Nutritional factors in disease
Dheyaa Kadhim Al-Waeli - MD, FICMS, MSc. (Endo.)Lecturer: University of Thi-Qar, College of medicine , Department of Medicine
Adult Endocrinologist: Thi-Qar Specialized Daibetes Endocrine and Metabolism Center (TDEMC)
Thi-Qar Internist Association
E-mail: dheyaaalwaeli@yahoo.com
Email: dhiaa.alwaeli@fdemc.iq
ORCID iD:http://orcid.org/ 0000-0001-8738-2205
Clinical assessment and investigation of nutritional status
Ask about weight• Current weight
• Assessment of degree of change
Ask about current food intake
• Quantity , Quality
• Nutritional supplements
• Reliance on supplements/tube feeding
• Change in appetite or interest in food
• Taste disturbance
Important elements of the diet history
Ask about
• Oral ulcers or pain
• Difficulties swallowing
• Nausea/vomiting
• Early satiety
• Alteration in bowel habit
• Abdominal (or other) pain
Ask about activity levels/performance status
• Normal activity
• Slightly reduced activity
• Inactive < 50% of the time
• Inactive most of the time
• Clinical examination in nutritional disorders
• Observation• Signs of weight loss: Prominent ribs Muscle wasting ↓Skin turgor
• Simple anthropometrics
• Body mass index
• Triceps skin fold thickness
• Waist circumference
• Hands
• Muscle wasting (dorsal interossei, thenar eminences)
• Finger clubbing
• Leukonychia (low albumin)
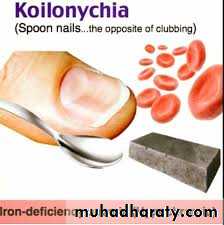
• Koilonychia (iron deficiency)
• Eyes
• Sunken eyes
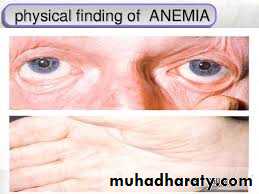
• Pallor
• Jaundice
• Bitotspots
• Affect
• Fatigue
• Depression Dementia
Mouth Pallor
Angular stomatitis (↓B12, folate, iron)Glossitis (↓B12, folate, iron)
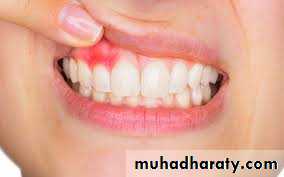
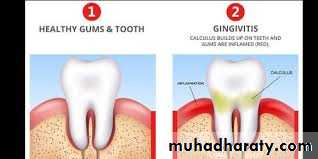
Gingivitis, bleeding gums (↓vitamin C) Poorly fitting dentures
Skin
Dry, flaky skin or dermatitis
Hair loss
Specific abnormalities: Petechiae, corkscrew hairs (↓vitamin C) Dermatitis of pellegra (↓niacin)
Legs
Pitting oedema Ulcers
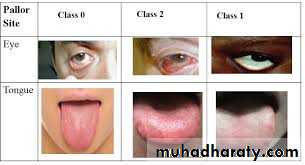







Glossitis can mean soreness of the tongue, or more usually inflammation with depapillation of the dorsal surface of the tongue (loss of the lingual papillae), leaving a smooth and erythematous (reddened) surface, (sometimes specifically termed atrophic glossitis)






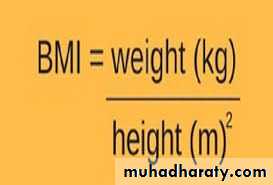
Body mass index (BMI)
BMI=wt(kg)/ ht (m)²
Example: an adult of 70 kg with a height of 1.75 m has a BMI of 70/(1.75)² = 22.9 kg/m²
• BMI is a useful way of identifying under- or over-nutrition but cannot discriminate between lean body or muscle mass and fat mass
• Fat mass is also subject to ethnic variation; for the same BMI, Asians tend to have more body fat than Europeans
• If height cannot be determined (e.g. in older people or those unable to stand), measurement of the femoral length or ‘knee height’ is a good surrogate



How do Screening hospitalised patients for risk of malnutrition ????
