



GROWTH
& DEVELOPMENT
Dr. Mazin Al-Jadiry
13&14 Oct. 2014
The Newborn at birth
Until six hours ago, this baby
had spent all her life inside her
mother.
The mother had provided her
with food, breathed for her,
removed her waste products,
kept her warm and protected
her from damage and disease.
Suddenly, at the moment of
birth, the baby is on her own.
she is now a separate person
who can move freely and has
to breath, feed and excrete for
herself.
Infants go through many changes during their
first 12 months, and no two infants develop at
the same pace
Growing up
“Growing up” involves three major dynamic processes:
Growth
Development
Sexual Maturation
Physical Growth
Increase in the size of the body as a whole or the increase
in its separate parts.
Growth milestones are the
most predictable
, although
they must be viewed within the context of each child’s
specific genetic and ethnic influences.
It is essential to plot the child’s growth on
gender
and
age
appropriate charts
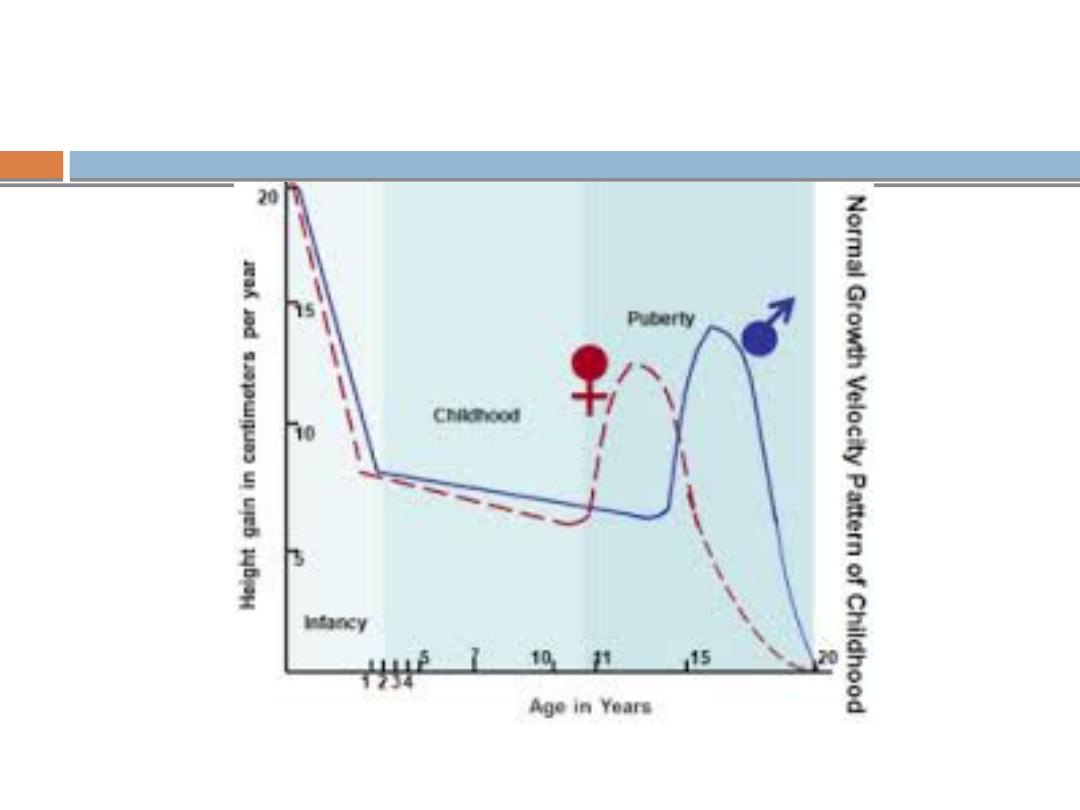
Physical Growth
The growth of a child occurs in four phases—
Fetal
Infantile
Juvenile
Adolescent
Fetal Growth
Prenatally, the growth of the
head
predominates, reaching
the peak in the third trimester.
