Human Immunodeficiency Virus (HIV)
م.د. انتظار علاوي جعفر / فرع الاحياء المجهريه / كليه الطب / جامعه ذي قارPhD. M.Sc. Microbiology
Introduction
• There were approximately 37.9 million people living with HIV at the end of 2018.• However, with increasing access to effective HIV prevention, diagnosis, treatment and care, including for opportunistic infections, HIV infection has become a manageable chronic health condition, enabling people living with HIV to lead long and healthy lives.
• Due to gaps in HIV services, 770 000 people died from HIV-related causes in 2018 and 1.7 million people were newly infected according to WHO.
As of December 2014, less than 100 people living with HIV
were reported. From 1986 to 2014, a slight increase occurred in officially reported HIV cases, half of which were nationals and half foreigners. The large majority were males, with more thanhalf between 15 and 29 years of age.
Of reported cases, 57% were infected by blood transfusion and blood products, though sexual transmission has become the main reported mode of transmission since 2003.
Origin of AIDS
HIV in humans originated from cross-species infections by simian viruses in rural Africa, probably due to direct human contact with infected primate blood.Classification
Human immunodeficiency virus (HIV) is a a Lentivirus , a sub family of Lentiviridae in the family Retroviridae that causes :
Acquired immunodeficiency syndrome (AIDS).
Morphology
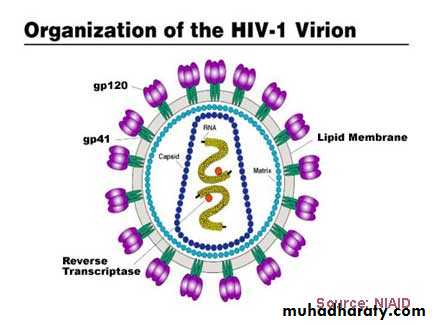
HIV is a spherical, enveloped virus, which measures up to120 nm in diameter (See-Fig). HIV, is an enveloped RNA viruses, possessing an RNA-dependent DNA polymerase called Reverse transcriptase.
It has a unique three-layered structure:
• The innermost genome layer,
• Middle cone shaped nucleocapsid
• An outer membrane of glycoprotein surrounded by lipoprotein envelope.
Viral genome
HIV genome is most complex of human retroviruses.The genome consists of two identical copies of single-stranded positive-sense RNA genome.
The HIV contains three major genes gag , pol , and env , characteristic of all retroviruses.
All these genes encode for the structural proteins.
HIV shows two distinct antigenic types: HIV-1 and HIV-2.
The two types are distinguished on the basis of genome organization and phylogenetic (evolutionary) relationships with other primate lentiviruses. Sequence divergence between HIV-1 and HIV-2 exceeds 50%.
The gag gene encodes for internal capsid and matrix “core” proteins (p15, p18, and p24).
Of these three proteins, p24 is the major antigen, which is demonstrated in serum of HIV patients during the early stage of infection and persists till the appearance of serum antibodies.
Detection of p24 antigen in serum, therefore, is of diagnostic value.
The pol gene encodes for several proteins, including the enzymes reverse transcriptase, integrase, and protease. The reverse transcriptase synthesizes DNA by using the genome RNA as a template.
The integrase integrates the viral DNA into the cellular DNA,
The protease cleaves various viral precursor proteins.
The env gene codes gp160, a precursor glycoprotein that is split to form two envelope glycoproteins, gp120 and gp41, which form the surface spikes and transmembrane tissue proteins, respectively.
tat gene is the most important one, which encodes a protein called Tat protein that facilitates viral gene transcription.
Tat protein along with other HIV-encoded regulatory protein called Nef suppresses the synthesis of class I MHC proteins thereby reducing the ability of cytotoxic T cells to kill the HIV-infected cells.
Nucleocapsid: The viral genome is surrounded by a nucleocapsid consisting of proteins.
Three enzymes are located in the nucleocapsid:(i) Reverse transcriptase.
(ii) Integrase.
(iii) Protease.