Physiology of nutrition
Nutrients in the diet can be classified into:-Macronutrients which are eaten in relatively large amounts to provide fuel for energy,
Micronutrients’ (e.g. vitamins and minerals), which do not contribute to energy balance but are required in small amounts because they are not synthesised in the body.
Energy balance is achieved when energy intake = energy expenditure
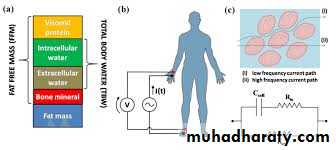
Determinants of energy balance.The basal metabolic rate (BMR) is the obligatory energy expenditure required to maintain metabolic functions in tissues and hence sustain life. It is most closely predicted by fat-free mass (i.e. total body mass minus fat mass), which is lower in females and older people.
Extra metabolic energy is consumed during:-
• Growth
• Pregnancy
• Lactation
• Fever
• Thermal regulation (cold or hot environments)
The energy required for digestion of food (diet-induced thermogenesis) accounts for approximately 10% of total energy expenditure, with protein requiring more energy than other macronutrients.
Another component of energy expenditure is governed by the level of muscular activity, which can vary considerably with occupation and lifestyle.
Energy intake is determined by the ‘macronutrient’ content of food. Carbohydrates, fat, protein and alcohol provide fuel for oxidation in the mitochondria to generate energy (as adenosine triphosphate (ATP) The energy provided by each of these elements differs: • carbohydrates (16 kJ/g) • fat (37 kJ/g) • protein (17 kJ/g) • alcohol (29 kJ/g).
Regulation of energy balance
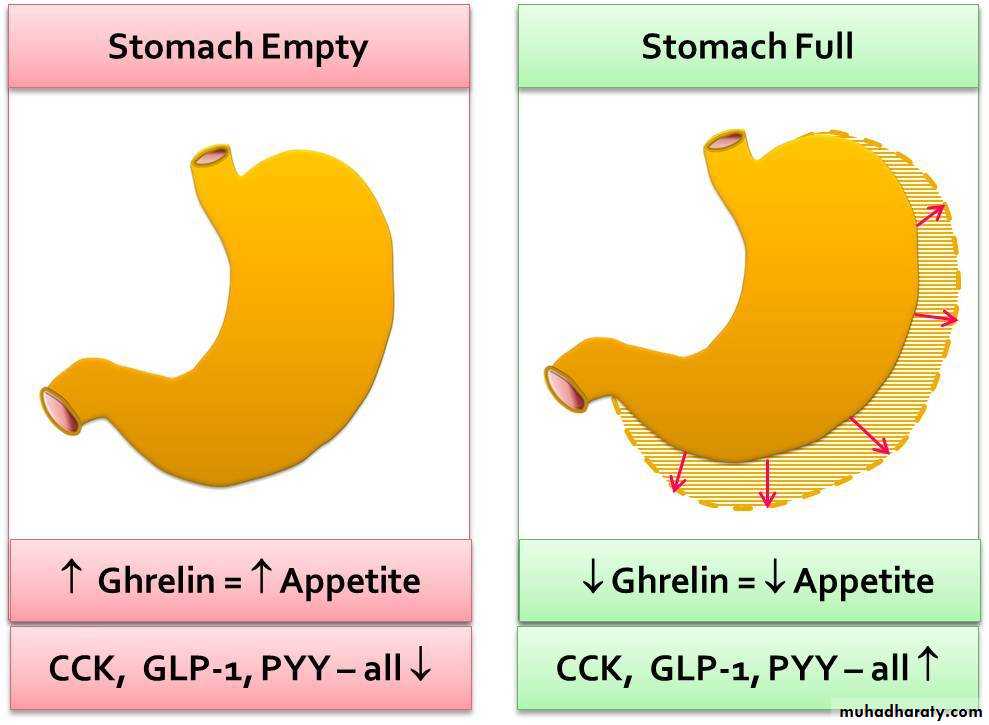
Regulation of energy balance is coordinated in the hypothalamus, which receives afferent signals that indicate nutritional status in theshort term (e.g. the stomach hormone ghrelin, which falls immediately after eating and rises gradually thereafter, to suppress satiety and signal that it is time for the next meal) and the long term (e.g. the adipose hormone leptin, which increases with growing fat mass and may also link fat mass to reproductive function).
