Reactive hyperplasia Dr. Hameed pathology
Reactive hyperplasias
•
Exaggerations of normal histology .
•
Expansion of all regions or selective expansion
•
Some types characteristic of certain diseases, but most not
•
Follicular hyperplasia- increase in number and size of germinal centers, spread into
paracortex, medullary areas
•
Collagen vascular diseases
•
Systemic toxoplasmosis
•
Syphillis
•
Interfollicular hyperplasia- paracortex
•
Skin diseases
•
Viral infections
•
Drug reactions
•
Sinus histiocytosis- expansion of the medullary sinus histiocytes-
•
Adjacent cancer
•
Infections
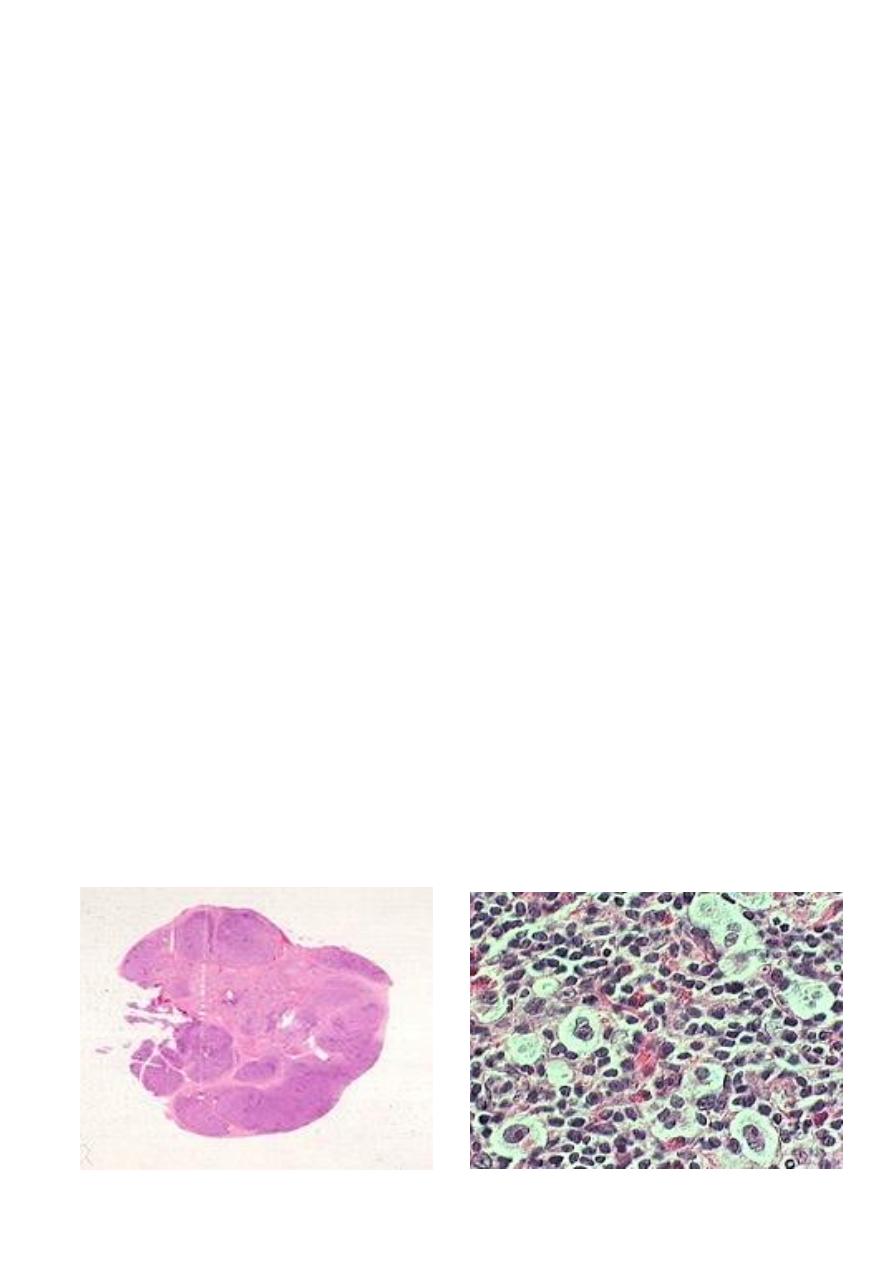
F .63 ISOLATED ENLARGED LT .SUBMANDEBULAR LYMPH NODE
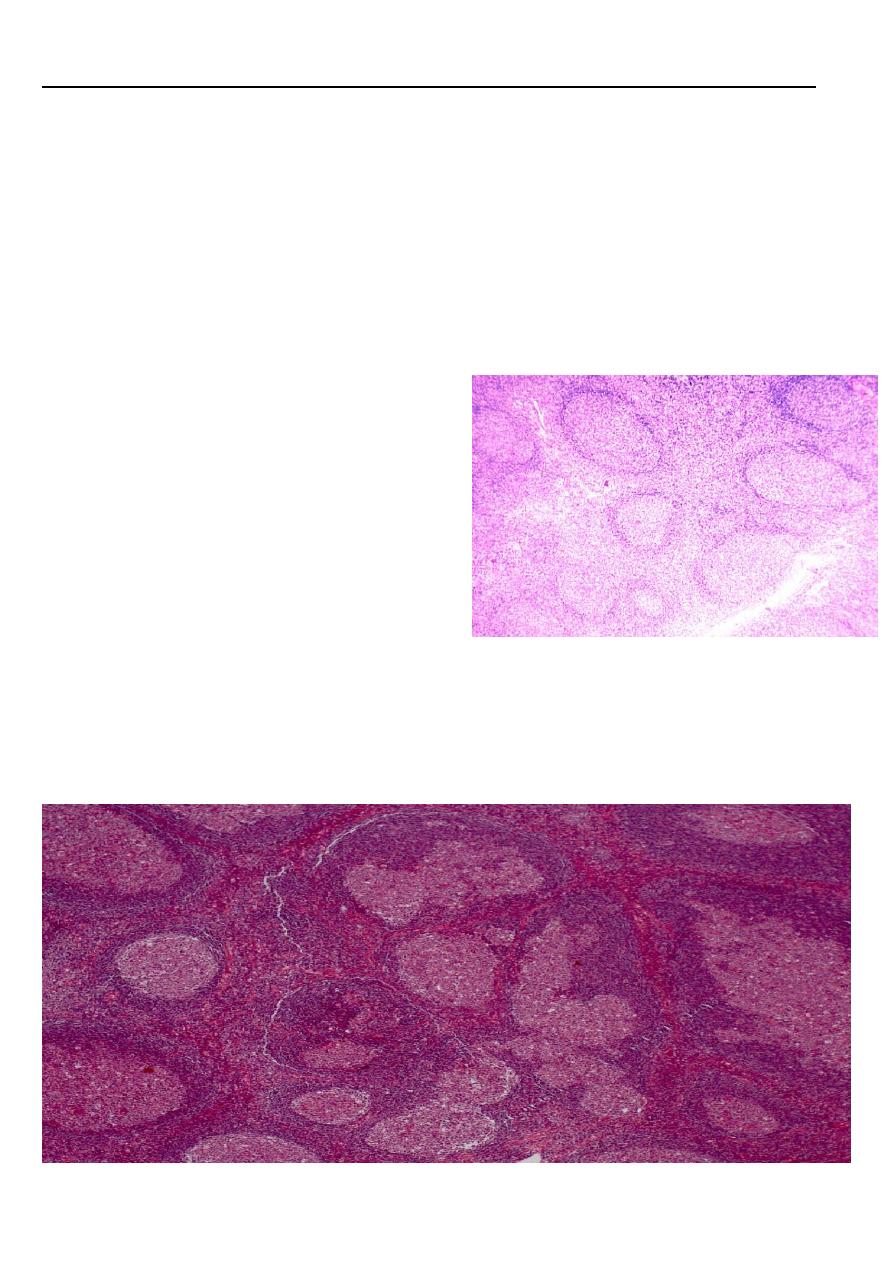
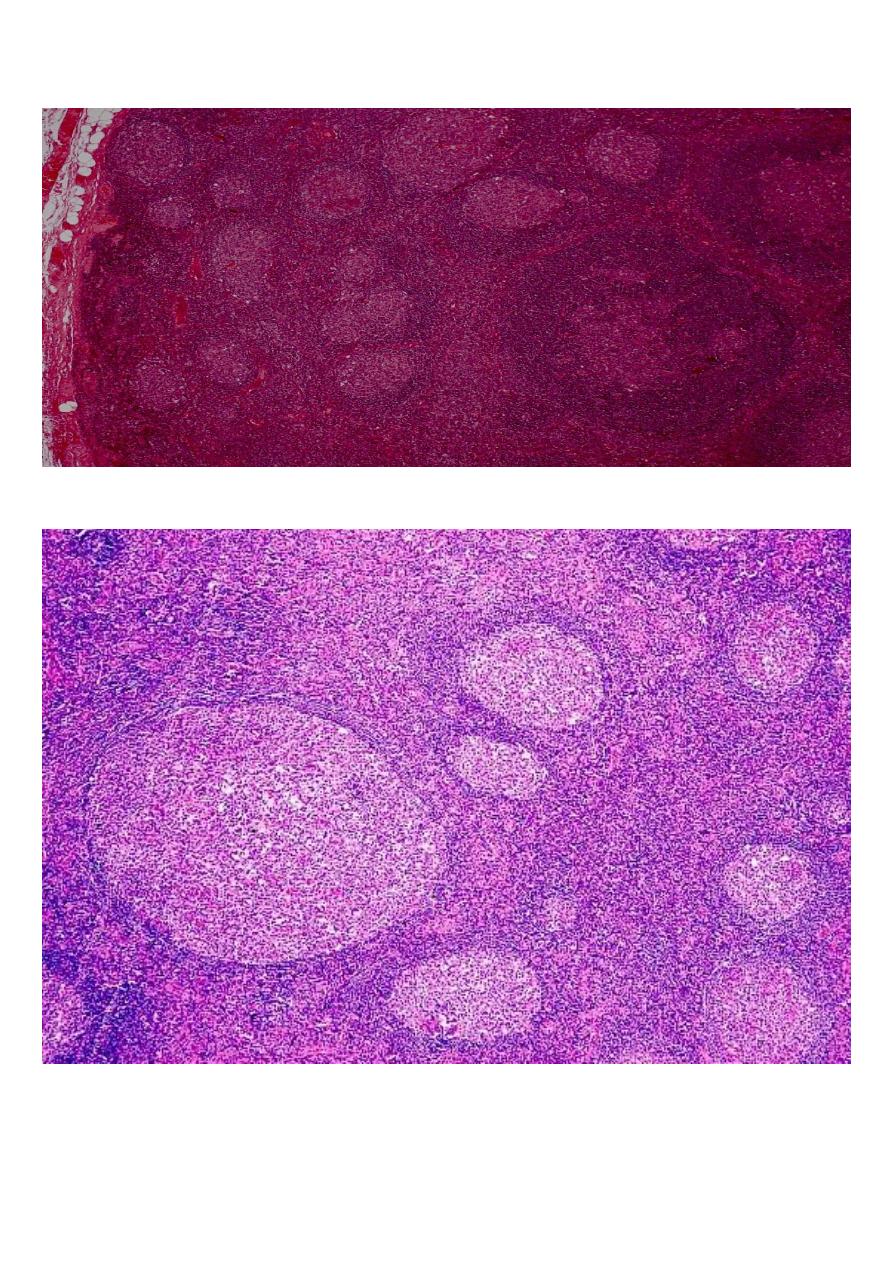
Follicular hyperplasia lymph node LP mic
There is marked differences in size of germinal centers, their well-circumscribed character,