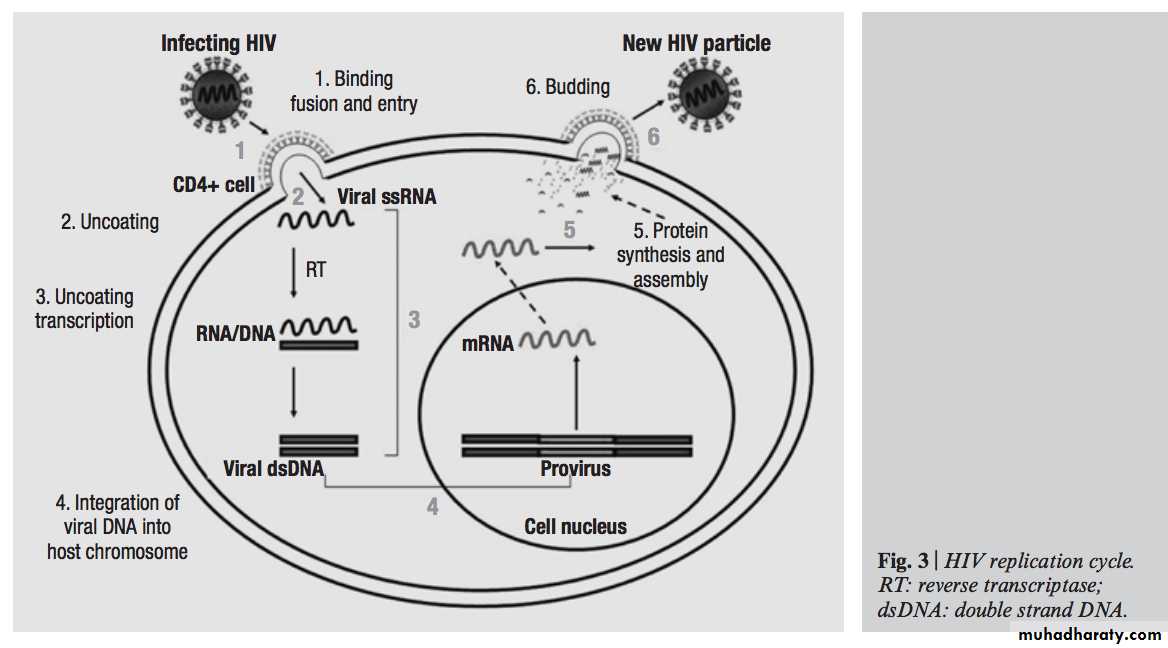
HIV replication cycle
Viral replicationThe virus binds to the CD4 proteins on the cell surface with the help of its gp120 envelope protein (See-Fig).
This protein also interacts with chemokine receptors on the cell surface including the CXCR4 and CCR5, which are essential for entry of HIV into CD4 cells.
Note: Individuals who possess homozygous deletions in CCR5 or produce mutant forms of the protein may be protected from infection by HIV-1; mutations in the CCR5 gene promoter appear to delay disease progression.
• Then gp41 of the virus mediates fusion of the viral envelope with the cell membrane followed by entry of the virus into the cell.
• Once inside the cell, after uncoating, the virion RNA-dependent DNA polymerase transcribes the genome RNA into double-stranded DNA, which subsequently integrates with the host cell DNA.
• Integration is mediated by the viral enzyme integrase. The host cell RNA polymerase transcribes the viral mRNA from the proviral DNA.
The viral mRNA encodes several proteins, protease to form the main core protein (p24), the matrix protein (p17), and several smaller proteins such as reverse transcriptase, integrase, and protease.
The immature virions are assembled in the cytoplasm, and cleavage by the viral protease occurs as the immature virion buds from the cell membrane, resulting in the production of mature infectious HIV.
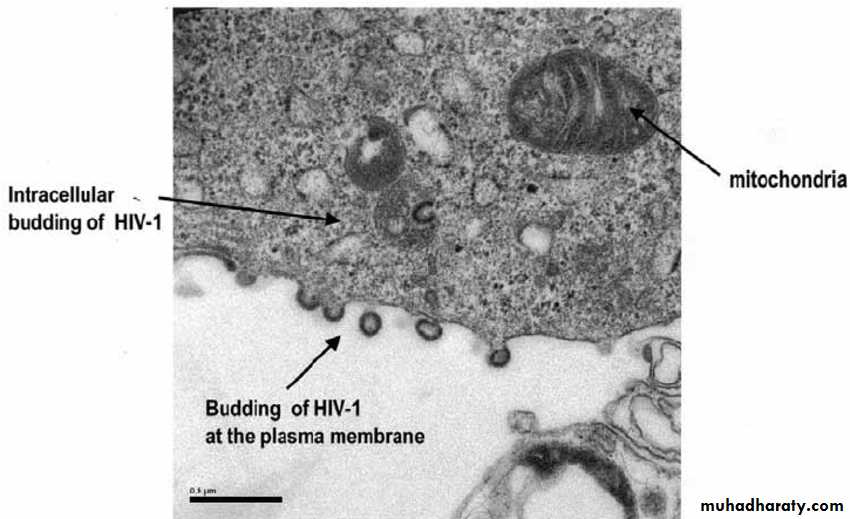
Grigorov, et al. (2005).