The hypothalamus responds with changes in many local neurotransmitters that alter activity in a number of pathways that influence energy balance including hormones acting on the pituitary gland, and neural control circuits that connect with the cerebral cortex and autonomic nervous system.
Regulation of energy balance and its link with reproduction.
+ indicates factors that are stimulated by eating and induce satiety.- indicates factors that are suppressed by eating and inhibit satiety.
Starvation
Reproductive function is suppressedBMR is reduced
Psychological effects, including energy conservation through lethargy.
Responses to under- and over-nutrition
In the low-insulin state of starvation, however, fuels are liberated from stores initially in glycogen (in liver and muscle), then in triglyceride (lipolysis in adipose tissue, with excess free fatty acid supply to the liver leading to ketosis) and finally in protein (proteolysis in muscle).These adjustments can ‘defend’ body weight within certain limits. In those with a high glucose requirement, such as neonates and women who are pregnant or breastfeeding, starvation can result in ketoacidosis associated with normal or low blood glucose.
In response to
over-nutritionBMR is increased
Extra energy is consumed in the work of carrying increased fat stores
so that body weight is again ‘defended’ within certain limits.
In the high-insulin state of over-nutrition, excess energy is invested in fatty acids and stored as triglycerides; these are deposited principally in adipose tissue but they may also accumulate in the liver (non-alcoholic fatty liver disease and skeletal muscle.
If hypothalamic function is abnormal loss of response to satiety signals, together with loss of adaptive changes in energy expenditure, result in relentless weight gain.
Macronutrients (energy-yielding nutrients)
Carbohydrates Fats ProteinsCarbohydrates
The ‘available’ carbohydrates (starches and sugars) are broken down to monosaccharides before absorption from the gut and supply over half the energy in a normal, well-balanced diet . No individual carbohydrate is an essential nutrient, as carbohydrates can be synthesised de novo from glycerol or protein. If the available carbohydrate intake is less than 100 g per day, however, increased lipolysis leads to ketosisDietary guidelines do not restrict the intake of intrinsic sugars in fruit and vegetables or the sugars in milk.
However, intake of non-milk extrinsic sugars (sucrose, maltose, fructose), which increase the risk of dental caries and diabetes mellitus, should be limited.
Individuals who do not produce lactase (‘lactose intolerant’) are advised to avoid or limit dairy products and foods with added lactose.
Starches in cereal foods, root foods and legumes provide the largest proportion of energy in most diets around the world. All starches are polymers of glucose, linked by the same 1–4 glycosidic linkages. Some starches are digested promptly by salivary and then pancreatic amylase, however, producing rapid delivery of glucose to the blood. Other starches are digested more slowly, either because they are protected in the structure of the food, or because of their crystal structure, or because the molecule is unbranched (amylose).
These differences are the basis for the ‘glycaemic index’ of foods.
This is the area under the curve of the rise in blood glucose concentration in the 2 hours following ingestion of 50 g CHO, expressed as a percentage of the response to 50 g anhydrous glucose.
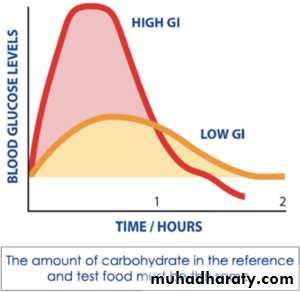
There is evidence linking high glycaemic index foods, particularly foods containing large amounts of sugars such as glucose, sucrose or fructose (e.g. in soft drinks) with obesity and type 2 diabetes
Obesity
T2DM
Sugar alcohols (e.g. sorbitol) that are not absorbed form the gut and are used as replacement sweeteners can cause diarrhoea if eaten in large amounts.
