Physiology
Of blood

WBCs” Leucocyte”
Lect. 6
Ministry of Defense is WBCs
وزارة الدفاع في جسم االنسان

O
BJECTIVES
:
1. What are the
WBC
cells in our body?
2. Define
their role in
blood .
3. Determine its
type and function
.
4. Describe the pathological states of
Leukocytosis & Leucopenia
The leukocytes, also called white blood cells, are the mobile units of
the body’s protective system. They are formed
partially
in the bone
marrow (
granulocyte and monocytes
) and
partially
in the lymph
tissue (
lymphocytes and plasma cells
).
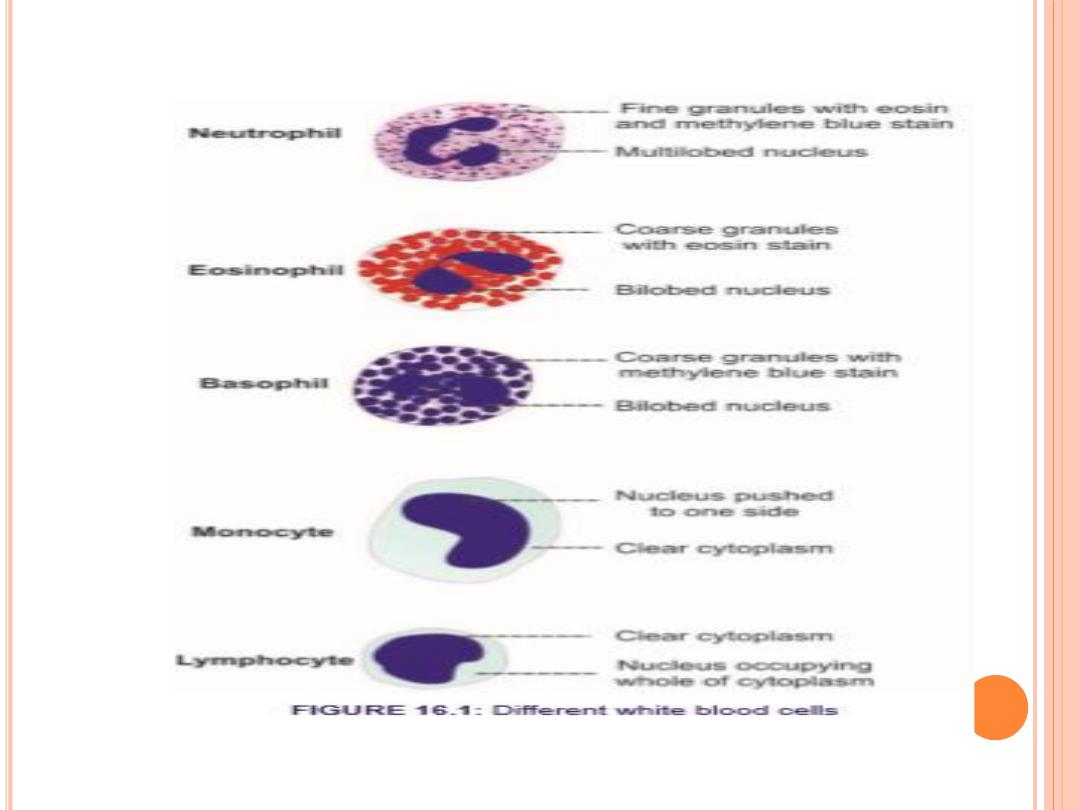
Six types of WBCs
are normally present in the blood.
1.Polymorphonuclear
Neutrophils
they have granular cytoplasm
2. Polymorphonuclear
Eosinophils,
3.Polymorphonuclear
Basophils,
4.
Monocytes,
5.
Lymphocytes
,
with the immune system..
6.
Plasma cells
.
***The granulocytes and monocytes protect the body against
invading organisms mainly by ingesting them— phagocytosis.
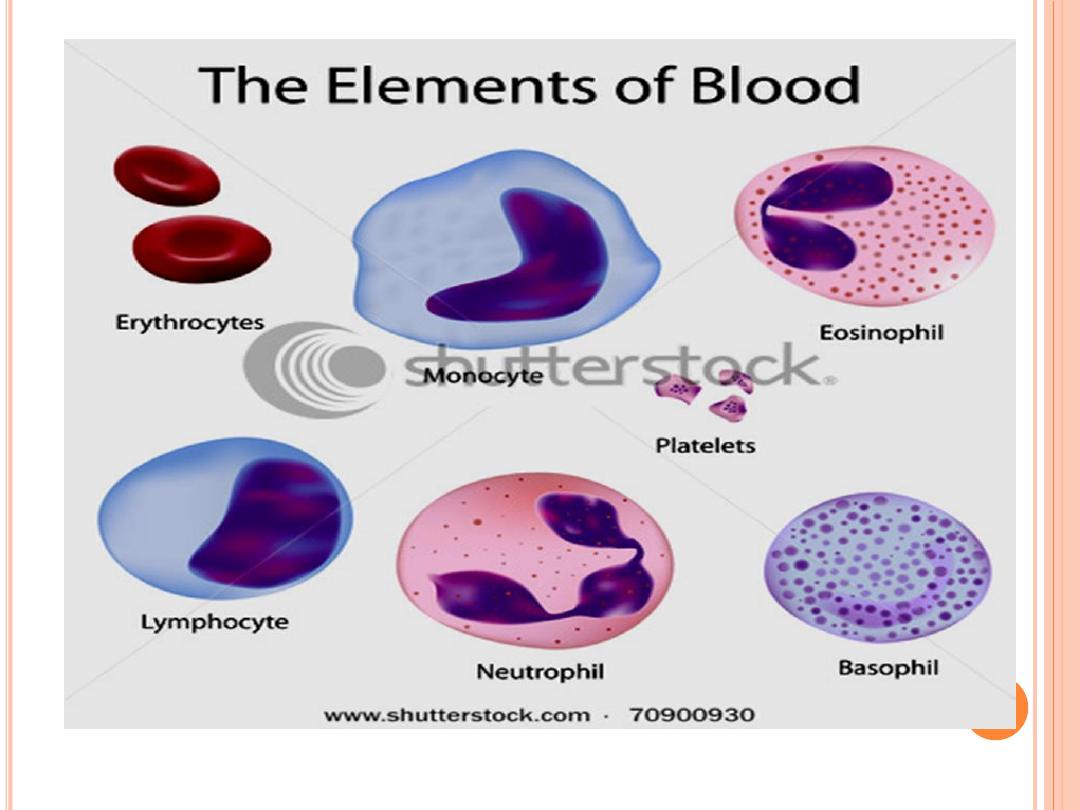

