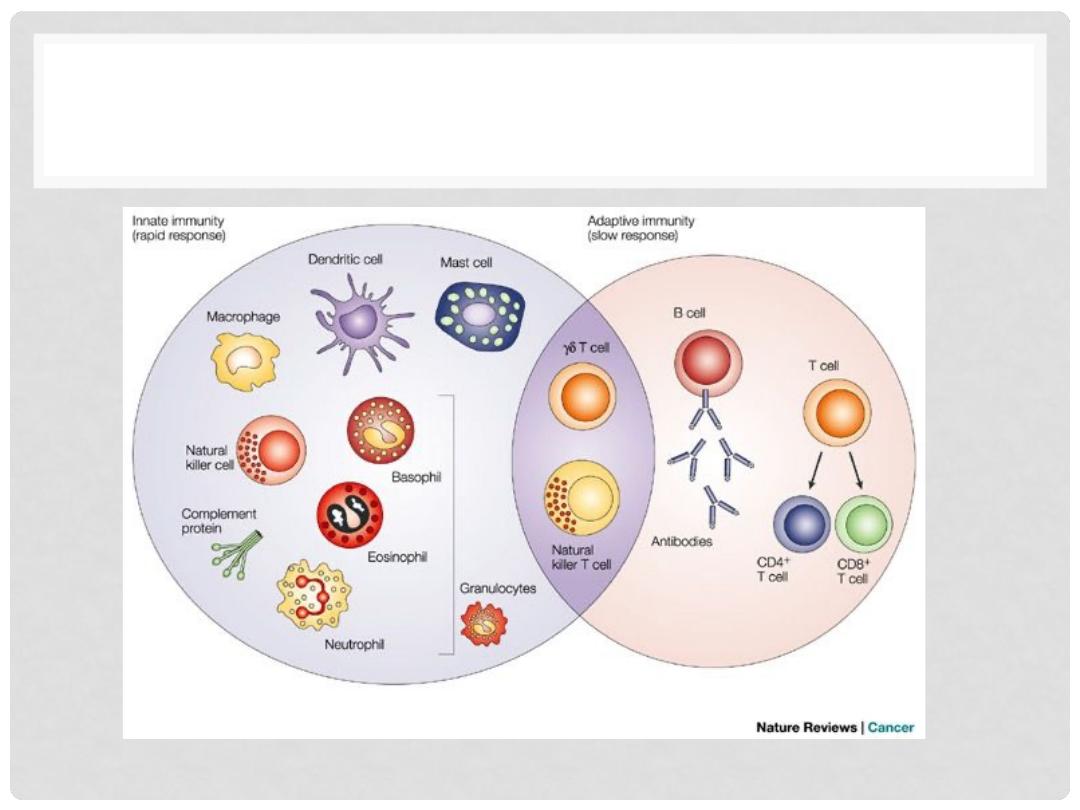
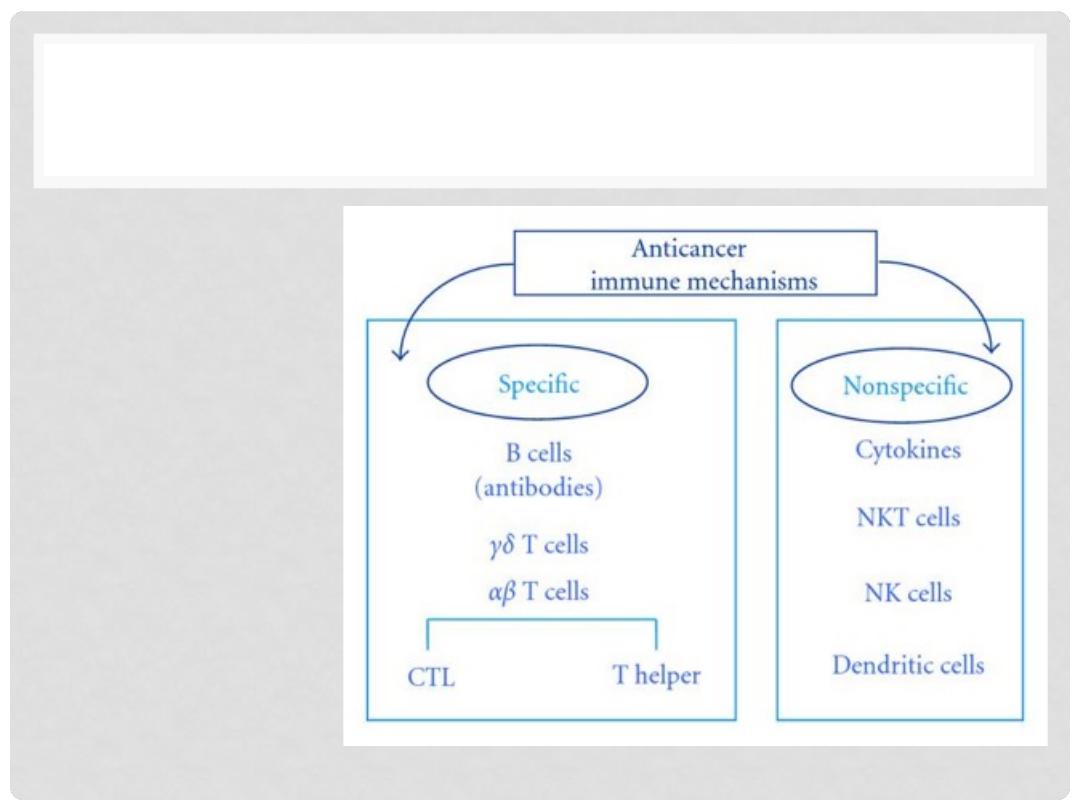
IMMUNE DEFENSE AGAINST CANCER
Lectures of Dr. Mohanad Aljanabi / Oncology
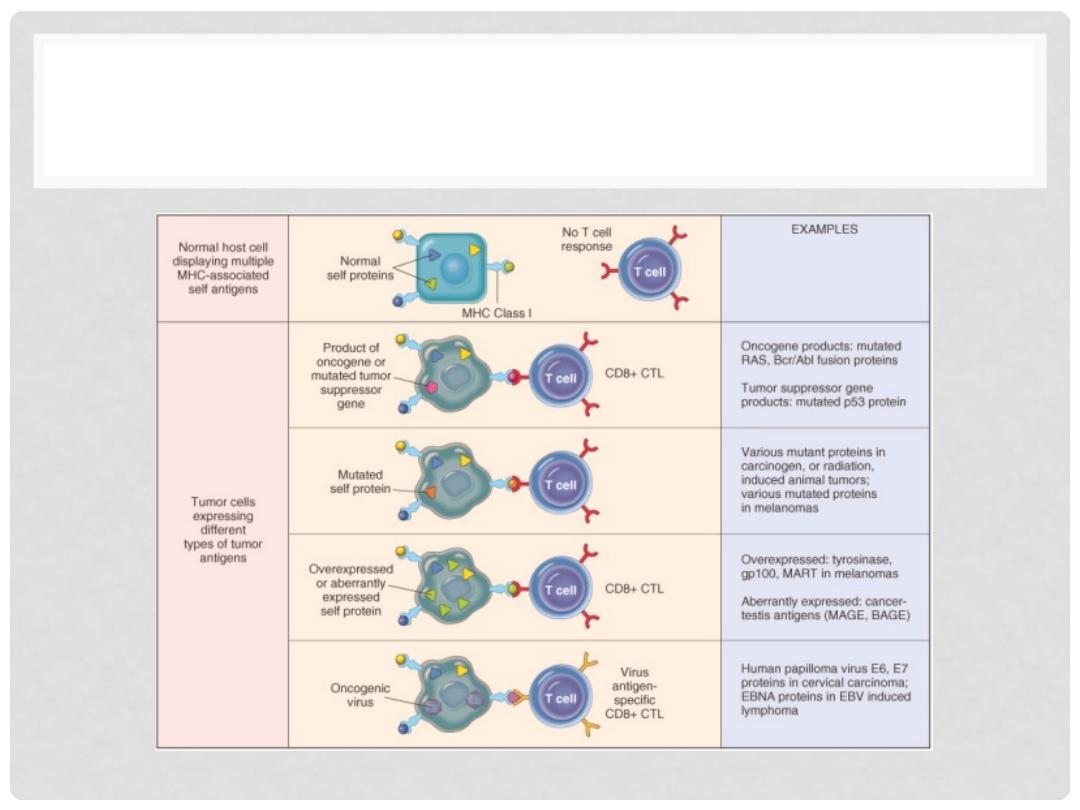
T CELLS ARE THE MAIN PLAYERS
Lectures of Dr. Mohanad Aljanabi / Oncology
CAUSES OF CANCER
•
Most cancer arises as the result of
somatic
mutations
in the genome resulting from:
•
Chance (ie, we dont know)
•
Environmental factors – chemical, radiation, viruses
•
Ageing
•
Inherited
cancer syndromes-
defect in germline
DNA
Lectures of Dr. Mohanad Aljanabi / Oncology
ENVIRONMENTAL CARCINOGENS
•
Sun exposure
•
Melanomas 6x incidence New Zealand vs. Iceland
•
Blacks have low incidence of melanoma, so do normally