Dietary fibre
Dietary fibre is plant food that is not digested by human enzymes in the gastrointestinal tract. Most dietary fibre is known as ‘non-starch polysaccharides’ (NSPs). A small percentage of ‘resistant’ dietary starch may also pass unchanged into the large intestine. Dietary fibre can be broken down by the resident bacteria in the colon to produce short-chain fatty acids. This is essential fuel for the enterocytes and contributes to bowel health. The extent of flatus formed is dependent on the food source.Some types of NSP, notably the hemicellulose of wheat, increase the water-holding capacity of colonic contents and the bulk of faeces. They relieve simple constipation, appear to prevent diverticulosis and may reduce the risk of cancer of the colon.
Other viscous, indigestible polysaccharides like pectin and guar gum are important in the upper gastrointestinal tract, where they slow gastric emptying, contribute to satiety, and reduce bile salt absorption and hence plasma cholesterol concentration.
Essential fuel for the enterocytes and contributes to bowel health.
Bulk of faeces
Slow gastric emptying, contribute to satiety.

Fats
Fat has the highest energy density of the macronutrients (37 kJ/g) and excessive consumption may be an insidious cause of obesity.Free fatty acids are absorbed in chylomicrons, allowing access of complex molecules into the circulation.
The principal polyunsaturated fatty acid (PUFA) in plant seed oils is linoleic acid (18 : 2 ω6). This and α-linolenic acid (18 : 3 ω3) are the ‘essential’ fatty acids, which humans cannot synthesise de novo.
They undergo further desaturation and elongation, to produce, for example, γ-linolenic acid (18 : 3 ω6) and arachidonic acid (20 : 4 ω6).
These are precursors of prostaglandins and eicosanoids, and form part of the structure of lipid membranes in all cells..
Fish oils are rich in ω3 PUFA (e.g. eicosapentaenoic (20 : 5 ω3) and docosahexaenoic (22 : 6 ω3), which promote the anti-inflammatory cascade of prostaglandin production and occur in the lipids of the human brain and retina.
They inhibit thrombosis by competitively antagonising thromboxane A2 formation
Replacing saturated fat (i.e. from animal sources: butter, ghee or lard) with PUFA in the diet can lower the concentration of circulating low-density lipoprotein (LDL) cholesterol and may help prevent coronary heart disease. High intakes of trans fatty acids (TFAs; isomers of the natural cis fatty acids) reflect the use of oils that have been partially hydrogenated in the food industry.
It is recommended that TFAs are limited to less than 2% of the dietary fat intake, as they are associated with cardiovascular disease.
Cholesterol is also absorbed directly from food in chylomicrons and is an important substrate for steroid and sterol synthesis, but not an important source of energy.
Proteins
Proteins are made up of some 20 different amino acids, of which nine are ‘essential’, (cannot be synthesised in humans but are required for synthesis of important proteins).Another group of five amino acids are termed ‘conditionally essential’, meaning that they can be synthesised from other amino acids, provided there is an adequate dietary supply.
The remaining amino acids can be synthesised in the body by transamination, provided there is a sufficient supply of amino groups.
The nutritive or ‘biological’ value of different proteins depends on the relative proportions of essential amino acids they contain.
Proteins of animal origin, particularly from eggs, milk and meat, are generally of higher biological value than proteins of vegetable origin, which are low in one or more of the essential amino acids.
When two different vegetable proteins are eaten together (e.g. a cereal and a legume), however, their amino acid contents are complementary and produce an adequate mix, an important principle in vegan diets.
Dietary recommendations for macronutrients
Recommendations for energy intake have been calculated to:-• Provide a balance of essential nutrients
• Minimise the risks of excessive refined sugar (dental caries, high glycaemic index/diabetes mellitus), saturated fat or trans fat (obesity, coronary heart disease).
• Recommended dietary fibre intake is based on avoiding risks of colonic disease.
• The usual recommended protein intake for a healthy man doing light work is 65–100 g/day.The minimum requirement is around 40 g of protein with a high proportion of essential amino acids or a high biological value.