WBCs are the colorless and
nucleated
formed elements
of blood
Compared to
RBCs,
the
WBCs
are larger in size and
lesser in number, have a role in defense mechanism of
body and protect the body from invading organisms .
The differences between
WBCs and RBCs are:
1.
Larger in size.
2.
2. Irregular in shape.
3.
3. Nucleated.
4.
4. Many types.
5.
5. Granules are present in some type of WBCs.
6.
6. Lifespan is shorter.

O
RIGINS AND
D
IFFERENTIATION OF
F
ORMED
E
LEMENTS
All blood cells originate from
hemocytoblasts:
which produce myeloid stem cells and lymphoid stem
cells
Myeloid Stem Cells
Differentiate into progenitor cells:
which produce all WBCs except lymphocytes
Lymphocytes
Are produced by lymphoid stem cells
Lymphopoiesis: the production of lymphocytes.
WBCs, except monocytes: develop fully in bone
marrow i. e develop into macrophages in peripheral
tissues
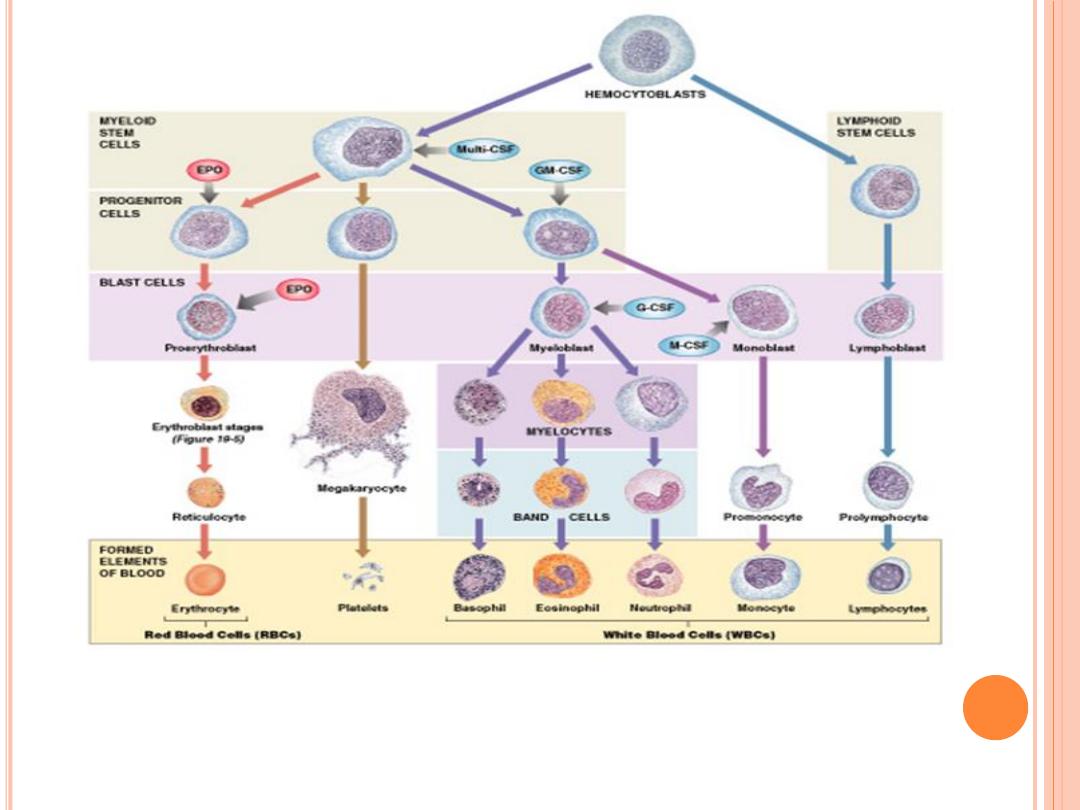

