Pathology of the urinary system
The pathology of the kidneyIntroduction:
Disease of the kidney are divided into four categories depending on which component of the kidney is primarily affected; these are
Glomerular
Tubular
Interstitial
Vascular
This division is useful because:-
The early manifestations of each group of diseases tend to be distinctiveThese groups differ in their pathogenesis for e.g. glomerular disease are often immunologically mediated, whereas tubular and interstitial disorders are more likely to be caused by toxic or infectious agents, however it should be noted that
The interdependence of renal components translated into that damage to one component is almost always affects secondarily the others
All form of chronic renal disease tend ultimately to damage all four components of the kidney thus eventuates in chronic renal failure (end stage kidney disease).
Glomerular diseases:-
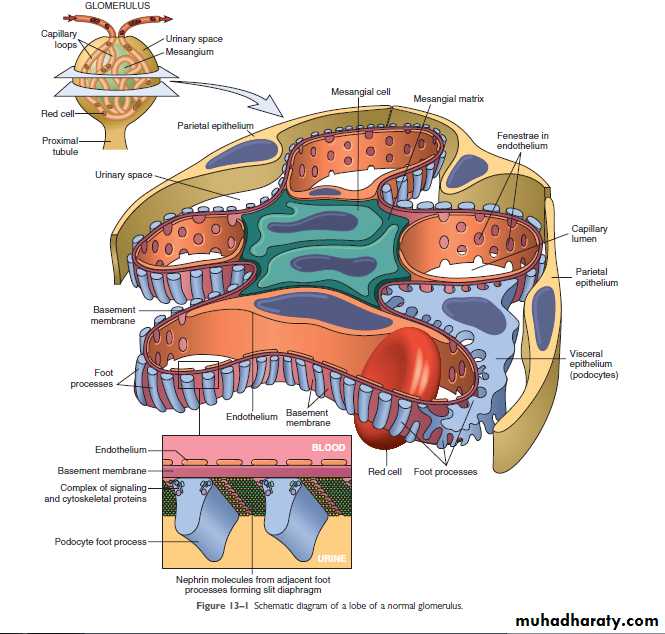
The glomerulus consist of an anastomosing network of capillaries invested by two layers of epithelium; visceral and parietal . the visceral epithelium (podocytes) is an intrinsic part of the capillary wall, whereas the parietal epithelium lines the Bowmans space (urinary space), the cavity in which plasma ultrafiltrate first collects. The glomerular capillary wall is the filtration unite and consists of the following structures:-A thin layer of fenestrated endothelial cells (each hole is about 100 nm in diameter ).
Glomerular basement membrane (GBM), ultrastructurally made up of a thick, dense central layer (lamina densa), and thinner, lucent peripheral layers (lamina rara interna & externa)
The visceral epithelial cells (podocytes) that possess foot processes adherent to the lamina rara externa of the basement membrane. Adjacent foot processes are separated by 25- nm wide filtration slits bridged by a thin slit diaphragm composed in largely of nephrin.
The entire glomerular tuft is supported by mesangial cells lying between the capillaries. Basement membrane- like mechanical matrix forms a meshwork through which the mesangial cells are scattered.
The glomerular basement membrane shows selective permeability, which is size dependent and charge dependent. The major characteristics of glomerular filtration are:
A high permeability to water and small solutes
Almost complete impermeability to molecules of the size and molecular charge of albumin.
More permeability to cation than anions
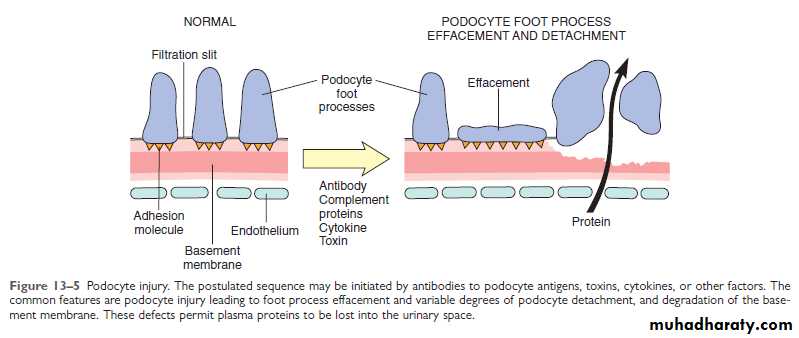
The podocyte is decisive(important) to the glomerular barrier function by providing a distal resistance to the flow of water and a barrier to the filtration of proteins. It is also largely responsible for synthesis of GBM component..
The pathogenesis of the glomerular diseases:-
Immune mechanisms (antibody – associated & cellular) underlie most primary and many secondary glomerular diseases:Circulating immune complex- mediated nephritis (type III hypersensitivity reactions)
With circulating immune complex- mediated disease, the glomerulus is an,, innocent bystander,, because it is not responsible for their formation. The antigen in these complexes may be:
Endogenous as in SLE or
Exogenous as in bacterial (streptococcal), viral (hepatitis B), parasitic (plasmodium falciparum malaria), and spirocheatal ( Treponema Pallidum) infections.
Unknown as often the case in membranous nephropathy.
The antigen- antibody complexes are trapped in the glomeruli, where they produce injury mainly through the activation of complement and the recruitment of the leukocytes. E.M reveals the immune complexes as electron dense granular deposits in the glomerulus.
Mediators of immune injury:-
A major pathway of antibody initiated injury is activation of the complement that lead to generation of chemotactic agents (mainlyC5a) and thus recruitment of the neutrophils and monocytes . neutrophils in turn release.
Proteases, which cause GBM degradation
Oxygen- derived free radicals, which cause cell damage and
Arachidonic acid metabolites, which contribute to reduction in GFR.
In some cases however complement – dependent (but not neutrophil- dependent) injury occurs through the effect of the C5-C9 lytic component (membrane attack complex) of complement which causes
Epithelial cell detachment and
Stimulation of the mesangial and epithelial cells to secrete various mediators of cell injury.
Up- regulation of transforming growth factor-β (TGF- β) receptors on podocytes; TGF-β stimulates synthesis of extracellular matrix, thus giving rise to altered GBM composition and thickening
Nephritis caused by in situ immune complexes:-
Antibodies in this form of injury react directly with planted antigens in the glomerulus:-
The best –characterized disease in this group is anti-GBM antibodies. It results from the formation of autoantibodies directed against the GBM. Deposition of these antibodies creates a linear pattern of staining when visualized by I.F.M . this is in contrast with granular pattern described for other forms of immune complex-mediated nephritis. Sometimes the anti- GBM antibodies cross react with the basement membranes of the lung alveoli, result in combined lung and kidney lesions (Goodpasture syndrome).