and the fact that they are surrounded by a well-defined mantle of lymphocytes
Lymphoma
●
Clonal malignant disorders that
are derived from lymphoid cells:
either precursor or mature T-
cell or B-cell
●
Majority are of B- cell origin
●
Divided into 2 main types :
1.
Hodgkin’s lymphoma
2.
Non -
Hodgkin’s lymphoma
Etiology
●
Infection
–
EBV
●
Environmental factors
REAL* Classification
Classic :
●
Nodular Sclerosis
●
Lymhocyte rich
●
Mixed Cellularity
●
Lymhocyte depleted
Non-Classic
●
Nodular Lymphocyte predominant
*
REAL – Revised European,American,lymphoma
Hodgkin Lymphoma
Nodular lymphocyte-predominant Hodgkin lymphoma
Classical Hodgkin lymphoma
•
Nodular sclerosis classical Hodgkin lymphoma
•
Lymphocyte-rich classical Hodgkin lymphoma

•
Mixed cellularity classical Hodgkin lymphoma
•
Lymphocyte-depleted classical Hodgkin lymphoma
The etiology of Hodgkin's lymphoma remains unknown ,but there is considerable evidence
to suggest that the EBV plays an important role
Clinical features
●
Bimodal age distribution :
●
young adults
(20-30 yrs) & elderly (
>50 yrs)
M
ay occur at any age
●
M
>
F
●
Lymphadenopathy
:
●
most often cervical region
●
asymmetrical, discrete
●
painless, non-tender
●
elastic character on palpation)rubbery)
●
not adherent to skin
●
fluctuate in size
●
Constitutional symptoms
(
B symptoms )
●
Night sweats ,
●
sustained fever >38 degree celsius ,
●
loss of weight > 10% of body weight in 6 mo
●
Fever sometimes cyclical
)
Pel-Ebstein fever ’ (
●
Pain at the site of disease after drinking alcohol
●
Pallor
●
Pruritis
●
Symptoms of Bulky( > 10 CM) disease
Gross features
lymph nodes involved by Hodgkin's lymphoma are enlarged, sometimes massively so .