The size of an infant at birth is affected:
Primarily by
maternal size
Secondarily by
other Intra uterine factors
such as
Maternal nutrition,
Use of tobacco and alcohol,
Placental adequacy,
Intrauterine infection and
Gestational age at birth
.
Infantile Growth
During the first 12–24 months after birth, the time of greatest
postnatal growth velocity, the infant
“seeks his or her own
curve.”
That is, by age 2–3 years, the child's stature reflects his
or her own genetic endowment rather than mother's size and
health.
Infancy is a period of rapid but
decelerating growth
; the
average of infant's birth weight doubles within 5 mo, but is
only triple at 1 yr.
Infantile Growth
Length follow a similar but less dramatic growth curve, it
increases by 30% at 5 mo, the growth rate slowly decreases so
that the length is only 50% above birth length at 1 yr.
Growth of the brain occurs almost exclusively during the early
years of life. At birth, it is 25% of adult size and at 1yr, 75%.
Full development is not achieved until adolescence.
Juvenile and adolescent Growth
Growth during the remainder of childhood occurs at a rate of
5–6 cm per year, along the percentile band achieved by 2–3
years.
Adolescence is characterized by an
abrupt
,
short-lived
increase in growth velocity (the “growth spurt”), mediated by
gonadal & growth hormones.
Adult height may to some degree be predictable by the mid-
parental height (maternal height plus paternal height, divided
by two).
Developmental Milestones
A skill that a child acquires within a specific time frame.
4 fields with a sequence of development:
Gross Motor - the development of locomotion
(Latin locō, from a place, place + motion).
Vision and fine manipulation - the development of eye-
hand control
Hearing & speech - the development of language
Personal & social - integration of acquired abilities to
reflect understanding of environment.
Developmental Milestones
Development progresses from generalized reflexes to
stimuli to voluntary discrete actions that are asymmetric
and precise toward stimuli (eg, grasping with one hand and
examining with the other).
Developmental control progresses from
cephalic to caudal
and from
proximal to distal
.
Sexual Maturation
The process of normal sexual development can be divided
into three discrete components:
1.
Differentiation of the bipotential fetal gonad and
development along either male or female phenotype;
2.
Maturation (puberty) with the attainment of secondary
sexual characteristics and the capacity for fertility; and
3.
The psychological concept of sexuality.
Milestones
Newborn

What a normal new baby can do
?
Although basically helpless, newborn babies are able to do
many things besides cry.
There are times when they sleep and times when they
are awake.
They can move their arms, legs and head.
They can stretch, hiccup, sneeze & make many other
movements
They are also able to receive a certain amount of
information from the world around them through the five
senses-
Sight
Hearing,
Touch
Smell & taste
From the day they are born, children learn and
develop by:
Touching
Seeing
Hearing
Smelling
Tasting
Moving
Doing (for example, playing).
Infantile development
Motor development is the major indicator of neurologic
health and proceeds in a cephalocaudal fashion.
Neonates demonstrate involuntary "primitive" reflexes, such
as the suck, grasp, and Moro (startle) responses, which may
be elicited to demonstrate muscle tone and should always be
symmetric.
These movements are inborn (existing from birth) and made
automatically without thinking
These reflexes mainly disappear by the age of 4-6 months and
are replaced by actions which the baby has to learn.
Primary Primitive reflexes
Rooting reflex; when gently touched on the cheek, the
baby's head turns as if in search of the nipple
Swallowing and sucking reflexes: when anything is put in
the mouth, the baby immediately sucks and swallows
Primary Primitive reflexes
The grasp response is elicited by placing a finger or object
in the open palm of each hand. Normal infants grasp the
object, and with attempted removal, the grip is reinforced.
Walking (stepping) reflex: when held upright with the feet
touching a firm surface, the baby will make walking
movements.