Planted antigens also include DNA bacterial products, aggregated IgG which deposit in the mesangium because of their size. Most of these planted Ags induce a granular pattern of immunoglobulin deposition as seen by I.F.M
Cell mediated immune GN:-
T cell- mediated injury may account for some cases of GN in which either there are no deposits of Ab or immune complexes or the deposits do not correlate with the severity of damage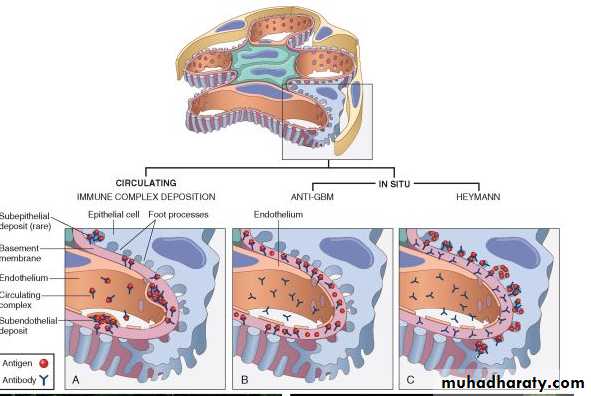
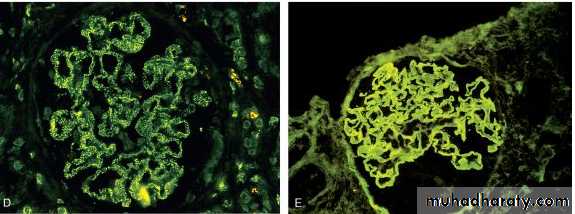
FIGURE 20-4 Antibody-mediated glomerular injury can result either from the deposition of circulating immune complexes (A) or, more commonly, from in situ formation of complexes exemplified by anti-GBM disease (B) or Heymann nephritis (C). D and E, Two patterns of deposition of immune complexes as seen by immunofluorescence microscopy: granular, characteristic of circulating and in situ immune complex nephritis (D), and linear, characteristic of classic anti-GBM disease (E).
The nephrotic syndrome:-
This refers to a clinical complex that is includes:-
Massive proteinuria ( daily protein loss of 3.5 gm or more in adults)
Hypoalbuminemia ( plasma albumin level less than 3 gm)
Generalized edema
Hyperlipidemia and lipiduria
The initial event is the derangement of the capillary walls that leads to increased permeability of plasma protein into the glomerular filtrate. With long standing or extremely heavy proteinuria, serum albumin is decreased resulting in hypoalbuminemia.
The generalized edema is in turn, a consequence of the drop in the plasma colloid osmotic pressure as a result of hypoalbuminemia and retention of salt and water by the kidney.
As the fluid escape from the vascular tree into the tissues, there is concomitant drop in plasma volume, with diminished glomerular filtration. Compensatory secretion of aldosterone along with the reduced GFR and reduction of secretion of natriuretic peptides, promotes retention salt and water by the kidneys, thus further aggravating the edema. By repetition of this chain of events, generalized edema (anasarca) may develop.
It is possible that hypoalbuminemia triggers increased synthesis of lipoproteins in the liver and thus hyperlipidemia. the lipiduria reflects the increased permeability of the GBM to lipoproteins.
The relative frequencies of the several causes of the nephrotic syndrome is almost always caused by a primary kidney disease, whereas among adults it is often due to renal manifestations of a systemic disease. The most frequent systemic causes of the nephrotic syndrome in adults are (DM, amyloidosis, SLE)
The most primary glomerular lesions that lead to the nephrotic syndrome are:
Focal and segmental glomeruloscrelrosis (FSGS), which is more important in adult
Minimal changes disease (MCD), which is more important in children.
Membranous nephropathy
Membanoproliferative GN
Minimal change disease (MCD) (lipoid nephrosis):-
This is the most frequent cause of nephrotic syndrome in children mostly between ages 1 and 7 years (65%). The glomeruli have normal appearance under L.M. however E.M. shows diffuse effacement of podocyte damage. The cells of the proximal convoluted tubules are often heavily loaded with protein droplets and lipids secondary to tubular reabsorption of the leaking lipoproteins. The renal function is preserved in most individual . the protein loss is confined to the smaller serum proteins, chiefly albumin (selective proteinuria). The prognosis in children with the disorder is generally good, more than 90% of cases respond to a short course of corticosteroid therapy.
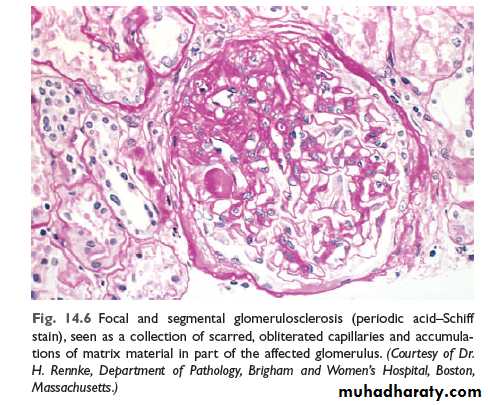
Focal and segmental glomerulosclerosis:-
Is characterized histologically by sclerosis (fibrosis) affecting some but not all the glomeruli (focal) and involving only segments of each glomerulus (segmental).FSGS is either primary or secondary. The former is the common cause of nephrotic syndrome in adults (30%) and frequent cause in children (10%). The secondary form is seen with :HIV immunodeficiency or heroin abuse (HIV nephropathy , heroin nephropathy)
IgA nephropathy
Maladaptation after nephron loss
Mutation affecting cytoskeletal proteins of podocytes (e.g. nephrin) (inherited form).
Unlike MCD there is higher incidence of hematuria and hypertension; the proteinuria is nonselective and the response to the corticosteroid therapy is poor. At least 50% of individuals with FSGS develop end stage renal failure with 20 years of diagnosis. The pathogenesis of primary FSGS is unknown.
As with MCD, permeability – increasing factors produced by lymphocytes have been proposed. The entrapment of plasma proteins and lipids occur in foci of injury where the sclerosis occur .
FSGS initially affects focally the juxtamedullary glomeruli. With progression eventually all level of the cortex are affected.
The affected segment of the glomerulus shows increased mesangial matrix , obliterated capillary lumens and deposition of the hyaline masses . in time progression of the disease lead to global sclerosis of the glomeruli with secondary tubular atrophy and interstitial fibrosis. About 50% of individuals suffer renal failure after 10 years.
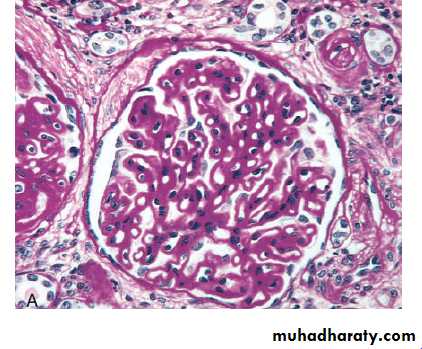
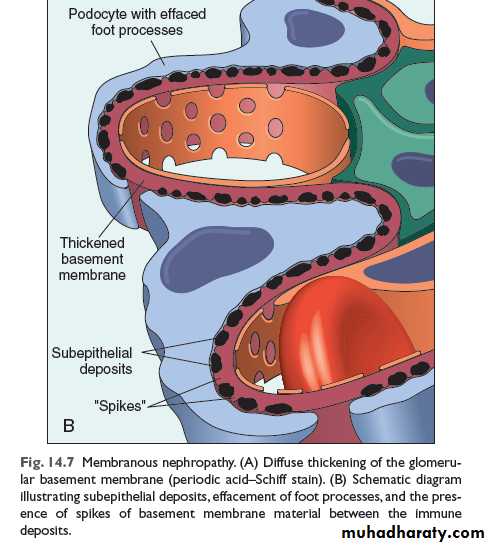
Membranous nephropathy (membranous glomerulonephritis, MGN):-
This slowly progressive disease most commonly in adults 30 -50 years of age the disease is of idiopathic (primary in about 85%) of cases. In the remainder it may be secondary to other disorders, including :-Infections(chronic hepatitis B, syphilis, malaria, schistosomiasis)
Malignancy especially lung , colonic carcinoma and melanoma
Autoimmune disease e.g. SLE
Exposure to inorganic salts (gold, mercury)
Drugs (penicillamin, captopril, NSAID)
MGN is a chronic immune complex nephritis, most idiopathic form are considered autoimmune diseases caused by antibodies to renal GBM autoantigen. There seem to be a direct action of the C5b-C9 (the membrane attack complex) on the podocytes and mesangial cells, inducing them to liberates protease and oxidants that can cause the damage .