The gross appearance depends on the microscopic subtypes the consistency varies from soft
to hard depending on the amount of fibrosis . Some degree of nodularity is often appreciated,
particularly in the nodular sclerosis Foci of necrosis may be present the cut surface of the
node has a more heterogeneous appearance than most non-Hodgkin's lymphoma .
in
advanced cases, several nodes from the same group become matted together
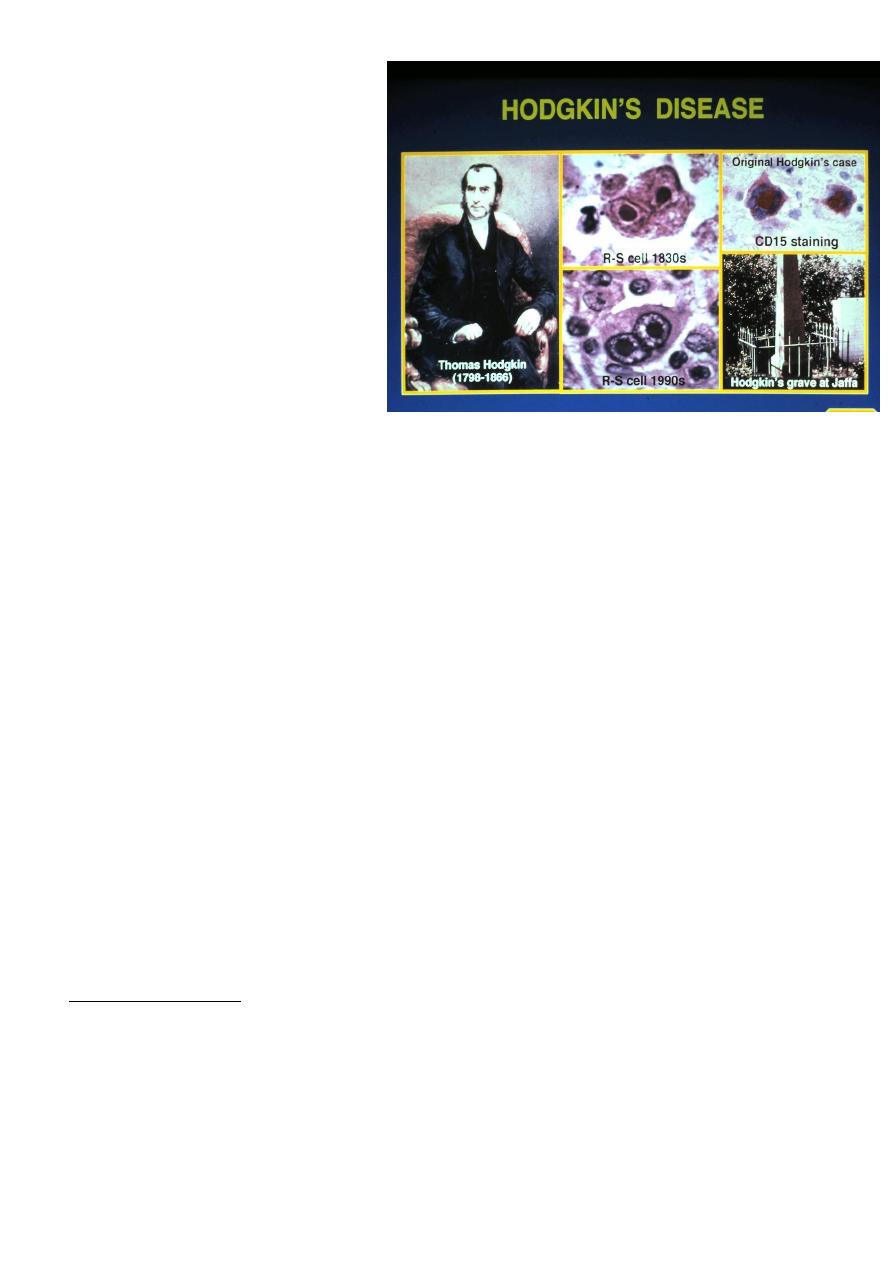
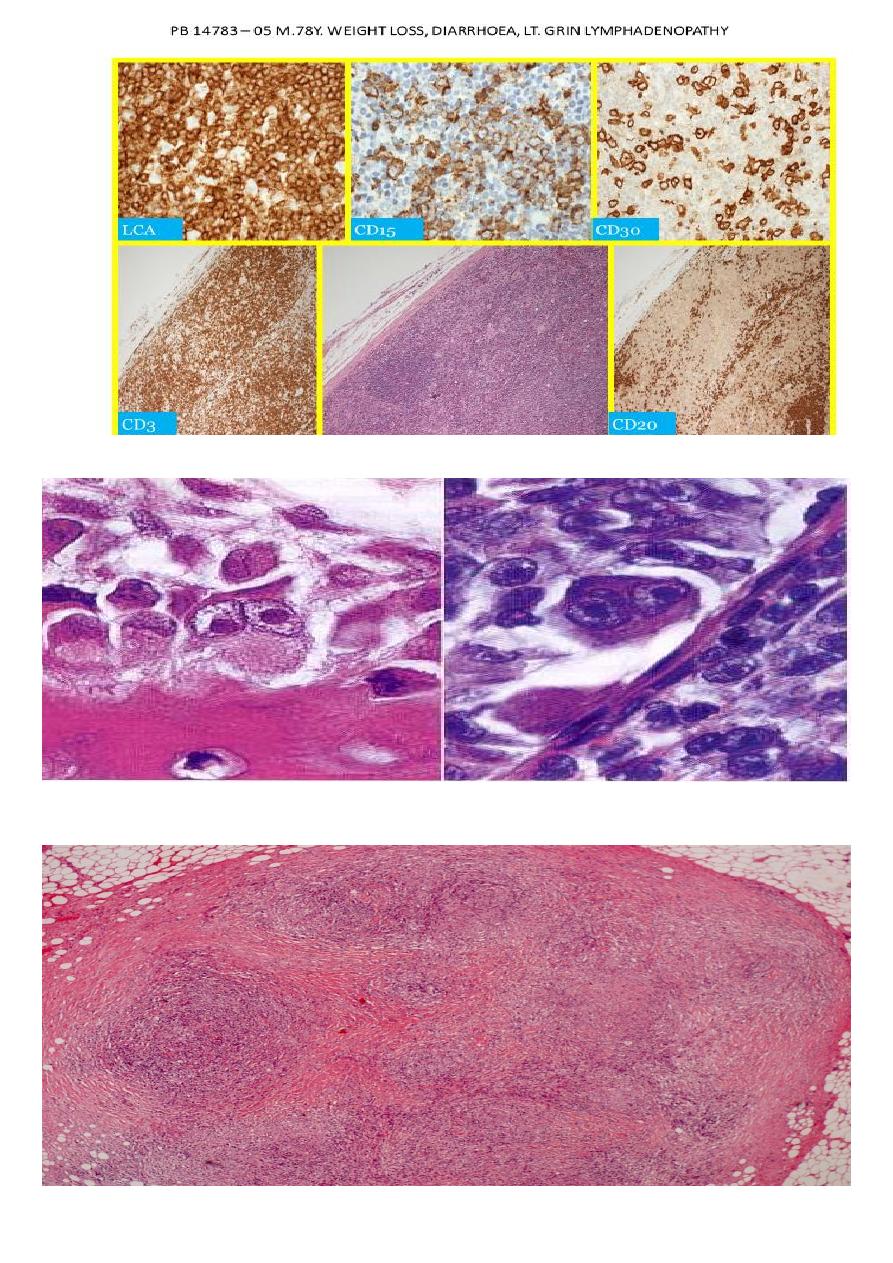
Reed-Sternberg cell
The classic Reed-Sternberg cell, as seen in all
subtypes of
classical Hodgkin's lymphoma, but not in NLPHL,
most important immunocytochemical profile of the Reed-
Sternberg cell is
• .
CD15
(
Leu-Ml :)
This is expressed in over 80% of the cases ;the pattern may be
paranuclear (corresponding to the Golgi region), diffuse cytoplasmic, and/or
corresponding to the cell membrane .
• .
CD30 (Ki-1) :
As recqgnized by the monoclonal antibody Be-Hz ,this is found in
approximately 90% of the cases . ,
• .CD45 (1CA) :This is expressed in less than 10% of the cases .
• .
CD40
(
a protein present in B cells and nerve growth factor receptor): This is expressed
in approximately 70% .
• .
CD74
:
This is e~pressed i ~over 75% .