Hormones that regulate blood cell populations:
Colony-Stimulating Factors (CSFs)
1.
M-CSF:
stimulates monocyte production
2.
G-CSF:
stimulates granulocyte production neutrophils, eosinophils, and basophils
3.
GM-CSF:
stimulates granulocyte and monocyte production
4.
Multi-CSF:
accelerates production of granulocytes, monocytes, platelets, and RBC
CLASSIFICATION
Based on the presence or absence of granules in the cytoplasm, the leukocytes are
classified into two groups:
1.
Granulocytes
which have granules.
2.
Agranulocytes
which do not have granules
**Granulocytes
Depending upon the staining property of granules, the granulocytes are classified
into three types:
i. Neutrophils with granules taking both acidic and basic stains.
ii. Eosinophils with granules taking acidic stain.
iii. Basophils with granules taking basic stain.
** Agranulocytes
have plain cytoplasm without granules are of two types:
i.
Monocytes.
ii.
ii. Lymphocytes
C
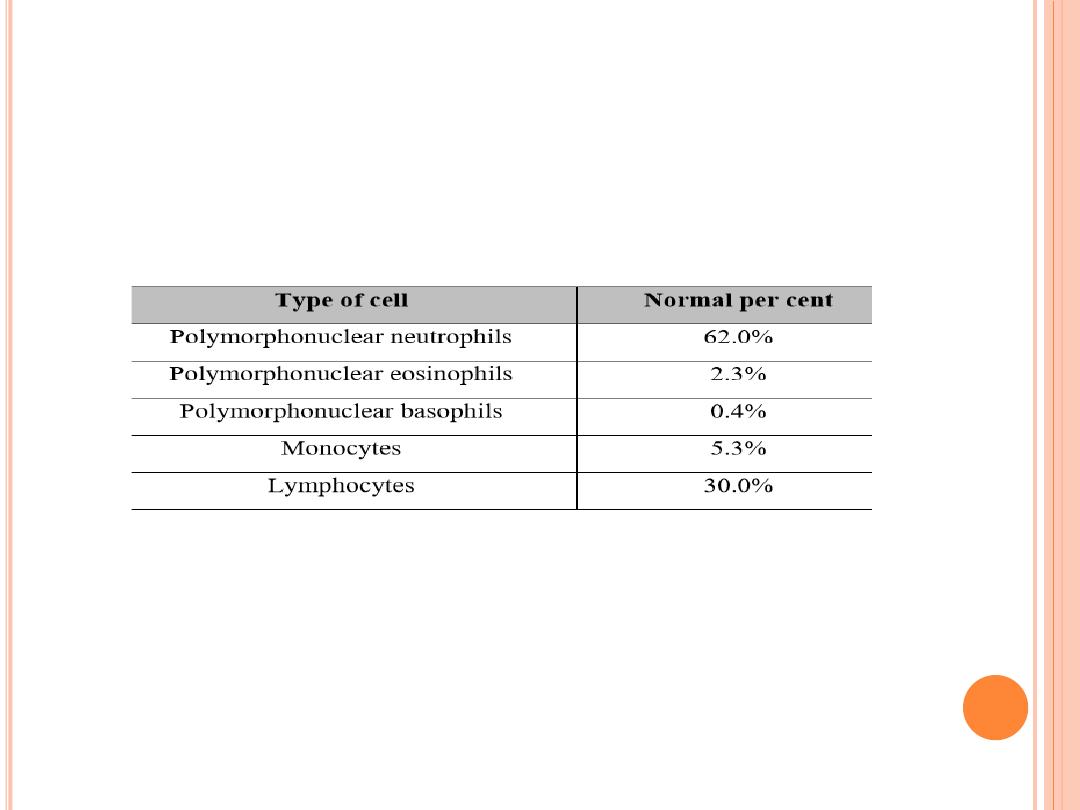
ONCENTRATIONS OF THE
D
IFFERENT
W
HITE
B
LOOD
C
ELLS IN THE
B
LOOD
.
The adult human being has about
7000 white
blood cells per microliter
of blood (in comparison with
5 million red
blood cells). Of the total
white blood cells, the normal percentages of the different types are
approximately the following:
Circulating WBCs
Migrate out of bloodstream
Have amoeboid movement
Attracted to chemical stimuli (positive chemotaxis)
Some are phagocytic: as neutrophils, eosinophils, and monocytes

