Pontics
UNIVERSITY OF MOSULCOLLEGE OF DENTISTRY
By:
Prof. Nawal Atiya Al-Sabawi
2020-2021
Department ofConservative Dentistry
5th. YEAR
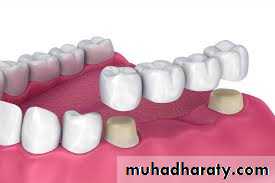
• Pontics: are the artificial teeth of a fixed partial denture that replace missing natural teeth, restoring function and appearance.
• Before determining optimal pontic design the following points should be considered:
• The edentulous areas where a fixed prosthesis is to be provided may be overlooked during the treatment planning phase. Properpreparation includes a careful analysis of the critical dimensions of the edentulous areas: mesiodistal width, occlusocervical distance, buccolingual diameter, and location of the residual ridge.
• To design a pontic that will meet hygienic requirements and prevent irritation of the residual ridge, particular attention must be given to the form and shape of the gingival surface.
• Pontic design must incorporate mechanical principles for strength and longevity as well as esthetic principles for satisfactory appearance of the replacement teeth.
PRETREATMENT ASSESSMENT
PONTIC SPACEOne function of an FPD is to prevent tilting or drifting of the adjacent teeth into the edentulous space. If such movement has already occurred, the space available for the pontic may be reduced and its fabrication complicated. At this point, creating an acceptable appearance without orthodontic repositioning of the abutment teeth is often impossible, particularly if esthetics is important. (Modification of abutments with complete-coverage retainers is sometimes feasible.) Even with a lesser esthetic requirement, as for posterior teeth, overly small pontics are unacceptable because they trap food and are difficult to clean. When orthodontic repositioning is not possible, increasing the proximal contours of adjacent teeth may be better than making an FPD with undersized pontics.
• PRETREATMENT ASSESSMENT
•RESIDUAL RIDGE CONTOUR
The edentulous ridge's contour should be carefully evaluated during the treatment planning phase:An ideally shaped ridge has a smooth, regular surface of attached gingiva, which facilitates maintenance of a plaque-free environment.
Its height and width should allow placement of a pontic that appears to emerge from the ridge and mimics the appearance of the neighboring teeth.
Facially, it must be free of frenum attachment and of adequate facial height to sustain the
appearance of interdental papillae.
Loss of residual ridge contour may lead to:
unesthetic open gingival embrasures ("black triangles")
food impaction
percolation of saliva during speech.
Siebert has classified residual ridge deformities into three categories
Class I defects-faciolingual loss of tissue width with normal ridge height
Class II defects-loss of ridge height with normal ridge width
Class III defects-a combination of loss in both dimensions
PRETREATMENT ASSESSMENT
SURGICAL MODIFICATIONAlthough residual ridge width may be augmented with hard tissue grafts, this is usually not indicated unless the edentulous site is to receive an implant.
Class I defects treatment:
The roll technique for soft tissue ridge augmentation.
The pouch technique for soft tissue ridge augmentation.
Class I I and III defects treatments:
An interpositional graft for augmentation of ridge width and height.
An onlay graft for augmentation of ridge width and height.
Roll technique
Pouch TechniqueInterpositional graft
Onlay graft

• PRETREATMENT ASSESSMENT
• GINGIVAL ARCHITECTURE PRESERVATION• Although the degree of residual ridge resorption following tooth extraction is unpredictable, resulting deformities are not an inevitable occurrence.
• Preservation of the alveolar process can be achieved through:
• immediate restorative (socket preservation techniques) and periodontal intervention at the time of tooth removal.
• By conditioning the extraction site and providing a matrix for healing, the pre-extraction gingival architecture (or "socket") can be preserved. If bone levels are compromised before or during extraction, the sockets can be grafted with an allograft material (hydroxyapatite, tricalcium phosphate, or freeze-dried bone).
•
• PRETREATMENT ASSESSMENT
Socket-preservation techniques:• A provisional FPD can be fabricated indirectly.
• Preparing the abutment teeth before the extraction.
• Extraction of the teeth or tooth.