The basic changecs microscopically is the diffuse thickening of the GBM. By E.M. this thickening is caused by subepithelial deposits that are separated from each other by small spike like protrusions of GBM matrix (spike and dome pattern ); these can be highlighted by silver stains. With progression these spikes close over the deposits, to incorporate them into the GMB.
Podocytes show effacement of foot processes. Eventually the glomeruli become gradually sclerosed.
IFM shows typical graunular depositis of immunoglobulin and complement along the GBM nonselective, involving globulins and albumin molecule .
overall only 40% suffer progressive disease terminating in renal failure after 2- 20 years.
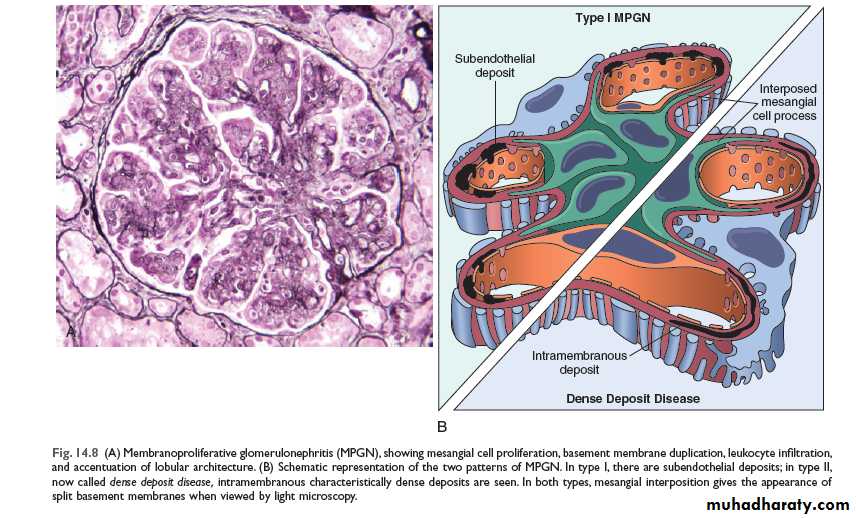
Membranoproliferative glomerulonephritis:-
This is manifested histologically not only by GBM thickening but also by proliferation of the glomerular cells.It account for up to 10% of cases of primary nephrotic syndrome in children and adults .
some individual present only with hematuria or subnephrotic proteinuria; other have combined nephrotic-nephritic picture.
Two major types of MPGN (I and II) are recognized; type I is far more common (80% of cases). Different pathogenic mechanisms are involved in the development of type I and type II disease . most cases of type I MPGN seem to be caused by circulating immunocomplexes. But the inciting antigen is not known (primary); it also occur as a secondary form in association of hepatitis B and C antigenemia ,SLE, and extra renal infections.
The fundamental abnormality in type II appears to be excessive complement activation .
by light microscopy both types of MPGN are similar. The glomeruli are large with an accentuated lobular appearance, and proliferation of mesangial and endothelial cells as well as leukocytic infiltration.
The GBM is thickened and the glomerular capillary wall often shows a double contour or ''tram track'' appearance especially evident in silver or periodic acid Schiff (PAS) stains. This is caused by ''splitting of the GBM '' due to inclusion(insertion) within it of processes of mesangial and inflammatory cells . type I AND type II have different ultrastructural and I.F.M features.
The prognosis of MPGN is generally poor in that 40 % of the cases progressed to end stage renal failure. Type II MPGN (also caused dense- deposit disease ) has a worse prognosis.
The nephritic syndrome:-
This is a clinical complex, usually of acute onset characterized byHematuria
Oliguria with azotemia
Hypertension
The lesions that cause nephritic syndrome have in common proliferation of the cells within the glomeruli, accompanied by leukocytic infiltration.
This inflammatory reaction injures the capillary walls permitting escape of the red cell into the urine and induces hemodynamic changes that lead to reduction in the GFR .
the reduced GFR is manifested clinically by oliguria, fluid retention, and azotemia. Hypertension is the result of both the fliud retention and excessive renin release.
The acute nephritic syndrome may be secondary to systemic disorders such as SLE or it may be the result of primary glomerular disease e.g. acute postinfectious GN.
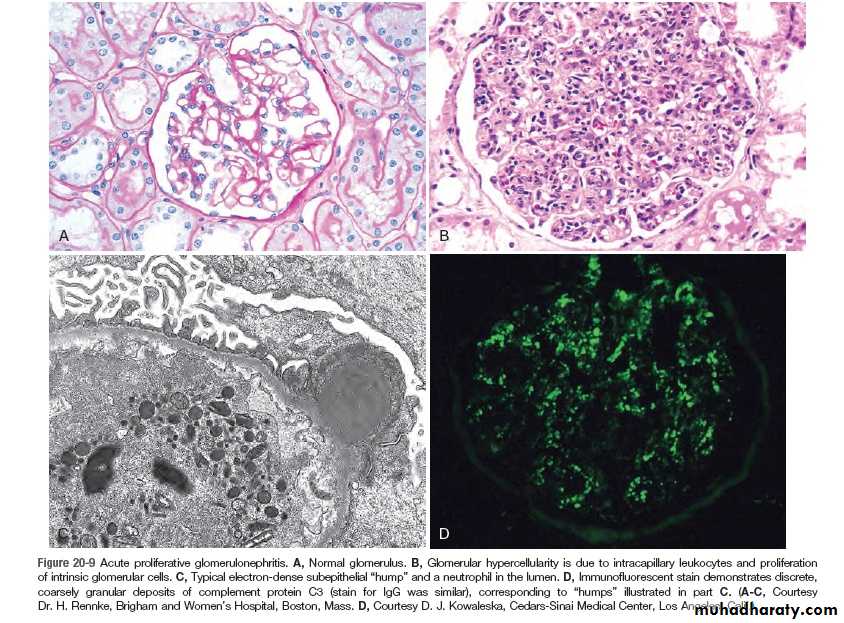
Acute postinfectious (post streptococcal) GN :-
This is typically associated with streptococcal infection, but other infectious agents may be responsible. The latter include certain pneumococcal and staphylococcal infections, as well as common viral diseases such as mumps, measles, chichenpox and hepatitis B and C .