L
IFE
S
PAN OF THE
W
HITE
B
LOOD
C
ELLS
The life of the
granulocytes
after being released from the bone
marrow is normally
4 to 8 hours
circulating in the blood and another
4 to 5 days
in tissues where they are needed.
The
monocytes
have a short time, 10 to 20 hours in the blood. Once
in the tissues, they swell to much larger sizes to become
tissue
macrophages
, can live for months unless destroyed while performing
phagocytic functions.
It is mainly the
neutrophils and tissue macrophages
that attack and destroy
invading bacteria, viruses, and other injurious agents by a
phagocytosis,
which means cellular ingestion of the offending agent.
The neutrophile has
a lysosomal enzymes & bactericides
(hydrogen peroxide and superoxide)
The macrophage are much more powerful phagocytes than neutrophils,
often capable of phagocytizing as many as 100 bacteria with the ability to
engulf much larger particles, even whole RBCs or, occasionally, malarial
parasites, whereas neutrophils are not capable of phagocytizing particles
much larger than bacteria.
Eosinophils
are weak phagocytes, they are produced in large numbers
in people with parasitic infections, and they migrate in large
numbers into tissues diseased by parasites , and allergic reactions as in
bronchial tissues of the lungs in people with
asthma
The
basophils
play an important role in some types of allergic reactions
that its release
histamine, bradykinin and serotonin
. basophils liberate
heparin
into the blood, a substance that can prevent blood coagulation
The mast cells and basophils play an important role in some types of
allergic reaction because the type of antibody that causes allergic
reactions, the
immunoglobulin E
(IgE)
type, has a special propensity to
become attached to mast cells and basophils.
Lymphocytes
enter the circulatory system continually, the lymphocytes have life
spans of weeks or months; this depends on the body’s need for these cells.
3 Types
:
1-T cells
Cell-mediated immunity ( Attack foreign cells directly)
2- B cells
Humoral immunity (Differentiate into plasma cells
(activated B cells that secrete antibodies)
3-Natural killer (NK) cells
Detect and destroy abnormal tissue cells
(cancers)

PHYSIOLOGICAL VARIATIONS
1. Age:
WBC count is about
20,000 per cu
mm in
infants
and
about
10,000 to 15,000 per cu
mm of blood in
children
. In
adults, it ranges between 4,000 and 11,000 per cu mm of
blood.
2. Sex: Slightly more in
males
than in females.
3. Diurnal variation: Minimum in early
morning
and
maximum in the afternoon.
4.
Exercise
: Increases slightly.
5.
Sleep
: Decreases.
6. Emotional conditions like
anxiety
: Increases.
7.
Pregnancy
: Increases.
8.
Menstruation
: Increases.
NORMAL WHITE BLOOD CELL COUNT
Total WBC count : 4,000 to 11,000/cu mm of blood.
„
PATHOLOGICAL VARIATIONS
All types of leukocytes do not share equally in the increase or decrease of total
leukocyte count. In general, the neutrophils and lymphocytes vary in opposite
directions.
Leukocytosis
occurs in conditions such as:
1.Infections 2. Allergy 3. Common cold 4. Tuberculosis 5. Glandular fever.
Leukopenia
is the decrease in the total WBC count , occurs in :
1. Anaphylactic shock 2. Cirrhosis of liver 3. Disorders of spleen 4. Pernicious anemia 5.
Typhoid and paratyphoid 6. Viral infections
Granulo
cytosis
Granulocytosis is the abnormal increase in the number of granulocytes.
Granulocyto
penia
Granulocytopenia is the abnormal reduction in the number of granulocytes.
Leukemia
is the condition which is characterized by abnormal and uncontrolled
increase in leukocyte count more than 1,000,000/cu mm. It is also called blood cancer.