• Immediate insertion of provisional FPD (The tissue-side of the pontic should be an ovate. it should extend approximately 2.5 mm apical to the facial free gingival margin of the extraction socket. The contour of the ovate tissue side must conform to within 1 mm of the interproximal and facial bone contour)
• After approximately 1 month of healing, oral hygiene access is improved by recontouring the pontic to provide 1 to 1.5 mm of relief from the tissue.
• When the gingival levels are stable (approximately 6 to 12 months), the final restoration can be fabricated.
•
Socket-preservation techniques
• UNIVERSITY OF MOSUL
• COLLEGE OF DENTISTRY• 020-2021
• Pontic Design Classification
No Mucosal Contact
Sanitary (Hygienic)Modified sanitary (Modified Hygienic)
Mucosal Contact
Ridge-lap (Saddle)
Modified ridge-lap (Modified Saddle)
Conical
Ovate
No Mucosal Contact
SANITARY OR HYGIENIC PONTIC: its tissue surface remains clear of the residual ridges.Advantage:
This hygienic design permits easier plaque control.
Disadvantage:
Poor esthetics
Indications:
None esthetic zone
Impaired oral hygiene
Contra indications:
Where esthetic is important
Minimal vertical dimension
Recommended location:
Posterior mandible
•

• No Mucosal contact