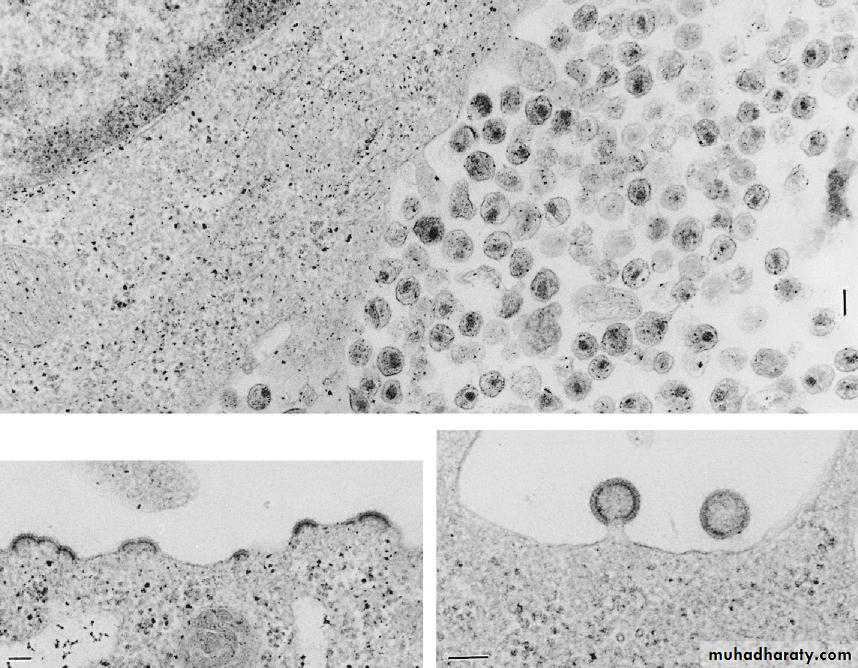
EM of HIV-infected lymphocytes, showing a large accumulation of freshly produced virus at the cell surface.
Jawetz Melnick & Adelbergs Medical Microbiology 2013.
HIV inactivation
HIV is a thermolabile virus.It is readily inactivated at 60°C in 10 minutes and at 100°C in seconds.
HIV is inactivated by treatment with 50% ethanol, 0.5% formaldehyde, 0.3% hydrogen peroxide, and 10% bleaching powder in 10 minutes.
A 2% solution of glutaraldehyde is effective for disinfection of medical instruments.
It is also inactivated at a very low pH (1) and high pH (13).
Pathogenesis and Immunity
• HIV is primarily a sexually transmitted pathogen transmitted by high-risk behaviors, such as unprotected intercourse, male homosexual intercourse, and also by intravenous (IV) drug abuse.• The tropism of the HIV for CD4-expressing T-cells and macrophages is the principal determinant of the pathogenicity of HIV.
Pathogenesis and Immunity
• The CD4 antigens act as receptors for HIV. The virus infects helper T cells and kills them, resulting in HIV-induced immunosuppression, leading to full-blown AIDS-a key feature of the pathogenesis of HIV infection.• This makes the patient most susceptible to opportunistic infections and certain cancerous conditions, such as Kaposi’s sarcoma and lymphoma.
• The virus replicates continuously in the lymph nodes, thereby releasing the virions and infected T cells into the blood.
• During the course of infection, the virus causes a drastic reduction in the number of CD4 T cells, which may occur due to
Direct HIV mediated cytopathic effect,
Virus specific immune response,
Apoptosis induced by viral proteins.
The deficiency or reduction of CD4 T cells leads to depression of cellular immune response and impairment of humeral responses.
The reduction of CD4 T cells leads to opportunistic infections caused by many opportunistic pathogens.