pigmented areas like areolae on white people
•
Smoking and alcohol abuse
•
Body mass
•
Overweight = 50% increase in cancer
•
Environmental vs. racial factors
•
Japanese immigrants to USA
•
Viral exposure
•
Human papilloma virus (HPV) and cervical cancer
•
Hepatitis B virus (HBV) and liver cancer (Africa, Asia)
•
Epstein-Barr Virus (EBV) and lymphoma
Lectures of Dr. Mohanad Aljanabi / Oncology
PREDISPOSING FACTORS FOR CANCER
•
Age
•
Most cancers occur in persons ≥ 55 years
•
Childhood cancers
•
Leukemias & CNS neoplasms
•
Bone tumors
•
Genetic predispostion
•
Familial cancer syndromes
•
Early age at onset
•
Two or more primary relatives with the cancer (“soil” theory)
•
Multiple or bilateral tumors
•
Polymorphisms that metabolize procarcinogens, e.g., nitrites
•
Nonhereditary predisposing conditions
•
Chronic inflammation?
•
Precancerous conditions
•
Chronic ulcerative colitis
•
Atrophic gastritis of pernicious anemia
•
Leukoplakia of mucous membranes
•
Immune collapse?
Lectures of Dr. Mohanad Aljanabi / Oncology
RADIATION
•
Ionizing radiation
– x-rays, gamma rays, radioactive
materials such as Radon gas – all cause a variety of
defects to DNA
•
UV light (non-ionizing)
– primarily sun-exposure and T-T
dimerization – skin cancers
Lectures of Dr. Mohanad Aljanabi / Oncology
ONCOVIRUSES
•
HPVà Cervical Cancer
•
EBVà Burkitt Lymphoma
•
HBVà Hepatocellular Carcinoma (Hepatoma)
•
HTLV1à T-Cell Lymphoma
•
KSHVà Kaposi Sarcoma
•
Can Bacteria cause Cancer???