Primary Primitive reflexes
: any sudden movement which cause head
extension (gives the baby the feeling that he may be
dropped) causes extension following by flexion of the arms
and legs.
An asymmetric response may signify a fractured clavicle, brachial
plexus injury, or a hemiparesis on the side of the poorly abducted
arm).
Absence response in a term newborn is ominous, suggesting
significant dysfunction of the CNS. Abn.
Primary Primitive reflexes
(trunk incurvation) is obtained by
placing the baby in ventral suspension, then stroking
the skin on one side of the back. The baby’s trunk and
hips should swing towards the side of the stimulus.
this reflex is absent in transverse spinal cord lesions
or injuries.
Primary Primitive reflexes
manually turning the head to one side while
supine. Extension of the arm occurs on that
side of the body corresponding to the direction
of the face, while flexion develops in the
contralateral extremities.
An obligatory tonic neck response, by which the
infant remains “locked” in the fencer's position,
is always abnormal and implies a CNS disorder.
Secondary (Postural) reflexes
Become apparent after the newborn period, indicating proper
maturation of appropriate brain structures, the development of
postural reflexes is essential for independent sitting and walking.
occurs when the baby is falling to one side or the
other and he extends the arm laterally to catch himself.
it appears at age of 6-8 months, fully developed at age of 10-11 month
and never disappear
Asymmetric lateral propping can be an early sign of hemiparesis, the
baby will prop on one side but on the paretic side he will not
extend the arm to catch himself with the infant sitting
Secondary (Postural) reflexes
is the last of the postural reflexes
to develop. It usually appears at 8 to 9 months of
age. demonstrated by suspending the child by the
trunk and by suddenly producing forward flexion as
if the child were to fall. The child spontaneously
extends the upper extremities as a protective
mechanism. Asymmetry of the reflex is abnormal
and may indicate paresis in the non-extended
Although many primitive reflexes have been described,
the Moro, grasp, tonic neck, and parachute reflexes
are the most important.
Reflexes and Responses
Primitive reflexes
Appearance
Disppearance
Sucking
Birth
Persist
Stepping, placing
Birth
1-2 mo
Rooting
Birth
3-4 mo
Palmar grasp
Birth
3-5 mo
Moro reflex
Birth
4-6 mo
Asymmetric tonic neck
Birth to 2 wk
6-7 mo
Plantar grasp
Birth
9-12 mo
Galant (trunk incurvation)
Birth
9-12 mo
Reflexes and Responses
Postural responses
Appearance
Disppearance
Lateral propping
6-8 mo
Remain throughout life
Forward parachute
8-9 mo
Remain throughout life
Clinical Pearl
A delay in achieving milestones does not always
indicate an abnormality, most late talkers and
walkers turn out to be normal. Likewise, achieving a
milestone at a given time does not always indicate
normalcy. E.g. a child with cerebral palsy or Down
syndrome may meet early milestones on schedule.
Developmental testing is not a substitute for the
physical examination.
Testing is merely an adjunct to aid in forming a
complete picture about the patient.