Clinical Syndromes
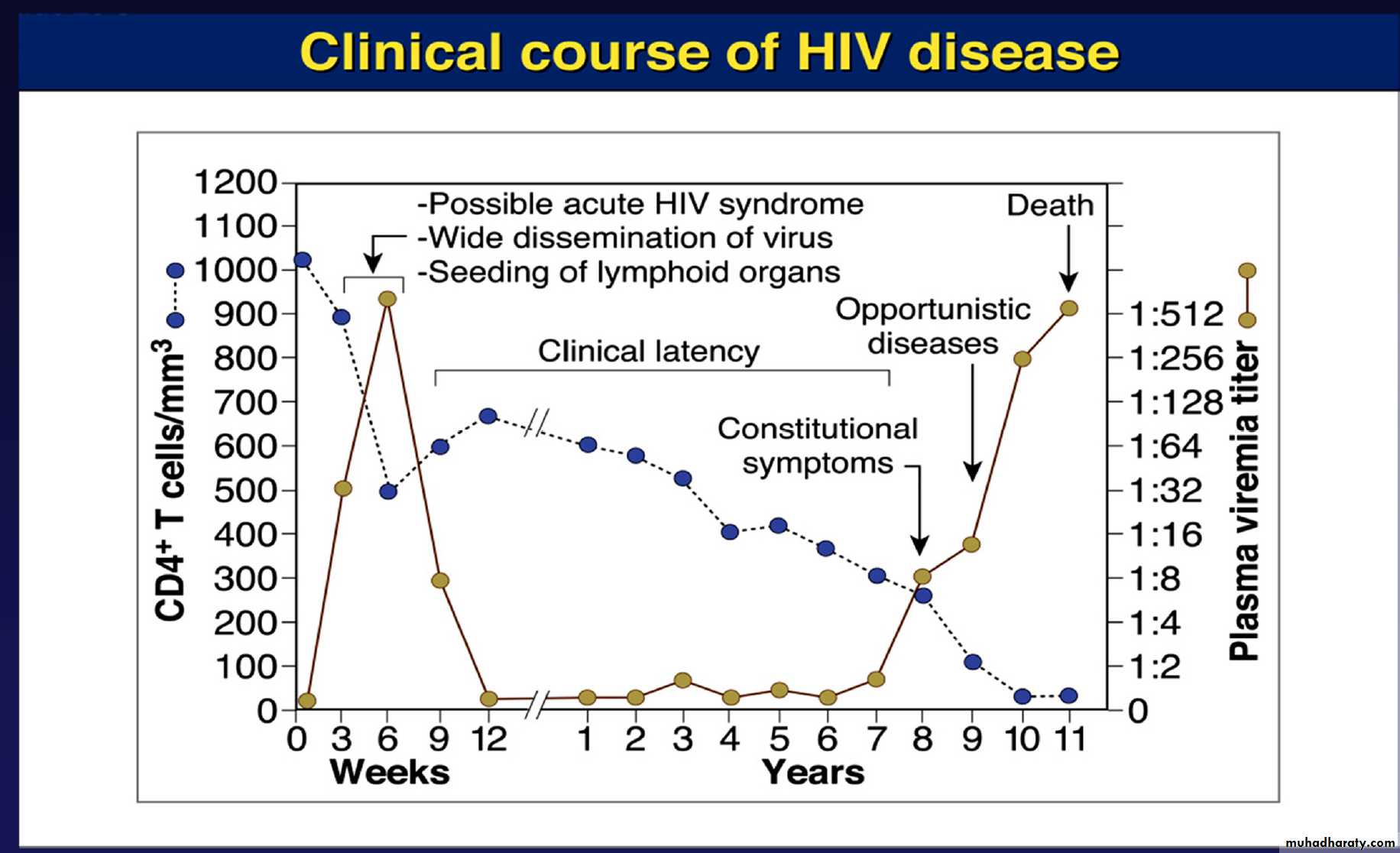
The course of untreated HIV infection is usually 10 years or longer. The disease progresses through the stages of• Primary infection (flu like disease).
• Dissemination of virus to lymphoid organs.
• Clinical latency.
• A late stage of profound immunosuppression known as full-blown Acquired Immune Deficiency Syndrome (AIDS).
Acute HIV infection
Is characterized by rapid rise in plasma viremia associated with drop in CD4 count after an incubation period of 3–6 weeks.The symptoms of HIV are nonspecific and include Low-grade fever, fatigue, malaise,
Rash, headache,
lymphadenopathy;
Spontaneous resolution may occur within weeks.