Mechanism of Defense of Neutrophils & Monocytes Against
Infection
Neutrophils & monocytes attack & destroy invading organisms like
bacteria, virus or other foreign agents.
The mechanism of destruction of bacteria include:
1.
Margination
:
Sticking
of leukocytes to endothelial cells in the capillary wall.
2.
Diapedesis
:
Squeezing
of leukocytes through capillary wall.
3.
Amoeboid motion
:
Movement
of leukocytes in the tissue with speed up to 40 μ/min
4.
Chemotaxis
: Movement of the leukocytes to the site of infection by the effect of
different substances like:
bacterial toxins, degenerative substances of tissue,
reactive products of complement (C5a) & clotting system, leukotrienes & polypeptide
for lymph
.
Chemotaxis depends on concentration gradient of chemical substance which is
effective up to
100 μm
away from site of inflammation.
Movement of neutrophils by
diapedesis
through capillary pores and by
chemotaxis
toward an area of tissue damage


البلعمة
5.Phagocytosis
:
(
ingestion of the offending agent
) cell
to be phagocytized:
a) Devoted from protective protein (Dead cell & foreign particles).
b) Some cells are recognized by Antibody adhere to bacteria with complement proteins
الهاضمة
(
Opsonization
)
Mechanism of phagocytosis
the neutrophil first attaches itself to the particle (attachment of bacteria on Ab-Ag
complex to cell).
Project of pseudopodia around particles then fused to form
phagosome
(vesicle).
Enzymatic digestion of phagocytized particles
Lysosome
fuse to vesicle to release digestive enzymes like
proteolytic enzymes
with sharp rise in
O
2
uptake with respiratory burst.
Macrophages also contain
lipases
to digest lipid membrane of TB.
If bacteria cannot be digested so it will be killed by
oxidizing agent
as superoxide (O
2
), hydrogen
peroxide (H
2
O
2
) & hydroxyl on (OH
Neutrophils are mature WBC can
start phagocytosis
of bacteria
immediately
, up to
20 bacteria
can be phagocytized before inactivation & death.
Monocytes
are immature, then as they go to tissue swollen to
5x
its diameter (
80 μ
) &
develop lysosomes & mitochondria in cytoplasm to be
macrophage
,as activated by
immune system they become powerful
>
than neutrophil (up to
100 bacteria
), dead
neutrophil, necrotic tissue, malarial parasite & even RBC can be engulfed and then can
extrude the residual products

Monocyte – macrophage system (
Reticuloendothelial system
):
It represented by combination of monocytes, mobile macrophages, fixed tissue
macrophages and a few specialized endothelial cells in B.M., spleen, and lymph nodes.
Tissue macrophages
in
skin
called
Histiocytes
.
in
spleen
,
lymph node
&
Bone.Marrow
called
Tissue macrophages
.
in
liver
called
Kupffer cells
.
in
Lung
called
Alveolar cells
.
in
Brain
called
Microglial cells
Inflammation
Local changes in the tissues due to the release of chemical substances like (histamine,
bradykinin, serotonin, prostoglandin, blood clotting products, complement system
products, lymphokines & others), which
strongly activate the macrophage system
.
These substances released as a result of tissue damage by injury, trauma, bacterial or
viral infection, heat & chemical substance.

Response of neutrophils & monocytes to inflammation
:
1.
Tissue Macrophage is the first line of defense against infection
:
within minutes
after inflammation begins; Tissue macrophages start their phagocytic effect).
Their
numbers are not great, but they are life saving
.
2.
Neutrophil invasion of the inflamed area is a second line of defense
:
within the first
hour
or so after inflammation begins, large numbers of neutrophils begin to invade the
inflamed area from the blood. This is caused by inflammatory
cytokines (e.g., TNF, IL-1) and other biochemicalsubstance produced by the inflamed
tissues.
3.
Second Macrophage Invasion into the Inflamed Tissue Is a Third Line of Defense:
•Migration of (immature) monocytes to inflammatory area to become (mature) macrophages.
Its maturation needs
8-12 hours
.
4.
Great increase in production of both granulocytes and monocytes by the Bone Marrow
.
This results from stimulation of the granulocytic and monocytic progenitor cells of the marrow by
factors released mainly by macrophages.
➢ It takes
3 to 4 days
before newly formed granulocytes and monocytes reach the stage of leaving
the Bone Marrow.
Cardinal Signs & Symptoms of Inflammation
(clinically)
Hot
Redness
Swelling
Pain
Loss of Function