A MODIFIED SANITARY PONTIC:Its gingival portion is shaped like an archway between the retainers. This geometry permits increased connector size while decreasing the stress concentrated in the pontic and connectors.“It is also less susceptible to tissue proliferation that can occur when a pontic is too close to the residual ridge.
•
• Mucosal Contact
SADDLE OR RIDGE LAP PONTICThe saddle pontic has a concave fitting surface that overlaps the residual ridge buccolingually,
simulating the contours and emergence profile of the missing tooth on both sides
of the residual ridge.
Advantage:
Esthetics
Disadvantages:
the concave gingival surface of the pontic is not accessible to cleaning with dental floss, which will lead to plaque accumulation.
Tissue inflammation
Indication:
Not recommended
Contra indication:
Not recommended
Recommended location:
Not recommended
•
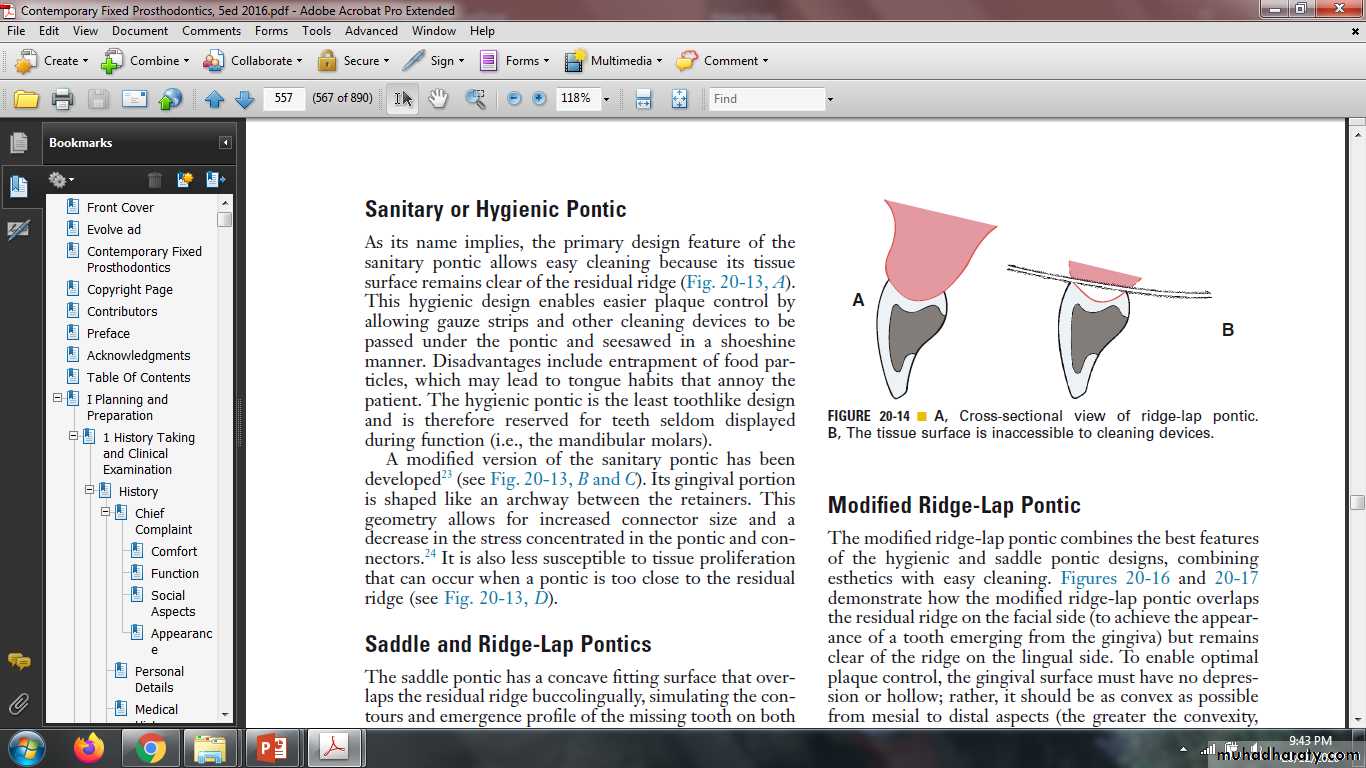
MODIFIED RIDGE LAP PONTIC (Modified saddle)
It combines the best features of the hygienic and saddle pontic designs, combining esthetics with easycleaning. This design overlaps the residual ridge on the facial (to achieve the appearance of a tooth
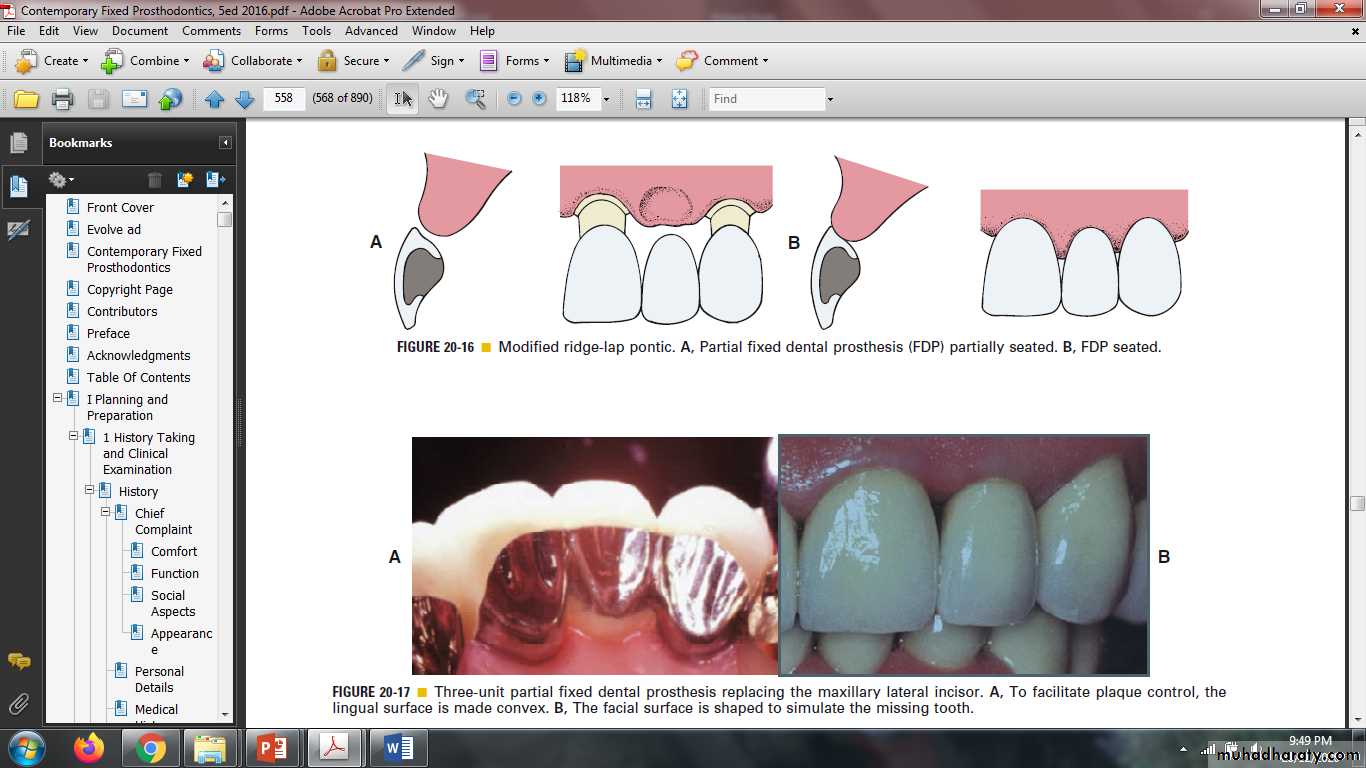
emerging from the gingiva) but remains clear of the ridge on the lingual. Tissue contact should resemble a letter T whose vertical arm ends at the crest of the ridge.