Asymptomatic HIV infection
In this period, patient continues to remain asymptomatic for several months to years. This stage is characterized by
A low level of viral replication and a gradual fall in CD4 count.
The serum is positive for HIV antibodies in these patients.
Another characteristic of the stage of latency is persistent generalized lymphadenopathy, which may last for several years or a period of asymptomatic infection.
During this stage, virus continues to replicate in the lymph node.
Acquired Immune Deficiency Syndrome (AIDS)
Is characterized by lymphadenopathy and fever. AIDS is the end-stage disease of the HIV infection.It denotes the irreversible breakdown of immune system of the host, making the infected host highly susceptible to a wide range of progressive opportunistic infections
Acquired Immune Deficiency Syndrome (AIDS)
Opportunistic infections such as tuberculosis, Pneumocystis carinii pneumonia, toxoplasmosis, cryptococcal meningitis or unusual malignancies, such as Kaposi’s sarcoma, non- Hodgkin’s lymphoma, Hodgkin’s lymphoma, cervical cancer, and Burkitt’s lymphoma.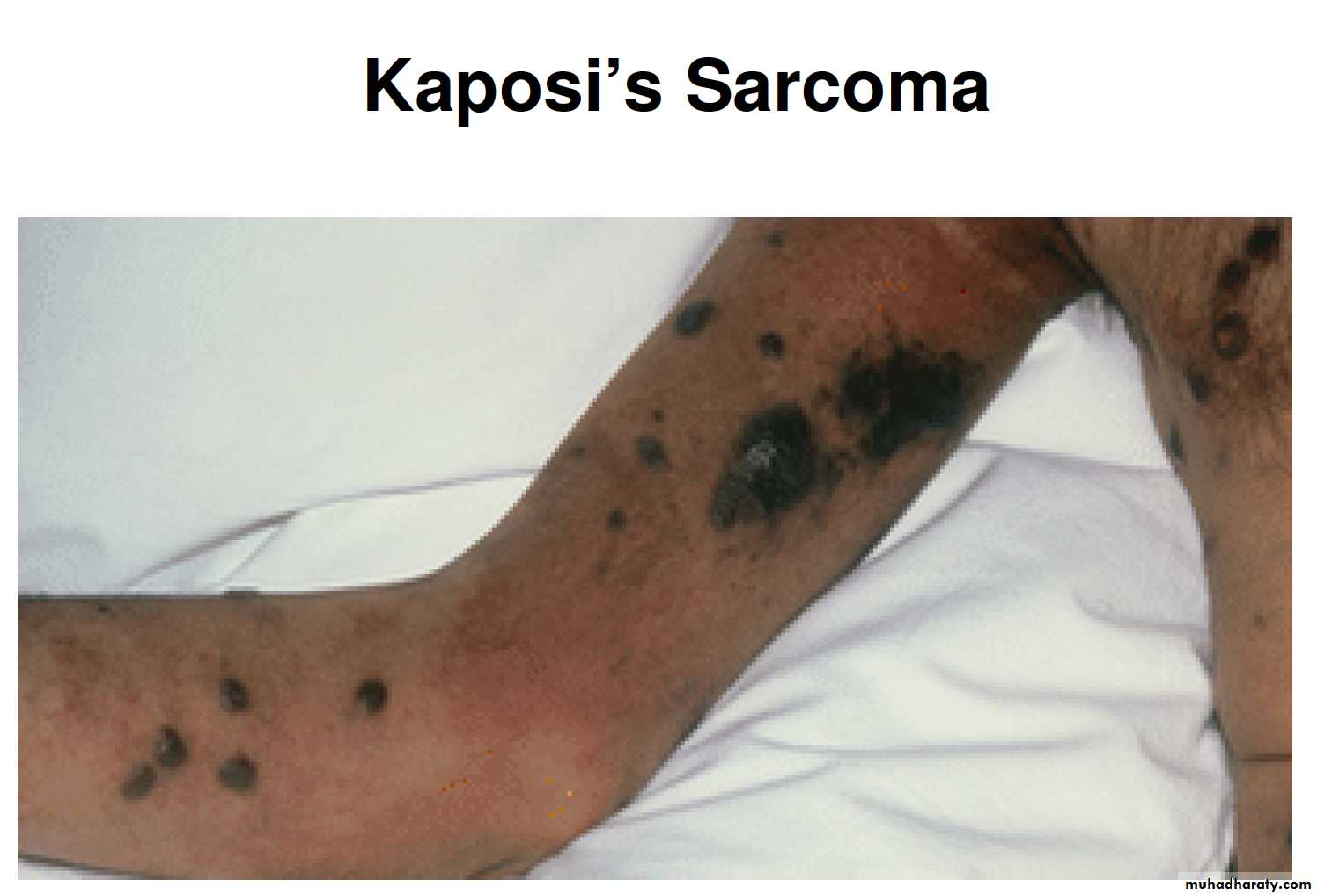

Yarchoan, R., & Uldrick, T. S. (2018). HIV-Associated Cancers and Related Diseases. The New England journal of medicine, 378(11), 1029–1041.