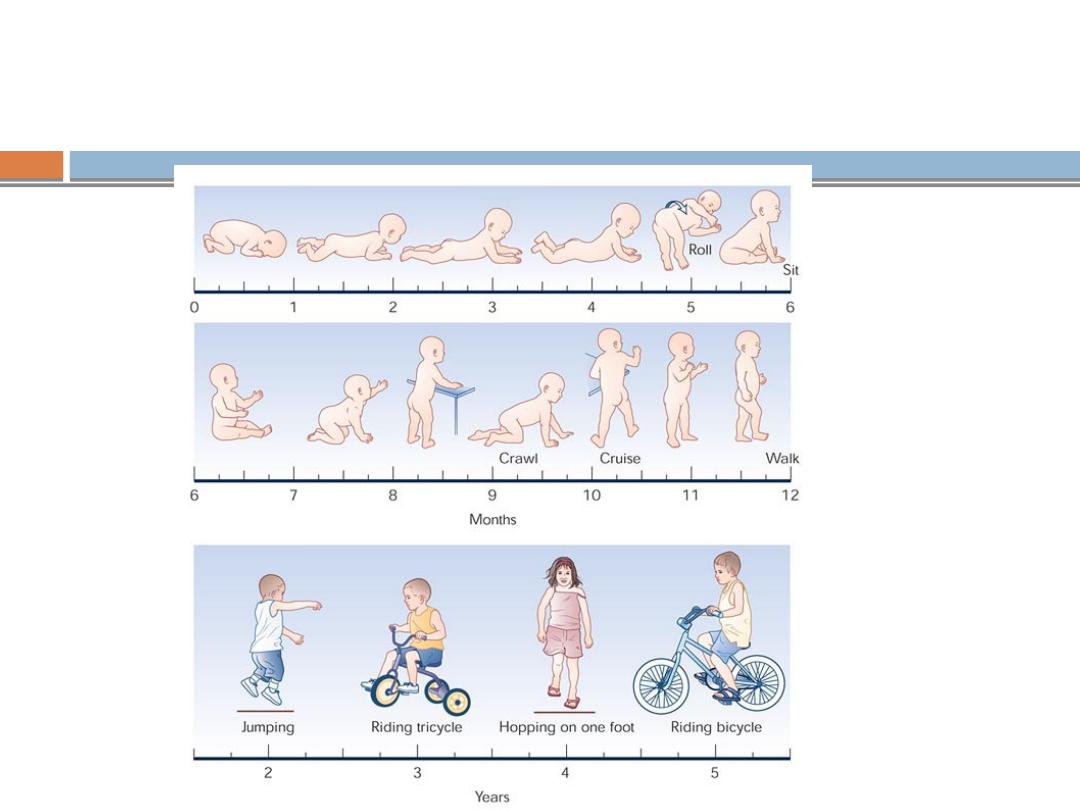
Progression of gross motor
milestones from birth to age 5 years
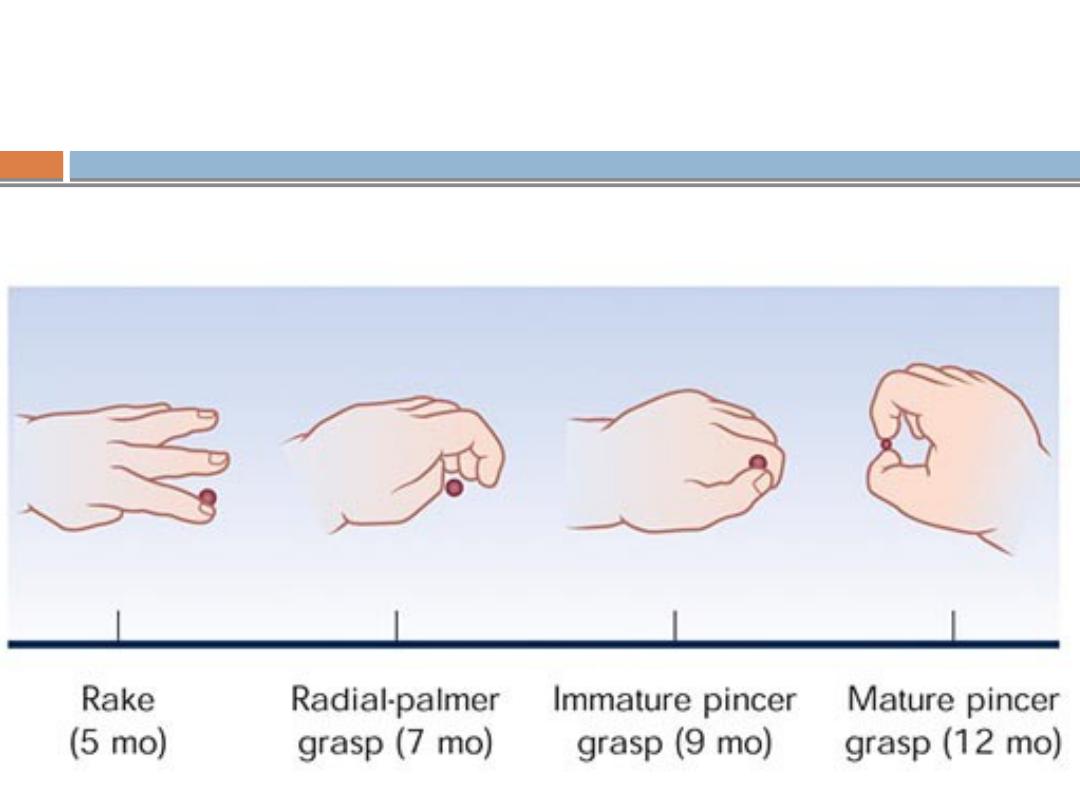
Progression of fine motor milestones
from birth to 12 months
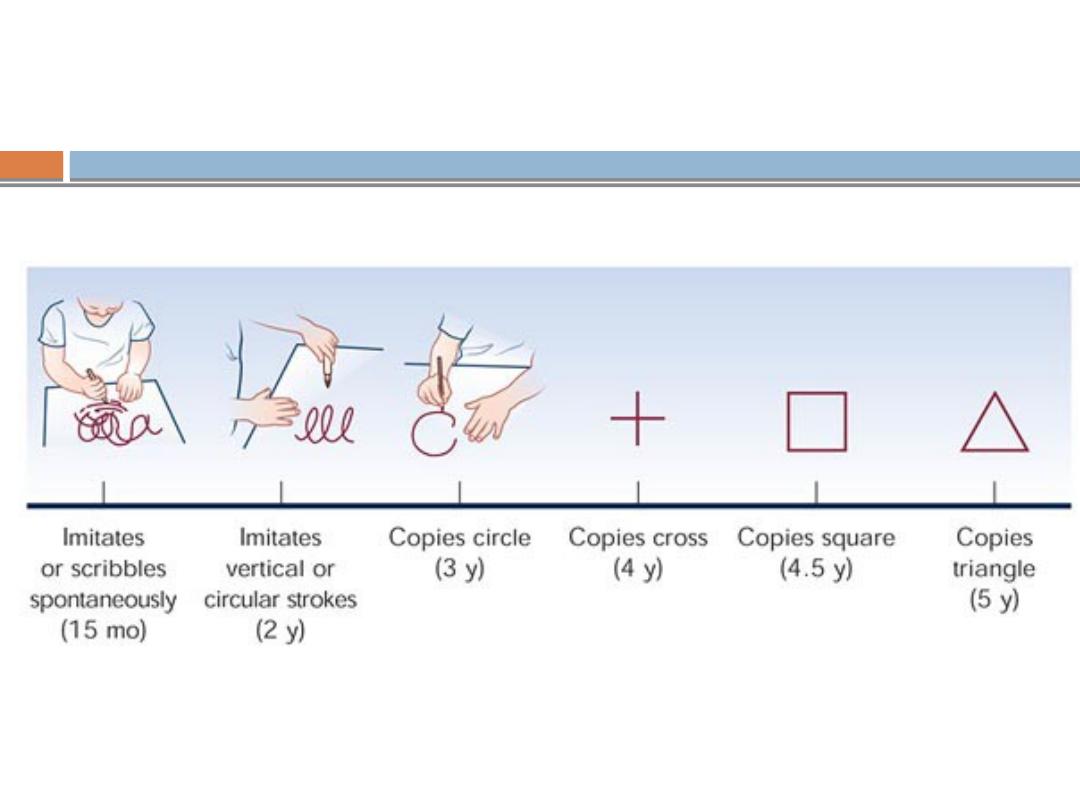
Progression of fine motor milestones
from 12 months to 5 years
Developmental Milestones
4 fields with a sequence of development
Gross Motor -
the development of locomotion
Vision and fine manipulation -
the development of
eye-hand control
Hearing & speech -
the development of language
Personal & social -
integration of acquired abilities to
reflect understanding of environment.