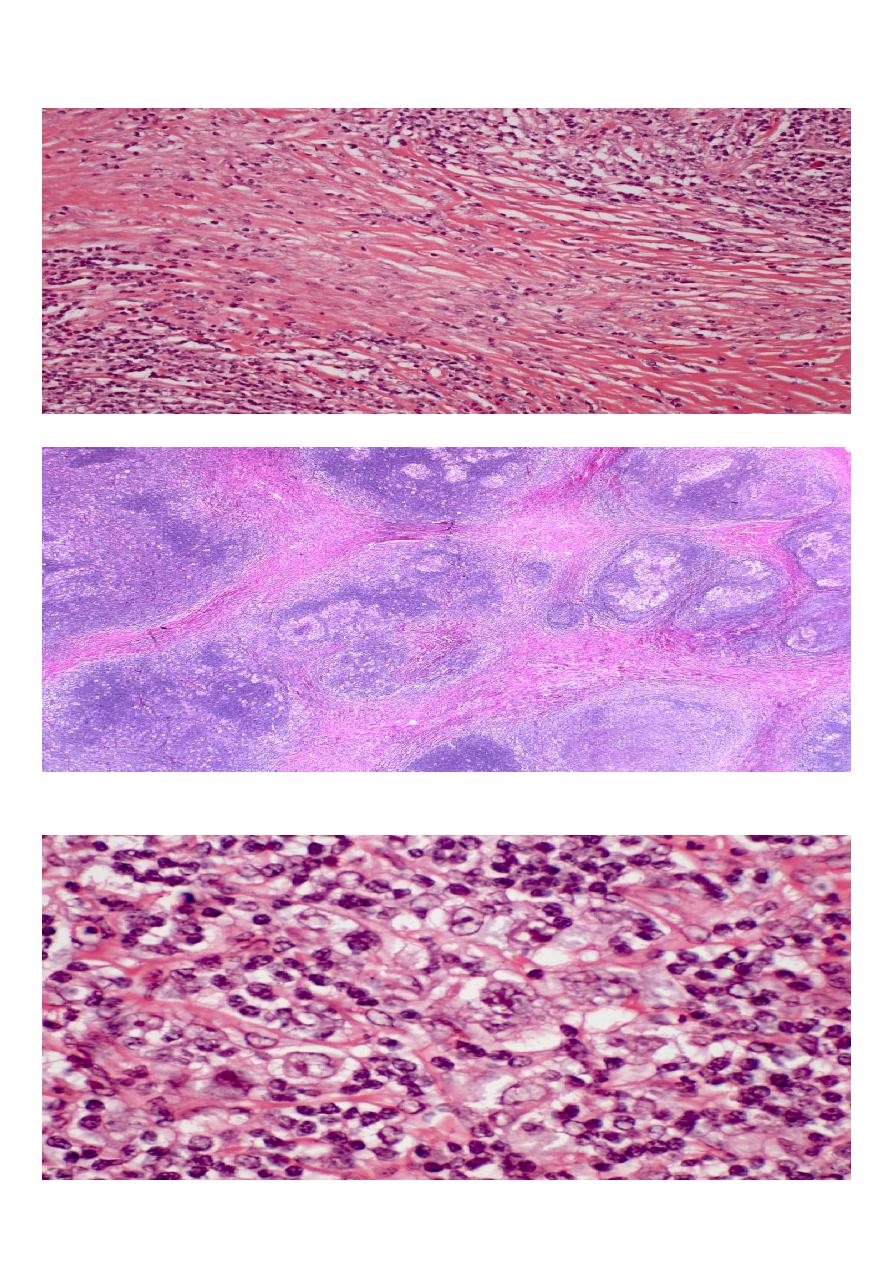
Hodgkin's Histologic subtypes
•
Are characteristic patterns of involvement, and characteristic variants of Reed
Sternberg cell associated with different subtypes
•
Nodular sclerosing HL
•
Most common type Hodgkin's lymphoma in US/Europe
•
Usually presents in the anterior mediastinum and neck of young adult females
•
Characterized by fibrotic capsule and bands subdividing tissue and
•
Lacunar variant Reed Sternberg cell
Histologic subtypes 2
•
Lymphocyte predominant
•
Usually presents with limited disease in the neck of young adults
•
Associated with L and H (lymphocytic and histiocytic) or
"
popcorn cell "variant RS
cell
•
Mixed cellularity
•
More extensive disease
•
Older patients than NS and LP
•
More R-S cells, eosinophils, plasma cells
•
Mononuclear variant R-S cells
•
Inherently more aggressive disease
•
Lymphocyte depleted
•
Often presents in retroperitoneum ,older patients
•
Accompanied by loss lymphocytes ,sclerosis and pleomorphic RS cell variants
•
Also more aggressive disease
General and clinical features
Hodgkin's lymphoma comprises approximatel 20% to30% of all malignant lymphomas in the
United Statesand Western Europe but a much lower percentage inJapan and other Oriental
countries .
with a peak at 15 to 40 years and a second, smaller peak in the seventh decade.