Selected Clinical Manifestations of Kaposi’s Sarcoma
AIDS is characterized by deterioration of immune response as evidenced by CD4 T cell decrease response. The onset of clinical manifestations correlates with:
A reduction in number of CD4 T cells to less than 450/L.
Increased level of virus in the blood.
Presence of p24 antigen in the blood.
HIV transmission occurs in following ways
Sexual transmission.Transmission by blood transfusion.
Parenteral transmission occurs largely among IV drug users through the use of contaminated needles.
Mother-to-child transmission: can occur by vertical transmission through the placenta or through the amniotic membrane or by perinatal transmission during delivery through infected birth canal.
Breast feeding
Transmission of infection
HIV is primarily a human infection. Humans infected with HIV and AIDS are the reservoir of infection.The high titer of HIV is found in the body fluids including blood, semen, and vaginal secretions of the infected people; hence these are important sources of infection.
Laboratory Diagnosis
1-Serodiagnosis:• Detection of specific antibodies to envelope glycoproteins gp41, gp120, and gp160 and to viral core p24 antigens using ELISA assay.
The level of these antibodies is demonstrated in most individuals within 6–12 weeks after infection and in all the individuals within 6 months of infection.
2-Molecular Diagnosis:
The circulating virus count (viral load) is determined by quantitative RT-PCR.
It can also be used to monitor the success of therapy with RT and protease inhibitors.
3-Virus isolation
The vast majority of HIV-1 antibody–positive persons
will have virus that can be cultured from their blood cells.
However, virus isolation techniques are time-consuming and aborious and are limited to research studies.
Monitoring status of HIV infection
1- CD4 T cell count: This is an important indicator for monitoring HIV infection.A rapid decrease in the CD4 count below 500/L in adults and in infants is a poor prognostic sign and requires the initiation or alteration of antiviral therapy.
When the count falls below 200/L, it indicates a very poor prognosis and shows the increased risk for serious infection of patient, particularly opportunistic infections.
2- Measurement of HIV RNA by PCR: HIV RNA level in serum is an important predictive marker of disease progression and are used as prognostic marker to monitor the effectiveness of anti-HIV therapies.
Treatment
The anti-HIV drugs can be broadly classified as:• Nucleoside analoge reverse transcriptase inhibitors (NRTIs) e.g Zidovudine, Didanosine, Zalcitabine and Lamivudine.
(b) Nonnucleoside reverse transcriptase inhibitors (NNRTIs) e.g Nevirapine, Delaviridine, Efavirenz.
(c ) Protease inhibitors e.g Ritonavir and Indinavir.
There is no effective cure for HIV infection. However, effective antiretroviral drugs (ARVs) can control the virus and help prevent onward transmission to other people.
• Therapy with combination of Highly active antiretroviral therapy, referred to as (HAART), is effective in inhibition of HIV replication.
HAART has improved efficacy of the therapy, and delayed emergence of drug resistance.
Treatment
It often can suppress viral replication to below limits of detection in plasma.Decrease viral loads in lymphoid tissues,
Allow the recovery of immune responses to opportunistic pathogens.
Prolong patient survival.
It is usually recommended to initiate double and triple drug therapy with two NRTIs Or two NRTIs an NNRTI or a protease inhibitor.
Treatment
HW!
https://docs.google.com/forms/d/1YTaHeCeqyY3PQvAw6XsnuUt6GDXz8dnUlzIb0lTnhoU/edit?usp=sharing