weeks
6-8
Smiles to maternal suggestions
Fixes & follows
Prone: pelvis flat, hips extended
Ventral: briefly holds head up
months
3
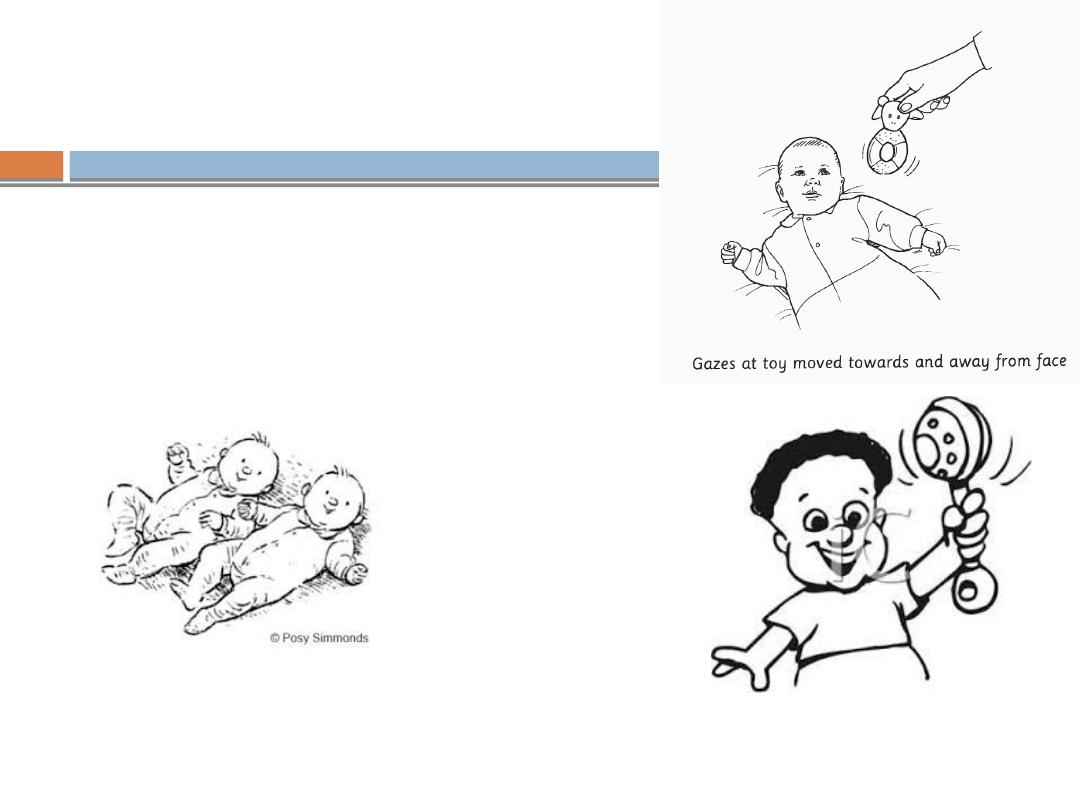
Holds head up, good eye contact
Holds rattle in hand
turns to sound ear level
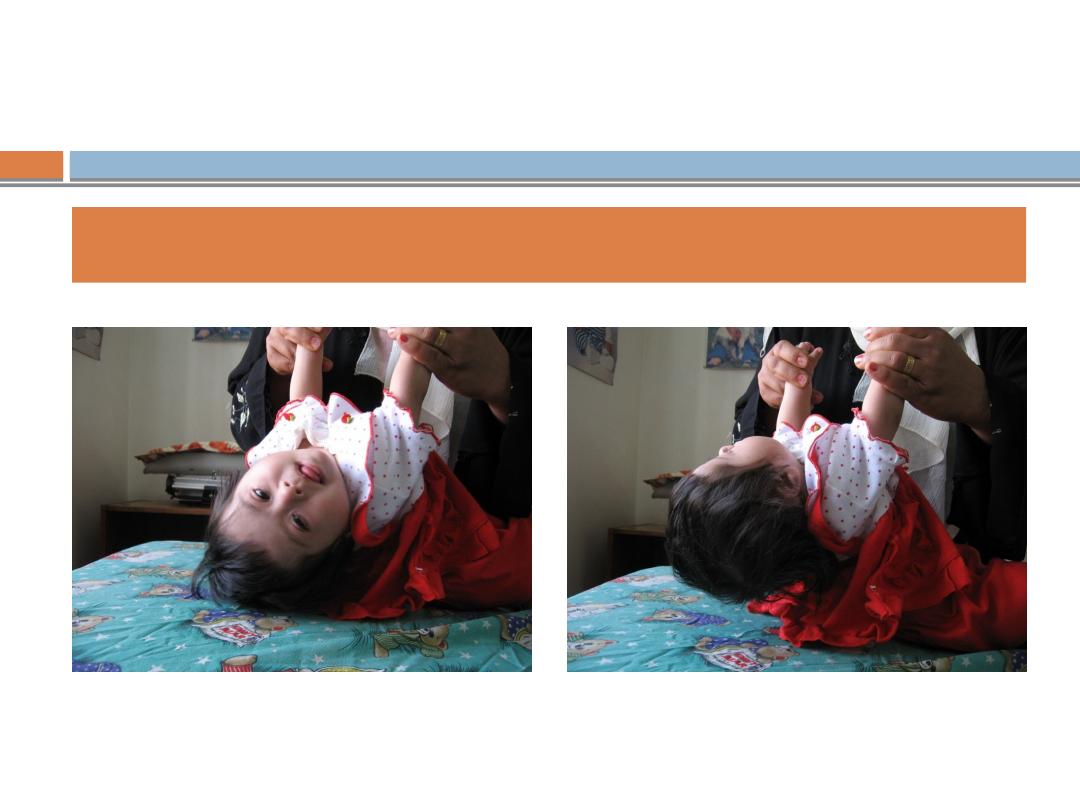
Head lag in a 5-month girl with Down syndrome
months
6
Transfers hand to hand
Chews, babbles
Sits supported (hands forward) (
Lifts head from supine
Recognize strangers
months
7-8
•C
om
es to
sit
•C
ree
p a
nd c
raw
ls
•C
om
es to
sit
•C
ree
p a
nd c
raw
ls
Gross Motor
Gross Motor
•In
sp
ects
obje
cts
•In
sp
ects
obje
cts
Visual-Motor/
Problem-
Solving
Visual-Motor/
Problem-
Solving
•“
Dada
” in
disc
rim
in
ate
ly
•“
Dada
” in
disc
rim
in
ate
ly
Language
Language
•F
ing
er fe
eds
•F
ing
er fe
eds
Social/Emotiona
l
Social/Emotiona
l
months
9-10
•Pul
ls to stan
d
•Crui
ses
•Pul
ls to stan
d
•Crui
ses
Gross Motor
Gross Motor
•Uses pi
ncer
grasp
•Probe
s with
foref
ing
er
•Hol
ds bottle
, t
hrow
s objects
•Uses pi
ncer
grasp
•Probe
s with
foref
ing
er
•Hol
ds bottle
, t
hrow
s objects
Visual-Motor/
Problem-
Solving
Visual-Motor/
Problem-
Solving
•“
Mama” ind
iscrimina
tely
•G
est
ures,
waves
bye
-bye
•“
Mama” ind
iscrimina
tely
•G
est
ures,
waves
bye
-bye
Language
Language
•St
arts t
o e
xpl
ore en
vironme
nt
•Pla
ys
gesture
games (eg
, pa
t-a
-cake)
•St
arts t
o e
xpl
ore en
vironme
nt
•Pla
ys
gesture
games (eg
, pa
t-a
-cake)
Social/Emotiona
l
Social/Emotiona
l
months
11-12
•W
alks al
one
•W
alks al
one
Gross Motor
Gross Motor
•Uses mature
pin
cer grasp
•Rel
ease
s voluntari
ly
•M
arks pape
r w
ith