Lectures of Dr. Mohanad Aljanabi / Oncology
CANCER DIAGNOSIS
•
Symptoms (history and clinical signs)
•
Radiological studies
•
BIOPSY for pathological studies
•
CYTOLOGY: (exfoliative)
•
CYTOLOGY: (FNA,
F
ine
N
eedle
A
spirate)
Lectures of Dr. Mohanad Aljanabi / Oncology

CANCER SIGNS
•
Signs and symptoms vary from one cancer to another
•
Eight early signs that
might
indicate cancer
Lectures of Dr. Mohanad Aljanabi / Oncology
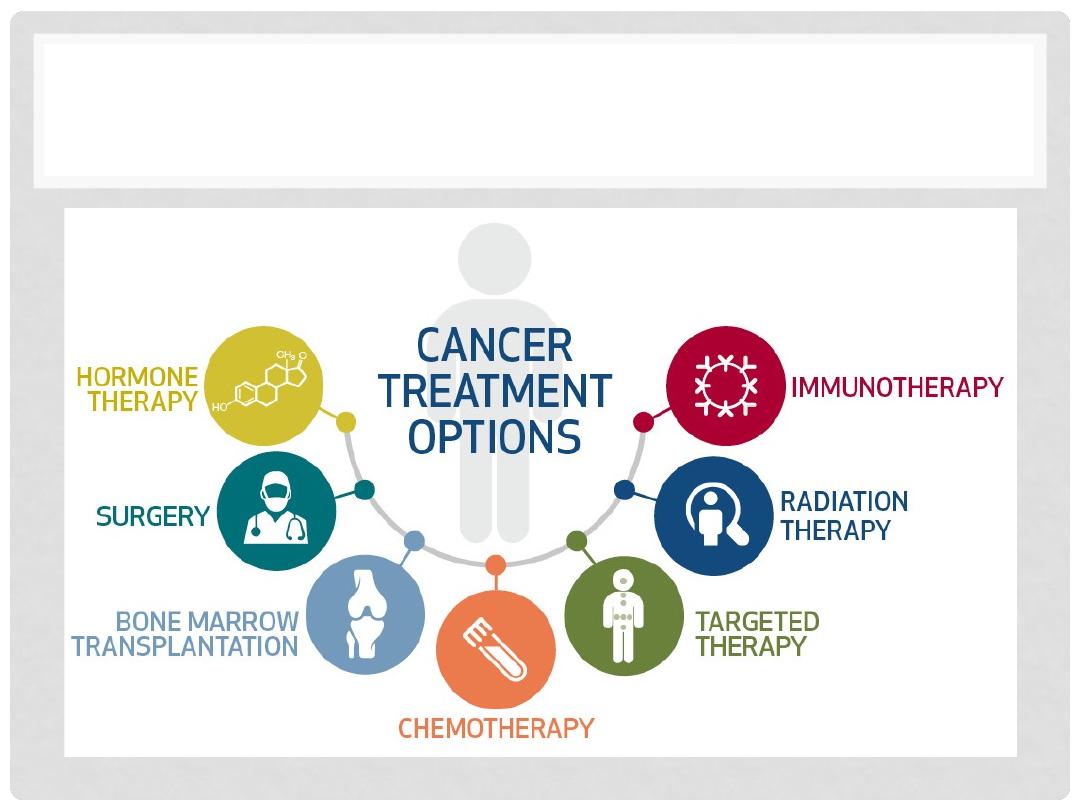
CANCER TREATMENTS
Lectures of Dr. Mohanad Aljanabi / Oncology
45
CANCER TREATMENT
•
Chemotherapy
•
Cytotoxic drugs + body defenses
•
Single agent
•
Combination chemotherapy
•
Radiation
•
targets DNA
•
kill tumor without damage to surrounding
tissues
•
tumor must be accessible
Lectures of Dr. Mohanad Aljanabi / Oncology
46
CANCER TREATMENT
•
Surgery
•
method of choice
•
can remove entire tumor
•
Debulking
•
adjuvant chemotherapy or radiation
palliation
Lectures of Dr. Mohanad Aljanabi / Oncology
CANCER TREATMENT
•
Immunotherapy
•
Nonspecific enhancement of the immune system –
interferons or interleukins
•
protect against recurrence
•
eliminates cancer cells only
•
T- cell based or antibody responses
•
Conjugated antibodies
Lectures of Dr. Mohanad Aljanabi / Oncology
48
SIDE EFFECT OF CANCER TREATMENT
•
Gastrointestinal tract:
•
Oral ulcers
•
Malabsorption
•
Diarrhea
•
Vomiting – caused by effects on CNS
•
Bone marrow:
•
chemo and radiation suppress bone marrow
•
decrease in red blood cells, white blood cells and platelets
Lectures of Dr. Mohanad Aljanabi / Oncology
49
SIDE EFFECT OF CANCER TREATMENT
•
Hair and skin:
•
alopecia
•
skin breakdown and dryness
•
Reproductive tract:
•
affects gametes
•
premature menopause
•
also due to damage of hypothalamus and/or pituitary
•
sperm or embryo bank?!