The gingival surface should be as convex as possible from mesial to distal (the greater the convexity, the easier the oral hygiene).
•
• Mucosal Contact
MODIFIED RIDGE LAP PONTIC
• Advantage:• Good esthetics.
• Disadvantage:
• Moderately easy to clean.
• Indication:
• Most areas with esthetic concern.
• Contra indication:
• Where minimal esthetic concern exists.
• Recommended location:
• High esthetic requirement (anterior teeth and premolar, some maxillary molar)
• Materials:
• Metal-ceramic
• All- resin
• Mucosal Contact
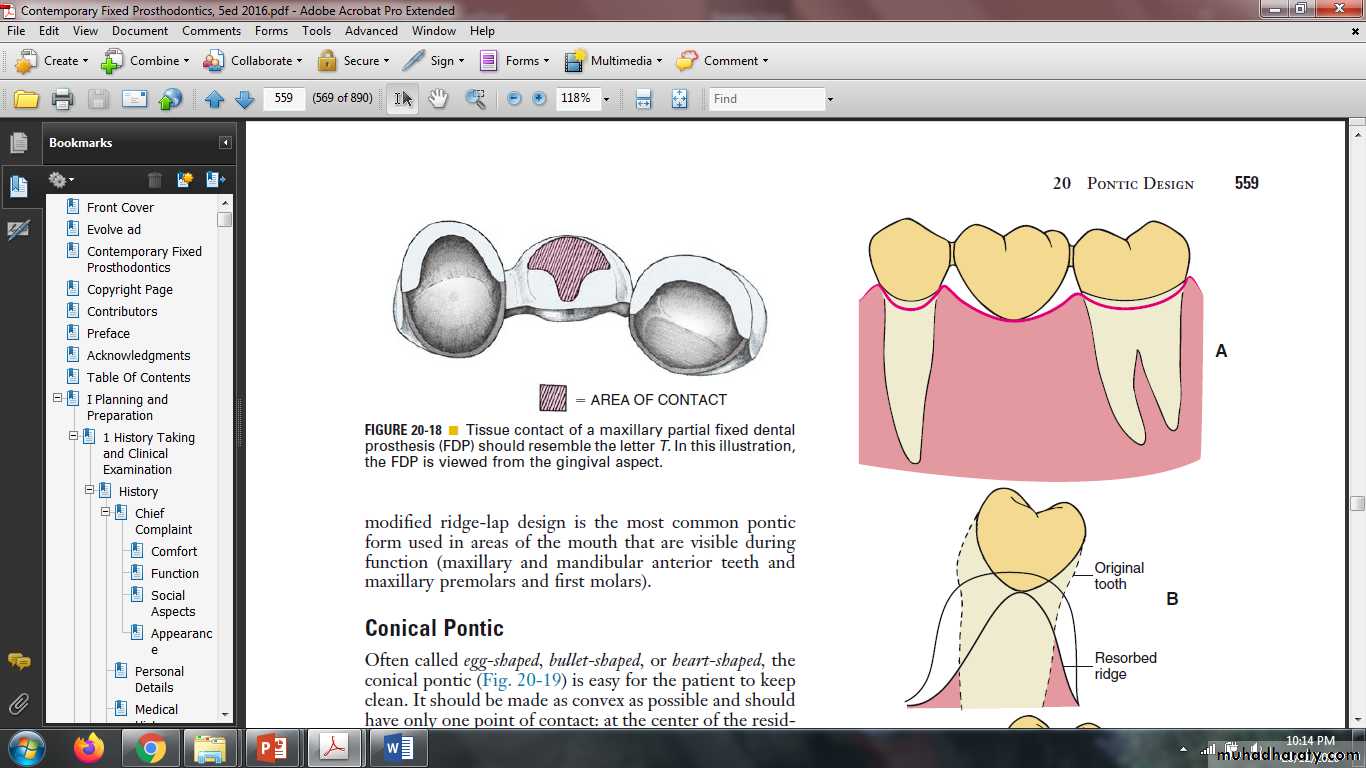
CONICAL PONTIC
Often called egg-shaped, bullet-shaped, or heart-shaped . It made with only one point of contact at the center of the residual ridge, it should be made as convex as possible.Advantage:
moderate access for oral hygiene.