The classic case of PSGN develops in children 1-4 weeks after recovery from nephritogenic ''strain of β- hemolytic group A streptococcal infection usually of the pharynx or skin.
Immune complex deposition is involved in the pathogenesis.
The relavent Ag are probably streptococcal proteins. Serum complement level are low and serum anti streptolysin O antibodies titers are elevated.
Characteristically the histology shows a uniform increased cellularity of the glomerular tufts . that affect nearly all glomeruli. This increases cellularity is caused both by proliferation and swelling of both endothelial and mesangial cells as well as by a neutrophilic and monocytic infiltrate .
E.M show subepithelial humps.
IFM display these immune complexes as scattered granular deposits of IGg and complement within the capillary walls.
Recovery occur in most children . (conversely up to 50% of adult develop end stage renal failure .
IgA nephropathy (Berger disease):-
Usually affects children and young adults as episodes of gross hematuria occurring within 1 to 2 days of nonspecific upper respiratory tract infections to last several days and then subsides only to recur every few months.IgA nephropathy is the most common cause of recurrent microscopically and gross hematuria and is the most common glomerular disease revealed by renal biopsies worldwide .
the pathogenic hallmark is the deposition of the IgA in the mesangium. IgA may be viewed as a localized renal variant of Henoch – Schonlein purpura, which is also characterized by IgA deposition in the masangium but it is a systemic syndrome characterized by purpuric rash, abdominal pain and arithritis. Microscopically, the glomeruli may be normal or show one of the following:
Focal proliferative GN
Diffuse mesangioproliferative GN
Crescentic GN (rare)
The characteristic IFM picture is of mesangial deposition of IgA. Electron microscopy shows mesangial electron – dense deposits.
Serum IgA is increased in 50% of patients due to its increased production in the marrow presumably in response to respiratory or GIT exposure to viruses, bacteria, or food proteins.
The deposition of IgA and IgA- immune complexes in the mesangium activate the alternative complement pathway and initiate glomerular injury. Slow progression to chronic renal failure occurs in up to 50% of cases.
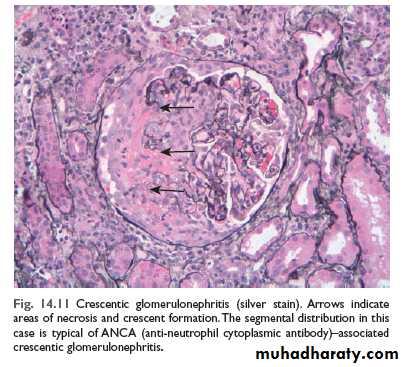
Rapidly progressive (Crescent) glomerulonephritis (RPGN; Cr GN):-
This is a clinical syndrome associated, irrespective of the etiology, with glomerular crescents; these are produce by proliferation of the parietal epithelial cells associated with infiltration by monocytes and macrophages. Cr GN is characterized clinically by:-
Rapidly progressive loss of renal function
Nephritic syndrome AND Severe oliguria (often)
Death from renal failure within weeks to months (if untreated)
A practical classification divide Cr GN into three groups on the basis of immunoglobuline findings. In each group the disease may associated with a known disorder or it may be idiopathic.
Type I (anti-GBM antibody):
Idiopathic
Goodpasture syndrome
This group is characterized by linear IgG deposits along the GBM. In some of these individuals the anti-GBM antibodies also bind to alveolar capillary basement membranes to produce the clinical picture of pulmonary hemorrhage associated with renal failure ( Goodpasture syndrome). In idiopathic cases the renal involvement occur in the absence of pulmonary disease. Anti GBM antibodies are present in the serum and are helpful in diagnosis.
IFM is characteristics with strong linear staining of deposited IgG and C3 along the GBM; these deposits are not visualized by E.M
Type II (immune complex):-
IdiopathicPostinfectious
SLE
Henoch –Schonlien purpura/ IgA nephropathy
In all of these cases, IFM shows the characteristic granular pattern of staining of the GBM and or mesangium for immunoglobulin and or complement.
Type III (pauci-immune) ANCA associated:-
Idiopathic
Wegener granulomatosis
Microscopic angitis
This group is defined by the lack morphologically of both anti-GBM antibodies and immune complexes deposition. Most of these individuals have antinutrophil cytoplasmic antibodies (ANCA) in the serum.
IF studies for immunoglobulin and complement are negative (cf of type I and II) and there are no ultrastructural deposits.
The onset of RPGN is much like that of the nephritic syndrome. proteinuria sometimes approaching nephrotic range may occur.
The prognosis can be related to the number of crescents; those with crescents in less than 80% of the glomeruli have a better prognosis than those with higher percentage of crescents.
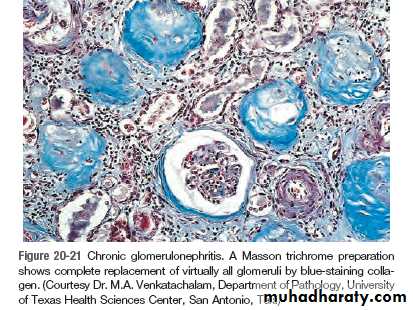
Chronic glomerulonephritis:-
Is one of the outcomes of the various glomerular diseases already discussed. It is an important cause of end stage renal disease.Among all individuals who require chronic hemodialysis or renal transplantation, 30-50% have the diagnosis of chronic GN. By the time chronic GN is discovered, the glomerular changes are so advanced that it is difficult to detect the nature of the original lesion.
Classically the kidneys are symmetrically contracted with red brown surface.
Microscopically the feature common to all cases is advanced scaring of the glomeruli. Sometimes to in the point of complete sclerosis.
There is relentless progression to uremia and death. The rate of the progression is extremely variable. Renal dialysis and kidney transplantation alter this course and allow long term survival.
Tubulointerstitial diseases:-
Most form of tubular diseases also involve the interstitium , so the two are discuss together. Under this heading are two categories:-Inflammatory involvement of the tubules and the interstitium (tubule-interstitial nephritis)
Ischemic or toxic tubular necrosis (ATN) leading to acute renal failure.
Tubulointerstitial nephritis (TIN):- is a group of inflammatory disease of the kidneys primarily involve the interstitium and tubules. The glomeruli are spared or affected late in the course . TIN is subdivided into:-
Bacterial TIN : the renal pelvis is prominently involved (pyelonephritis)
Nonbacterial TIN these include tubular injury resulting from drugs, metabolic disorders (hypokalemia), physical injury (irradiation), viral infection, immune reactions.
Pyelonephritis:- this divided into acute and chronic form.