penci
l
•Uses mature
pin
cer grasp
•Rel
ease
s voluntari
ly
•M
arks pape
r w
ith
penci
l
Visual-Motor/
Problem-
Solving
Visual-Motor/
Problem-
Solving
•Uses few
words o
the
r tha
n “dada/mama
”
•I
mmature
jarg
onin
g (ru
ns several
un
inte
lligi
ble
syll
ables toge
ther)
•Uses few
words o
the
r tha
n “dada/mama
”
•I
mmature
jarg
onin
g (ru
ns several
un
inte
lligi
ble
syll
ables toge
ther)
Language
Language
•I
mita
tes
act
ion
s
•Come
s when
ca
lled
•Coo
perat
es w
ith dressing
•I
mita
tes
act
ion
s
•Come
s when
ca
lled
•Coo
perat
es w
ith dressing
Social/Emotiona
l
Social/Emotiona
l
Important milestones
15 months:
walks alone, crawl up stairs. Makes tower of 3 cubes
18 months:
Runs stiffly. Picks up toy without falling over.
Gets up/down stairs holding onto rail.
Begins to jump with both feet.
Build a tower of 4 cubes and throw a ball.
Imitates vertical stroke.
Has vocabulary of 10 words.
Drinks from a cup with both hands.
Feeds self with a spoon.
Important milestones
2 years:
runs well.
Climb stairs.
Makes tower of 6 cubes.
Imitates horizontal stroke
Puts 3 words in sentences.
Develops control of sphincters (dry by day).
3 years:
Goes upstairs with alternate steps
Ride tricycle
Speak sentences of 6 syllables
Builds tower of 9 cubes
Copies circle
Undresses with assistance
Important milestones
4 years:
skips on one foot
Copies cross and square.
Dresses and undresses with assistance
Attends to own toilet needs
5 years:
Skips on both feet and hops
Copies triangle
Fluent speech with few infantile substitutions in speech
Knows 4 colours
Dresses and undresses alone
Developmental Warning Signs - at