Disadvantage:
Poor esthetic.
Indication:
Posterior areas where esthetic is of minimal concern.
Contra indication :
Poor oral hygiene.
Recommended location:
Molar without esthetic requirements.
Materials: All-metal
All- resin
Metal -ceramic
• Mucosal Contact
OVATE PONTIC
The ovate pontic is the most esthetically appealing pontic design. Its convex tissue surface resides in asoft tissue depression or hollow in the residual ridge, which makes it appear that a tooth is literally emerging from the gingiva.Advantages:
Superior esthetic.
Negligible food entrapment.
Ease of clean.
Disadvantage:
Require surgical preparation.
Indication:
Desire for optimal esthetic.
High smile line.
Contra indication:
Un willingness for surgery.
Recommended location:
Maxillary incisors
Cuspids and premolar.
Materials:
All- resin
Metal-ceramic
• Mucosal Contact
BIOLOGIC CONSIDERATIONS
The biologic principles of pontic design pertain to the maintenance and preservation of the residualridge, abutment and opposing teeth, and supporting tissues.
Factors of specific influence are:
Pontic ridge contact.
Oral hygiene considerations
Pontic material.
The direction of occlusal forces.
PONTICRIDGE CONTACT
Pressure-free contact between the pontic and the underlying tissues is indicated to prevent ulceration
and inflammation of the soft tissues.
ORAL HYGIENE CONSIDERATIONS:
Unlike removable partial dentures, FPDs cannot be taken out of the mouth for daily cleaning. Patients must be taught efficient oral hygiene techniques, with particular emphasis on cleaning the gingival surface of the pontic. The shape of the gingival surface, its relation to the ridge, and the materials used in its fabrication will influence ultimate success.
PONTIC MATERIAL
Any material chosen to fabricate the pontic should provide good esthetic results where needed; biocompatibility, rigidity, and strength to withstand occlusal forces; and longevity.FPDs should be made as rigid as possible, because any flexure during mastication or parafunction may cause pressure on the gingiva and cause fractures of the veneering material. Occlusal contacts should not fall on the junction between metal and porcelain during centric or eccentric tooth contacts, nor should a metalceramic junction occur in contact with the residual ridge on the gingival surface of the pontic.
For easier plaque removal and biocompatibility, the tissue surface of the pontic should be made in glazed porcelain. However, ceramic tissue contact may be contraindicated in edentulous areas where there is minimal distance between the residual ridge and the occlusal table. In these instances, placing ceramic on the tissue side of the pontic may weaken the design of the metal substructure, particularly with porcelain occlusal surface. If gold is placed in tissue contact, it should be highly polished.
OCCLUSAL FORCES:
In fact, narrowing the occlusal table may actually lead to:
Impede or even preclude the development of a harmonious and stable occlusal relationship. Like a malposed tooth.
It may cause difficulties in plaque control.
May not provide proper cheek support.
For these reasons, pontics with normal occlusal widths (at least on the occlusal third) are generally recommended. One exception is if the residual alveolar ridge has collapsed buccolingually. Reducing pontic width may then be desired, thereby lessening the lingual contour and facilitating plaque-control measures.
Mechanical problems may be caused by improper choice of materials, poor framework design, poor tooth preparation, or poor occlusion. These factors can lead to fracture of the prosthesis or displacement of the retainers. Long-span posterior FPDs are particularly susceptible to mechanical problems.