Acute pyelonephritis:- is a common bacterial suppurative inflammation of the kidney and the renal pelvis, and an important manifestation of the UTI . the great majority of cases of pyelonephritis are associated with lower UTI (cystitis, prostitis, urethritis). Ecoli. Is by far the most common offender. Other important organisms are proteus , kelbsiela, enterobacter and pseudomonas. These are usually associated with recurrent infections, especially due to urinary tract manipulations or congenital or acquired anomalies
Pathogenesis:-
Bacteria can reach the kidneys either through the blood stream (hematogenous)(descending infection) or from the lower urinary tract (ascending infection). The former is exemplified by acute pyelonephritis complicating septicemia or infective endocarditis. Ascending infection from the lower urinary tract is the most common & is an important rout by which bacteria reach the kidney. The evolution of acute pyelonephritis occur through the following steps:
Bacterial adhesion to urethral urothelium is influenced by genetically determined propertitis of both urothelium and the offending bacterial facilitate
Gaining access to the bladder is by growth expansion of the colonies and by moving against the urine out flow, the latter is overcome by urethral instrumentation including catheterization and cystoscopy. In the absence of instrumentation, UTI most commonly affects females because of factors that facilitate entry of bacteria to the bladder these are:
The close proximity of the urethra to the enteric bacteria loaded rectum favoring colonization
The short urethra
Trauma to the urethra during sexual intercourse (honeymoon cystitis).
Outflow obstruction: normally bladder urine is sterile as a result of the antimicrobial properties of the bladder mucosa and the flushing action of periodic voiding of urine. With outflow obstruction or bladder dysfunction, these natural defenses are overwhelmed, setting the stage for the UTI . obstruction at the level of the urinary bladder result in incomplete emptying and increase residual volume of the urine . in the presence of the stasis , bacteria introduce into the bladder can multiply freely , without being flushed out or destroyed by the bladder mucosa. From the contaminated bladder urine , the bacteria ascend along the ureter to infect the renal pelvis and paranchyma . thus UTI is also frequently in DM because of the increased the susceptibility to infection and neurogenic bladder which in turn predisposes to urine stasis
Vesicoureteral reflux (VUR):- incompetence of the vesicouretral orifice is required to allow bacterial ascent along the ureter and then into the pelvis . the normal ureteral insertion into the bladder is a competent one way valve that prevent retrograde flow of urine , especially during micturition, when the intravesical pressure rises. An incompetent vesicoureteral orifice allow the reflux of the bladder urine into the ureter. This is termed vesicoureteral reflux (VUR). This condition is present in 40% of young children with UTI and is usually a congenital defect. VUR can also be acquired in individual with flaccid bladder resulting from spinal cord injury and with neurogenic bladder dysfunction secondary to DM.
the effect of VUR is similar to that of an obstruction in that after voiding there is residual urine in the urinary tract, which favors bacterial growth . furthermore, VUR affords a ready mechanism by which the infected bladder urine can be propelled up to the renal pelvis and farther into the renal parenchyma through open ducts at the tips of the papillae (intrarenal reflux).
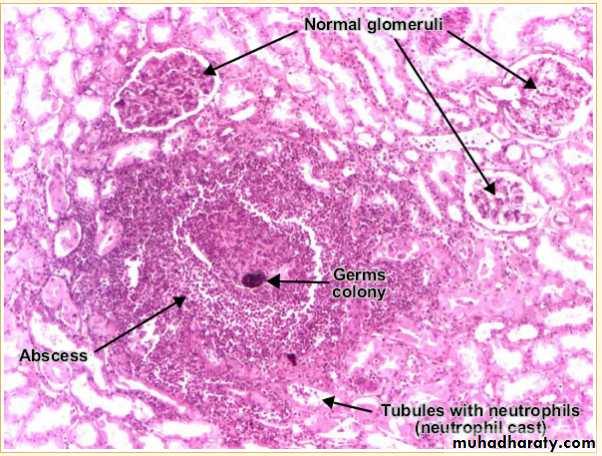
Gross features of acute pyelonephritis:-
one or both kidneys may be involved. The affected kidney may be normal in size or enlarged.
Characteristically ,discrete, yellowish raised abscesses are grossly apparent on the renal surface. They are variably scaterd and may coalesce to form a single large abscess.
When obstruction is prominent , the pus may fill the renal pelvis, calyces and ureter producing pyonephrosis
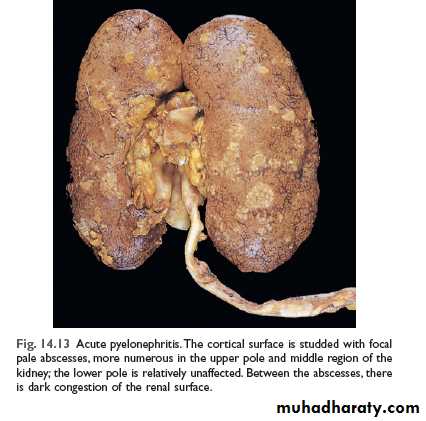
microscopic fearures:-
The characteristic features of acute pyelonephritis is suppurative necrosis with renal parenchyma. Both the tubules and interstitium are infiltratedLarge numbers of intratubular neutrophils frequently extending into the collecting ducts giving rise to the characteristic white cell cast found in the urine
Typically, the glomeruli are not affected.
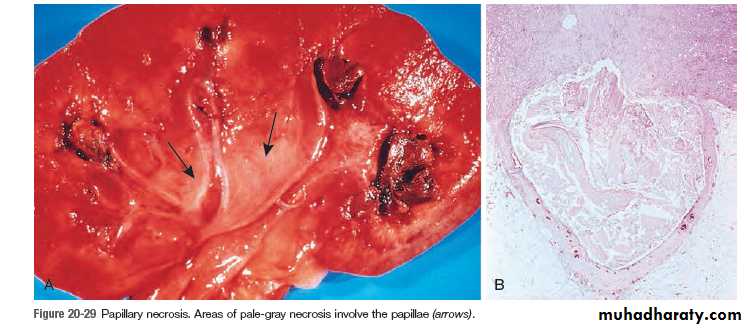
Papillary necrosis(necrotizing papillitis):-
This is an infrequent form of pyelonephritis, which may be encountered:
In DM
With significant urinary tract obstruction
Chronic interstitial nephritis associated with analgesic abuse.
This lesion consist of ischemic and suppurative necrosis of the renal papillae (tip of the renal pyramids). The pathognomic gross features is sharply defined gray- white to yellow necrosis of the apical two- thirds of the pyramids . the involvement range from one to all papillae. Microscopically, the papillae show characteristic coagulative necrosis with surrounding neutrophilic infilteration
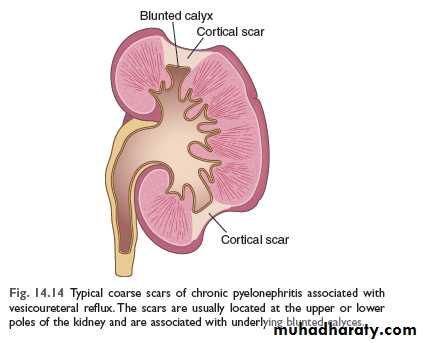
Chronic pyelonephritis (CPN) and reflux nephropathy:-
For the pathological diagnosis of the CPN two criteria must be presentGrossly visible scaring deformity of the pelvicalyceal system
Microscopic predominance of interstitial inflammation and fibrosis
CPN is an important cause of chronic renal failure . it can be divided into two forms.