In poorly developed countries, there is a high incidence in children, a relatively low incidence
in the 15- to 40-year age group ,
•
The is a male predominent (approximately 1.5 to 1) in all microscopic types except
nodular sclerosis
• .
The disease may present in a variety of ways
•
the most common (approximately 90% of the cases) being painless enlargement of
superficial (usually cervical) lymph node
•
Fever, night sweats, and loss of weight
(
so-called
"
B symptoms "
)
occur in approximately
25% of the cases ;their presence influences the clinical staging
•
Pruritus is also frequent .
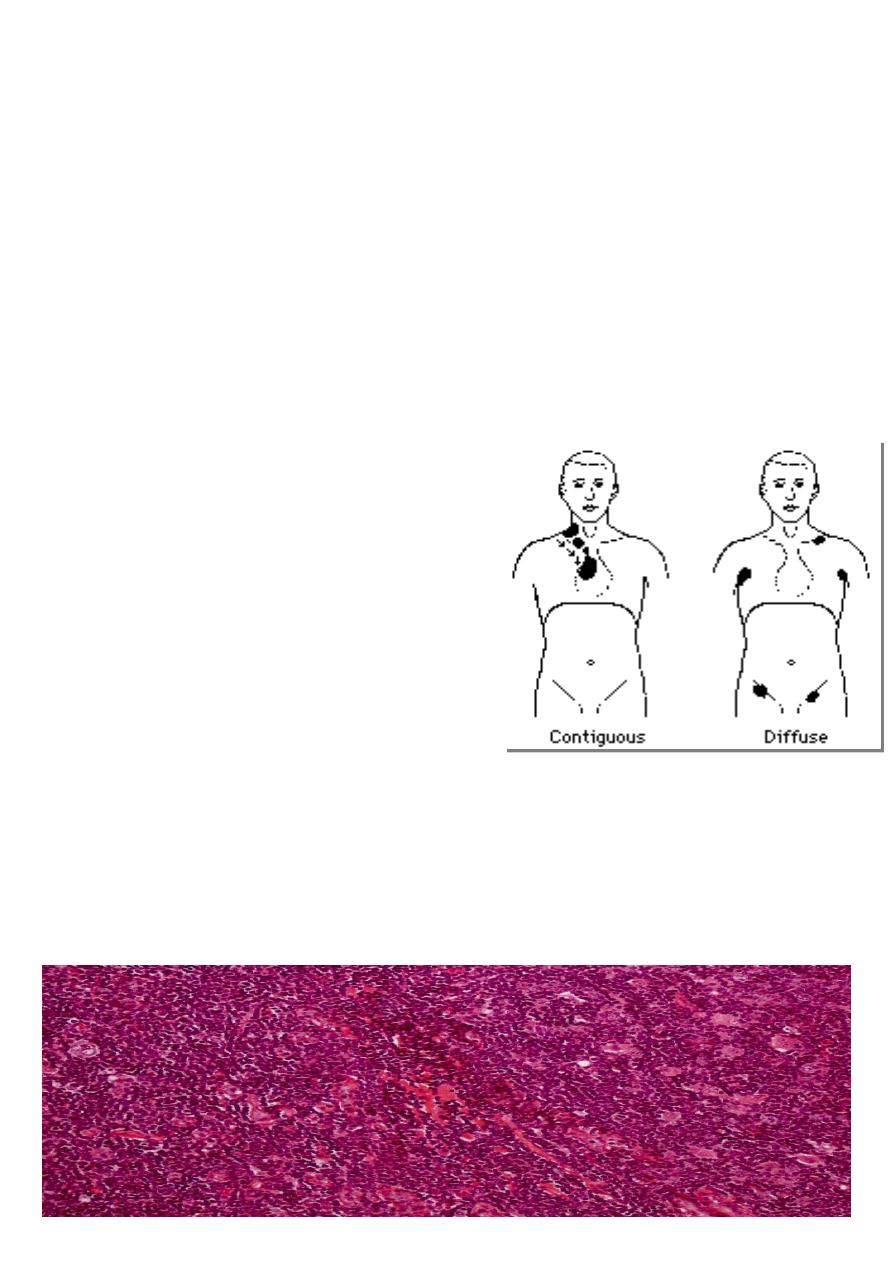
Patterns of spread
•
Hodgkin's lymphoma spreads contiguously
via lymphatics