Therefore, evaluating the likely forces on a pontic and designing accordingly are important. For example, a strong all-metal pontic may be needed in high-stress situations rather than a metal-ceramic pontic, which would be more susceptible to fracture. When metalceramic pontics are chosen, extending porcelain onto the occlusal surfaces to achieve better esthetics should also be carefully evaluated. In addition to its potential for fracture, porcelain may abrade the opposing dentition if the occlusal contacts are on enamel or metal.

MECHANICAL CONSIDERATIONS
THE GINGIVAL INTERFACEAn esthetically successful pontic will replicate the form, contours, incisal edge, gingival and incisal embrasures, and color of adjacent teeth. The pontic's simulation of a natural tooth is most often betrayed at the tissue-pontic interface. The recommendation of each type of pontic is describe before.
INCISOGINGIVAL LENGTH
Obtaining a correctly sized pontic simply by duplicating the original tooth is not possible. Ridge resorption will make such a tooth look too long in the cervical region. The height of a tooth is immediately obvious when the patient smiles and shows the gingival margin.
One solution is to shape the pontic to simulate a normal crown and root with emphasis on the cementoenamel junction. The root can be stained to simulate exposed dentin. Another approach is to use pink porcelain to simulate the gingival tissues.

ESTHETIC CONSIDERATIONS
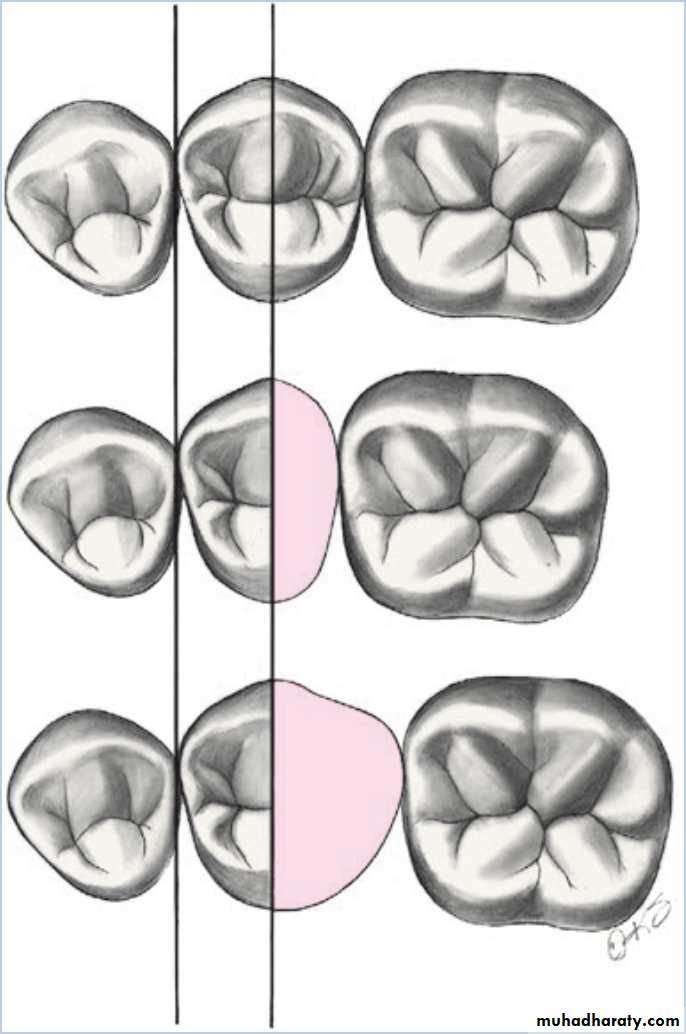
MESIODISTAL WIDTH
Frequently, the space available for a pontic will be greater or smaller than the width of the contralateral tooth. This is usually due to uncontrolled tooth movement that occurred when a tooth was removed and not replaced.Treatment of space discrepancy:
discrepancy should be corrected by orthodontic treatment
the space discrepancy can be compensated by altering the shape of the proximal areas.
A discrepancy in the posterior teeth can be managed by duplicating the visible mesial half of the tooth and adjusting the size of the distal half.
The retainers and the pontics can be proportioned to minimize the discrepancy.
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRY
Thank You
2020-2021