Chronic obstructive pyelonephritis: recurrent infections superimposed on obstructive lesions lead to recurrent bouts of renal inflammation and scaring, which eventually cause chronic pyelonephritis. The disease can be bilateral as with congenital anomalies of the urethra (posterior urethral valves), or unilateral such as occur with calculi and unilateral obstructive lesions of the ureter
Chronic reflux –associated pyelonephritis is the more common form and results from superimposition of a UTI on congenital vesicouretral reflux and intrarenal reflux. Reflux may be unilateral or bilateral; , thus, the resultant renal damage is either unilateral or bilateral
Gross features:-
One or both kidneys may be involved, either diffusely or in patches, even when involvement is bilateral , the kidneys are not equally damaged and therefore are not equally contracted kidneysThe hallmark of CPN is scaring involving the pelvis & or calyces leading to papillary blunting and marked calyceal deformities
Microscopic features:-
These are largely non- diagnostic since similar alteration may be seen with other tubulointerstitial disorders such as analgesic nephropathy.The parenchyma shows the following features.
-interstitial fibrosis with infiltration by lymphocytes, plasma cells, and sometimes neutrophils
-dilation or contraction of tubules with atrophic lining epithelium. Many of the dilated tubules contain pink to blue colloid – like casts, the overall appearance is reminiscent of thyroid tissue , hence the descriptive term thyroidization.
Chronic inflammation with fibrosis involving the pelvi-calyceal mucosa and wall. This is an important feature that is used in the differentiation from other conditions give otherwise similar parenchymal changes.
vascular changes of benign arterioseclerosis caused by the frequently associated HT.
although glomeruli may be normal some are sclerosed (glomerulosclerosis). Such changes represent maladaptive changes secondary to nephron loss.
Absence of significant bacteriuria should not rule out CPN . if the disease is bilateral and progressive , tubular dysfunction occur with loss of concentrating ability, manifested by polyuria and necturia. Some persons with CPN or reflux nephropathy ultimately develop glomerular lesion of global sclerosis and secondary FSGN. These are associated with proteinuria and eventually contribute to progressive chronic renal failure.
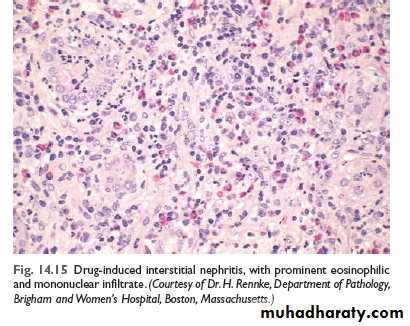
Drug –induced interstitial nephritis:-
Drugs are important cause of renal injury. These are two form of DITN:
Acute DIN:- this is most frequently occurs with such drugs as ampicillin, rifampicin, thiazide, diuretics, NSAID, ,phenindion and cimeditine. Most likely the drugs act as haptens that bind to a cytoblasmic or extracellular component of the secreting tubular cells and become immunogenic. The resultant tubulointerstitial injury is either caused by IgE,(type I) or cell mediated (type IV) immune reactions to tubular cells.
It is important to recognize drug-induce renal damage, because withdrawal of the offending drug is followed by recovery.
Analgesic nephropathy:-with intake of large quantities of analgesics, patients may develop renal papillary necrosis with chronic interstitial nephritis,
Most people who develop this nehropathy consume mixtures containing some combination of aspirin, paracetamole, caffeine and codeine for long periods.
cessation of analgesic intake may stabilized or even improve renal function. A complication of analgesic abuse is the increased incidence of transitional cell carcinoma of the renal pelvis or bladder in persons who survive with renal failure .
Diseases of renal blood vessels :-
Changes affecting blood vessels are both frequent and important for the following reasons:-The renal vasculature is secondarily involved in almost diseases of the kidney
Various form of systemic arteritis also involved blood vessels and such involvement is secondarily important
The kidney is intimately involved in the pathogenesis of both essential and secondary HT
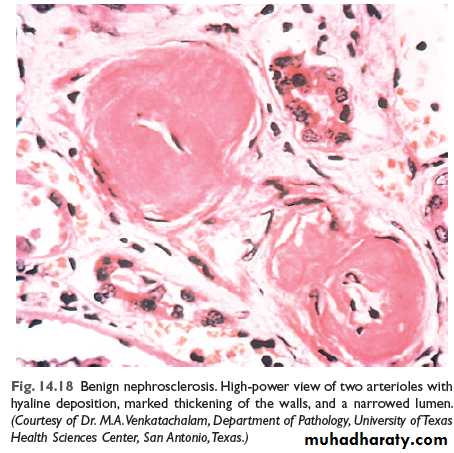
Benign nephrosclerosis (BNS):-
Some degree of BNS is present in many of those older than 60 years of age.
The frequency and severity of the lesion are increased at any age when HT &DM is present .
it is not clear whether BNS is a cause of HT or conversely, HT just accelerates an age related vascular seclerosis.
Howevere many renal diseases cause HT which in turn associated with BNS . thus this renal lesion is often seen superimposed on other primary kidney diseases
Gross features:-
The kidneys are symmetrically shrunken with diffuse fine granularity of the surface
Microscopic features :-
The basic changes are hyaline thickening of the walls of the small arteries and arterioles (hyaline arteriosclerosis). This appears as a homogenous pink hyaline thickening that reduce the lumen
The narrowing of the lumen result in markedly decreased blood flow through the affected vessels and thus producing ischemic atrophy of all structures of the kidney.
In advance cases the glomeruli become globally seclerosed . diffuse tubular atrophy and interstitial fibrosis are often present.
BNS rarely causes severe damage to the kidney . however all person with this lesion usually show some functional impairment
Malignant nephroseclerosis:-
Malignant HT occur in only about 5% of hypertensive pateints. It may occur de novo or suddenly complicates mild HTPathogenesis
The following sequence of event is suggested
Initially there is renal arteriolar vascular damage mostly from long standing benign HT. the result is increased permeability of the small vessels to fibrinogen and other plasma proteins, endothelial cell injury and platelets deposition
This lead to occurrence of fibriniod necrosis of the arterioles and small arteries with thrombosis
Platelet derived and other growth factors cause intimal smooth muscle hyperplasia
With severe involvement of the renal afferent arterioles , the renine stem is cycle is thus created in which angiotensin II causes intrarenal vasoconstriction and the resultant renal ischemia stimulates renini secretion.
Aldosterone levels are elevated the salt retention contributes to the elevation of the blood pressure
The consequences of markedly elevated blood pressure on the blood vessels throughout the body are known as malignant arteriosclerosis and the renal disorder is referred to as malignant nephroseclerosis.
Gross feature:
The kidney which may be normal in size or slightly shrunken display small pinpoint petechial hemorrahges on the cortical surface due to rupture of arterioles or glomerular capillaries. These give the kidney a pecular flea –bitten appareance
Microscopic:-
There is fibrinoid necrosis of the arterioles. The vessel walls show homognous granular eosinophilic appareance.
In the small arteries and large arterioles, proliferation of the intemal smooth muscle cells produce hyperplastic arterioloselerosis in which the intimal smoothe cells show concentric arrangement (onion skin appearance). This lesion cause marked narrowing of the arterioles and small arteries to the point of total obliteration
Necrosis may also involve glomeruli, with microthrombi within the glomeruli and necrotic arterioles.
