Dr.Methaq A.M. Hussein
MRCP (LONDON),,SCE endocrine(london),F.I.B.M.SASSIST. Professor
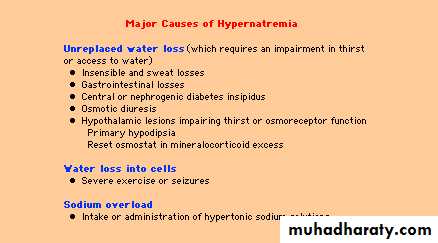
Sodium Disorders Hypernatremia
symptoms of hypernatremia
tend to be nonspecific. Anorexia, restlessness, nausea, and vomiting occur early. These symptoms are followed by altered mental status, lethargy or irritability, and, eventually, stupor or coma. Musculoskeletal symptoms may include twitching, hyperreflexia, ataxia, or tremoracute hypernatremia as a complication often results in significant brain shrinkage, thus causing mechanical traction of cerebral vasculature. Stretching of bridging veins can result in subdural hemorrhages. Venous congestion can lead to thrombosis of the intracranial venous sinuses
Background
Hypernatraemia is classified as:Mild (146-149 mmol/L)
Moderate (150-169 mmol/L)
Severe (≥170 mmol/L)
Moderate to severe hypernatraemia can cause acute brain shrinkage with vascular rupture, haemorrhage, demyelination and permanent neurological injuryInfants and small children are more vulnerable to hypernatraemia due to greater insensible losses and inability to communicate their need for fluids or access fluids independently Chronic hypernatraemia (>48 hours) is often well tolerated and asymptomatic due to cerebral compensation
Key points Start treatment early with IV sodium chloride with 5% GW?? The rate of correction should not exceed 0.5 mmol/L/hr, ie 10-12 mmol/L per day, to avoid cerebral oedema, seizures and permanent neurological injury
The sole indication for administering isotonic saline to a patient with hypernatremia??????????????? is a depletion of extracellular-fluid volume that is sufficient to cause substantial hemodynamic compromise. Even in this case, after a limited amount of isotonic saline has been administered to stabilize the patient's circulatory status, a hypotonic fluid (i.e., 0.2 percent or 0.45 percent sodium chloride) should be substituted in order to restore normal hemodynamic values while correcting the hypernatremia
Extreme care must be taken to avoid excessively rapid correction or overcorrection of hypernatremia, which increases the risk of iatrogenic cerebral edema, with possibly catastrophic consequences.
. Water deficit The water deficit in the hypernatremic patient can be estimated from the following formula.
C BW refers to estimated current body water. The total body water is normally about 60 and 50 percent of lean body weight in younger men and women, respectively, and is somewhat lower in the elderly (about 50 and 45 percent in men and women, respectively. However, it is probably reasonable to use values about 10 percent lower (50 and 40 percent) in hypernatremic patients who are water-depleted. Thus, in a 60 kg woman with a plasma sodium concentration of 168 mEq/L, total body water is about 40 percent of body weight and the water deficit can be approximated from :
Water deficit=0.4×60 ([168/140]-1) = 4.8 liters

treatment of moderate hypernatraemia due to water deficit Total fluid requirement = maintenance + replacement of deficit + replacement of ongoing losses
Replace water deficit over 48 hours in addition to daily maintenance, with IV sodium chloride 0.9% and glucose 5% In addition, replace ongoing losses mL for mL (excluding urine) with IV sodium chloride 0.9% Once urine output is established, add potassium to the IV fluid inputIf seizures occur:consider venous sinus thrombosis or cerebral infarctionconsider imaging with a contrast CT scancontact ICU -
Severe hypernatraemia requires correction over several days, at a slower rate
Diabetes InsipidusDdx
Diabetes Mellitus
Hypercalcemia
Solute diuresis:
Volume expansion 2° saline loading
High-protein feeds (urea as osmotic agent)
Post-obstructive diuresis
Diabetes Insipidus:
Central (CDI)
Nephrogenic (NDI)
Primary (Psychogenic) Polydipsia
Polyuria: > 3 L/d + Polydipsia: > 3.5 L/d