Lectures of Dr. Mohanad Aljanabi / Oncology
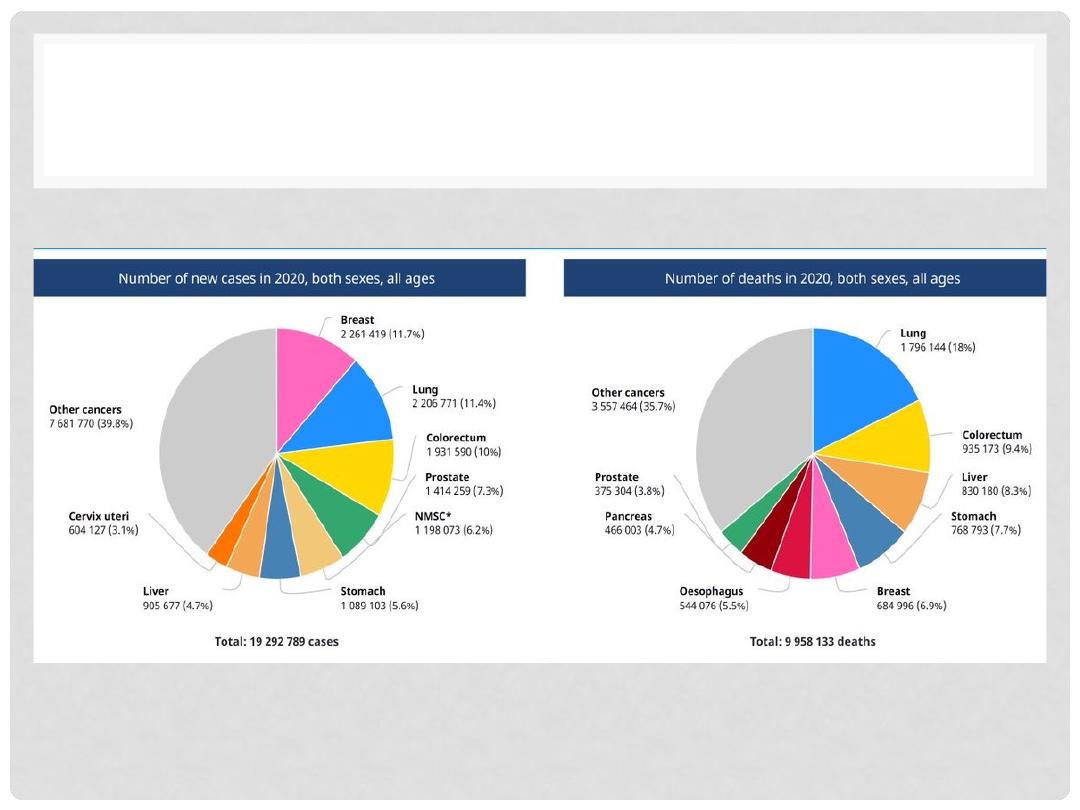
CANCER EPIDEMIOLOGY
Lectures of Dr. Mohanad Aljanabi / Oncology
Questions & Comments