The full-developed syndrome of malignant HT is characterized by diastolic pressures greater than 120 mmHg, papilledema, encephalopathy cardiovascular abnormalities and renal failure at the onset of rapidly rising blood pressure there is marked proteinutia and microscopic or sometimes macroscopic hematuria followed soon by renal failure. The syndrome is a true medical emergency. About 50%of patients survive at least 5 years. Ninety percent of deaths are caused by uremia and the other 10% by cerebral hemorrhage or cardiac failure
Urinary Tract Obstruction "Obstructive Uropathy"
CausesCongenital abnormalities or anomalies:
urethral valve
urethral stricture
meatal stenosis
bladder neck obstruction
uretero-pelvic Junction Obstruction
severe vesico-ureteral reflux
urinary stone
Benign prostatic hypertrophy
Tumors (Ca. prostate, bladder, cervix, ureter, Renal pelvis, retroperitoneum).
Inflammation: prostatitis, ureteritis, urethritis, retroperitoneal fibrosis, endometriosis.
Sloughed necrotic papillae, blood clots.
Pregnancy, uterine prolapsed.
Neurogenic bladder (spinal cord damage).
Obstruction either
sudden or insidious onset
complete or intermittent & partial
Unilateral or Bilateral
Obstruction increases the susceptibility to infection UTI and stone formation, if not relieved → permanent renal atrophy.
Complication
1. Infection.2. Stone formation.
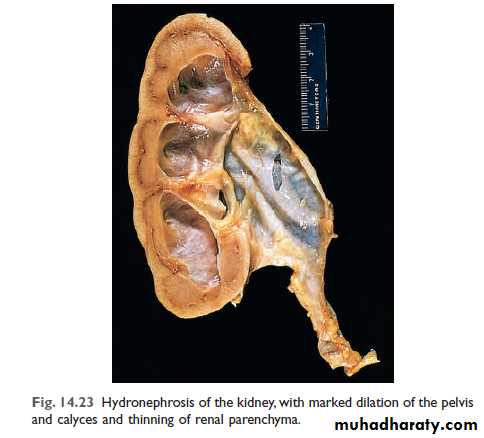
3. Hydronephrosis.
Effects of urinary obstruction
HydronephrosisDilatation of the renal pelvis and calyces with progressive atrophy of the kidney due to chronic incomplete (Partial) obstruction to urine outflow.
With more progressive dilatation → more atrophy of renal parenchyma and kidney become as cystic structure
Effects:
1. infection2. stone formation
3. Renal Failure (Bilateral)

Renal Stones (calculi, Urolithiasis)
Can occur at any level of urinary tract, but mainly occur in the kidney.Male > Female.
Types: according to the constituents of stones, can be classified into:
1. Calcium stones. 80%
2. Triple phosphate stone. 10 – 15%
3. Uric acid stone. 6%
4. Cystine stone. 1 – 2%
Calcium stones
Composed of
Calcium oxalate
Calcium phosphate.
mixed.
Hypercalciuria, hypercalcemia & Hyperoxaluria
The stone are radio opaque.Formed in acidic urine
Triple phosphate (Struvite) stone
Composed of magnesium, ammonium & phosphate.
Formed in alkaline urine by urea splitting bacteria
stag-horn stones (infection)
Radio opaque.
Uric acid stone
Common in pt. with hyperuricemia, such as gout-Radiolucent.
Formed in acidic urine
Cystine stones
occur due to genetically defect in the renal transport of amino acid like cystine.Predisposing factors
1. Decreased urine volume (dehydration).
2. Increased of stone constituents
3. Obstruction + Stasis of urine,
e,g, Prolong immobilization.
4. Infections.5. change in urine PH.
6. Diet. Vitamin A deficiency.
7. Idiopathic
8. Lack of inhibiter of crystal formation & urinary mucoprotein
Effects and complications
1. Passage of small stone → down the ureter to bladder → severe renal colic with injury to ureter → hematuria & /or inflammation → stricture with subsequent impaction.
2. Passage of large stone → impaction at upper or lower end of ureter or pelvic brim → stasis causing hydroureter, hydronephrosis & infection + stasis with further stone formation – stag horn stones
3. Pelvic suppuration and ulceration.
4. Squamous metaplasia of pelvis Transitional epith. with risk of development of Sq. cell Ca.
Urinary bladder stones
Either single or multiplemost cases arise in renal pelvis and pass down to bladder where grow to larger size sometime very large size
it cause cystitis, hematuria, obstruction, ulceration of mucosa, Squamous metaplasia & risk of Sq. cell . Ca.
Tumors of the Kidneys
Benign TumorsAdenoma
Small yellowish cortical tumor
less than 5 mm Ø.
Angiomyolipomas
Hamartoma composed of mixture of blood vessels, smooth muscle, and fat, common in patient with Tuberous sclerosis.Oncocytoma
Epithelial tumour composed (oncocytic cells), may reach large size 12 cm Ø.
Renal hemangioma
Hematuria.
Renal fibroma
Small round whitish nodule of fibrous tissue
Seen in medulla
Malignant Tumors
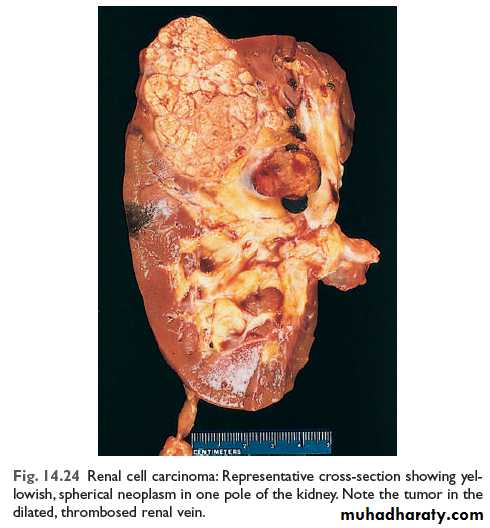
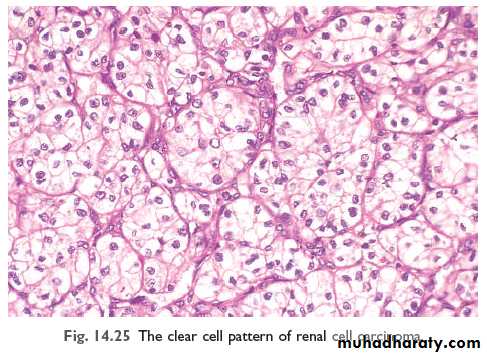
Renal cell carcinoma, Hypernephroma , AdenocarcinomaClear cell carcinoma
The commonest primary malignant renal tumor in adult90% of all renal cancers (tubular epithelial cell)
1-3% of visceral cancers.
Most common in 50-70 years of age
Male predominance
Most cases sporadic, very few familial cases.
40% of patient with von- Hippel-lindaue disease (retinal hemangioma with cerebellar hemangioblastoma) develop RCC, usually bilateral (AD disease)
Grossly: rounded mass 3-15 cm or more, partially encapsulated, yellowish-orange in color, with areas of hemorrhage, necrosis and cyst formation.