any age
Family History of developmental problems; eg.
deafness, cataracts
Maternal concern
Persistent primitive reflexes
Persistent squint
Discordance in developmental abilities in
different areas
Regression of previously acquired skills
Red flags in Development
(abnormal signs or observations)
Age
Warning sign
10 wks
Not smiling
3 mo
Not responding to noise or voice, not focussing on
face, not vocalising, not lifting up head when lying on
stomach
5 mo
Poor head
6 mo
Not interested in people, noises, toys. Does not laugh
or smile. Primitive reflexes still present. Absent
babbling may indicate hearing deficit. Absent smile
may indicate visual loss
Red flags in Development
(abnormal signs or observations)
Age
Warning sign
9-12 mo
Not sitting, not saying baba mama, not imitating speech
sounds, no pincer grasp, inability to localize sound may
indicate unilateral hearing loss
18 mo
Not walking, no words, no eye contact
3 yrs
Unaware of surroundings, not imitating adult activities,
little or no speech
4 yrs
Unintelligible speech
At any age
Parental concern, regression of acquired skills
• Jump
"Jump"is a action performed by pushing
yourself off the ground using your feet.
The children were jumping up and down
with excitement.
•
Hop
"Hop" is a quick jump or series of jumps.
We crossed the stream by hopping from
one rock to another.
• I hopped on the bus at the traffic lights.
•
Skip
"Skip" is a small quick jump after each
step.
She skipped happily down the path.
•
Leap
"Leap" is a large jump from one place to
another.
The horse leaped the stone wall.
• We leapt over the stream.
THANKS