Histology: tumor composed of large clear cells (Clear Cell Carcinoma) rich in glycogen and lipid, arranged in solid masses, tubules, acini, and papillae, some tumor composed of granular cells
clinically
Hematuria Loin pain
Palpable abdominal mass
Paraneoplastic syndromes due to hormone secretions: Hypocalcaemia (PTH), Polycythemia (erythropoietin), H.T (renin), Cushing syndrome (glucocorticoid), Amyloidosis.Secondaries (pathological fracture) Bone
Prognosis
depend on Tumour size, Grade and Stage (extent of spread). RCC has tendency to metastasize widely before the diagnosis.
may invade peri-renal fat, adrenal glands and others.
Commonly invades renal vein, blood spread to lungs, bone, also to the lymph nodes by lymphatic.
5- year survival is 45%, and up to 70% in absence of metastasize.
Wilm's Tumour (Nephroblastoma)
commonest malignant renal tumour in infant and childhood25% of all cancer in children
Most occurs between 2-5 years
Usually unilateral as palpable Abdominal Mass
Most cases are sporadic
few cases 5-10% familial associated with other developmental malformation syndrome have deletion in chromosome 11p
(aniridia, genitourinary anomalies, mental retardation), hemihypertrophy. & It is embryonic tumor derived from renal blastema
Gross: large soft well – circumscribed whitish renal mass rapidly invades blood vessels and give pulmonary metastasis.
Triphasic histological features
Blastema cells – small round cells.
2. Epithelial cells – forming primitive tubules and primitive glomeruli.
3. Stromal spindle cells
Prognosis
improved recently by combination of surgery + chemotherapy + radiotherapy
90%-95% - survival or cure.
Younger than 2 years children have better prognosis than older children.
Transitional cell carcinoma of Renal Pelvis
5-10% of renal tumourEarly diagnosed because of obstruction, hematuria, or renal colics
Similar to urothelial tumour of bladder, most are papillary
Prognosis
Good for papillary superficial-low grade tumor70% -- 5 yrs survival
Poor for Invasive (infiltrating )--high grade tumour
10% --5 yrs survival
Secondary tumor
are not uncommon in kidney
Diseases of the urinary Tract
1. Obstruction
2. Infections
3. Stone formation
4. Tumors
Ureter
Obstructive lesions most important causing hydroureter and hydronephrosisIntrinsic Factors
Stone < 5mm Ø causing renal colic, larger not enter
Stricture either congenital or acquired (inflammation)
Tumour – TCC
Blood clots: massive hematuria from stone, tumours, papillary necrosis.
Neurogenic bladder
Extrinsic Factors
Periureteral inflammation: e.g.: salpingitis, peritonitis, diverticulitis, retroperitoneal fibrosis & endometriosis.Tumour: e.g. rectum, bladder, prostate, ovaries, uterus, cervix, lymphoma, sarcoma
ureteral obstruction is one cause of death in cervical carcinoma.
Urinary bladder
Congenital anomalies
Diverticula
Congenital defect or more commonly acquired from persistent urethral obstruction
Predispose to infection, stone formation, vesicoureteral reflux & rarely carcinoma.
Bladder Extrophy
Incomplete closure of anterior abdominal & bladder walls, as exposed sacPredispose to infection and adenocarcinoma
Inflammation
Acute and Chronic CystitisVery common, causing frequency, dysuria, lower abdominal pain & fever
chronic cystitis is the result of repeated attacks of acute cystitis-
common in female especially during pregnancy.-
common in elderly male it associated with obstruction of the urethra caused by BPH or urethral stricture.
Causative agents:
Bacteria e.g. E- coli, proteus, klebsiella
viruses e.g. cytomegalovirus, adenovirus
Fungi e.g. Candida (in immunosuppressed patients, “AIDS, cancer patient, DM, and receiving long-term Antibiotic”) Chlamydia & Mycoplasma.
Tuberculous cystitis
Occurs secondary to TB of kidney & epididymis.
Radiation cystitis
hemorrhagic cystitis due to chemotherapy such as cyclophosphamide.
Bilhariziasis is common in Egypt, produce chronic granulomatous cystitis & predispose to carcinoma.
Special forms of cystitis
Interstitial cystitis (Hunner ulcer)Chronic cystitis of unknown etiology
Commonly seen women
Associated with severe pain not respond to treatment.
Malakoplakia: (soft Yellowish plaques)
Chronic bacterial cystitis (E. coli & Proteus)characterized by soft- yellowish plaques covering bladder mucosa
It may occurs in other organs such as colon, lung, bones, kidney & prostate.
Metaplasia
Two types occur in bladder mucosa1. Glandular (intestinal) metaplasia
Occurs in chronic inflammation, characterized by formation of cystic glands lined by columnar cells called cystitis cystica and cystitis glandularis, when extensive, carry risk of adenocarcinoma.
2. Squamous metaplasia
Result from chronic inflammation, stone, bilhariziasis, extrophy
predisposes to Squamous cell Carcinoma of the bladder.
Bladder Tumors
most bladder tumours 95% arise from transitional epithelium (Urothelium) “Transitional cell tumors“
Are very common.
Benign Tumours
Papillomais very rare, composed of finger - like papillae
May recur, local excision
some regard all transitional cell tumors are malignant, no papilloma = grade- I TCC
But other are not believed this.
Inverted papilloma
Downward growth of papillae with smooth surface, from benign nodule.Bladder Carcinomas
Are common.5% squamous cell carcinoma
1-2% adeno carcinoma
3-4% mixed carcinoma.
90% are transitional cell carcinoma
Predisposing factors
1. Smoking.
2. Infection: Bilharziasis.
3. Analgesic abuse.
4. Chemotherapy
5. Chemical substances: Naphthylamine.
Transitional cell carcinoma TCC
Commonest Ca. of bladder
Trigone common site
Also occurs in ureter and renal pelvis.
More in male, M/F: 3:1
Between 50-80 years.
Grading of TCC is important for prognosis
Low-Grade Papillary TTC (I – II)Papillary, Well-Differentiated Tumor
Usually Superficial- Non Invasive Tumor.
Good prognosis
Local Recurrence is common.
High-grade TTC (III-IV)
Most aggressive Sessile (Non-Papillary) TumorsLess-Differentiated Tumors
Invasion of muscle layers and lymphatic in the bladder wall are widespread and extensive
Very poor prognosis
Clinically – Painless hematuria
Frequency and Dysuria
Prognosis depend on
Tumor Grade
Tumor Stage
5-Yr survival is 95% for Low- Grade, 35% for High- Grade
Four morphologic patterns of bladder tumor:
Squamous cell carcinomaArise in areas of squamous metaplasia due to chronic inflammation and irritation as in stone and Billariziasis
Usually poorly – differentiated
Prognosis is very poor, Regardless of the tumour grade.
Death occurs in the first year of the diagnosis.
Adenocarcinoma
Uncommon 1-2 % of all cancerArise in the background of
chronic inflammation with cystitis cystica and cystitis – glandularis (glandular metaplasia)
Bladder Extrophy
Urachal remnant at the dome.