•
Staging as in NHL- may or may not include
laparotomy/splenectomy
Prognosis
•
Hodgkin's lymphoma is a curable malignancy
•
Overall cure rate approximately 80%
•
With modern therapy, prognosis based more on staging, bulk of disease, than
morphologic subtype
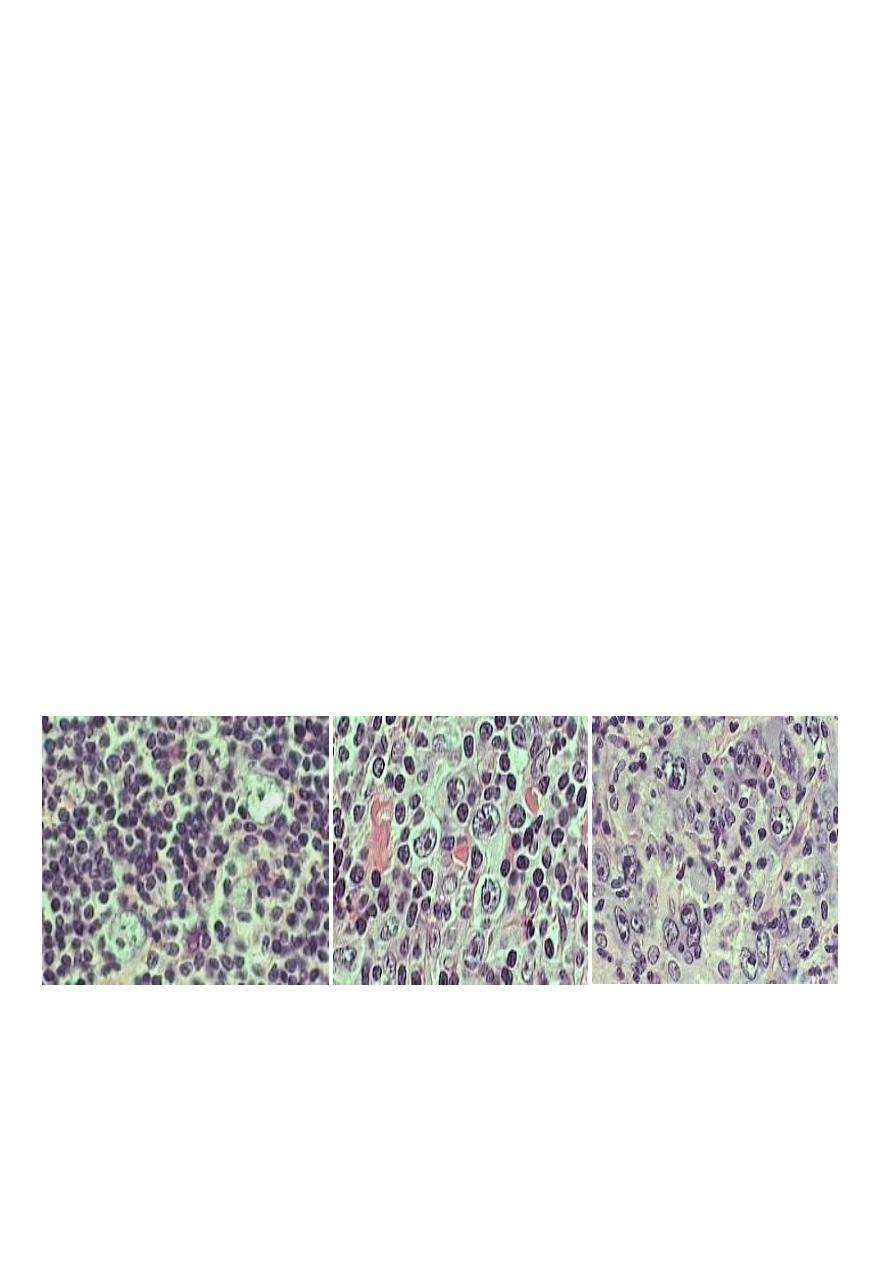
M .63Y. PELVIC AND GROIN LYMPHADENOPATHY
M.57Y .ISOLATED CERVICAL LYMPHADENOPATHY
M.57Y .ISOLATED CERVICAL LYMPHADENOPATHY
F.41Y.CERVICAL LYMPHADEOPATHY AND SPLEENOMEGALY
M. 39Y. PARA AORTIC, MESENTRIC LYMPHADEOPATHY,ANAEMIA,LETHARGY, NODE BIOPSY
M. 39Y. PARA AORTIC, MESENTRIC LYMPHADEOPATHY,ANAEMIA,LETHARGY, NODE BIOPSY
M. 39Y. PARA AORTIC, MESENTRIC LYMPHADEOPATHY,ANAEMIA,LETHARGY, NODE BIOPSY
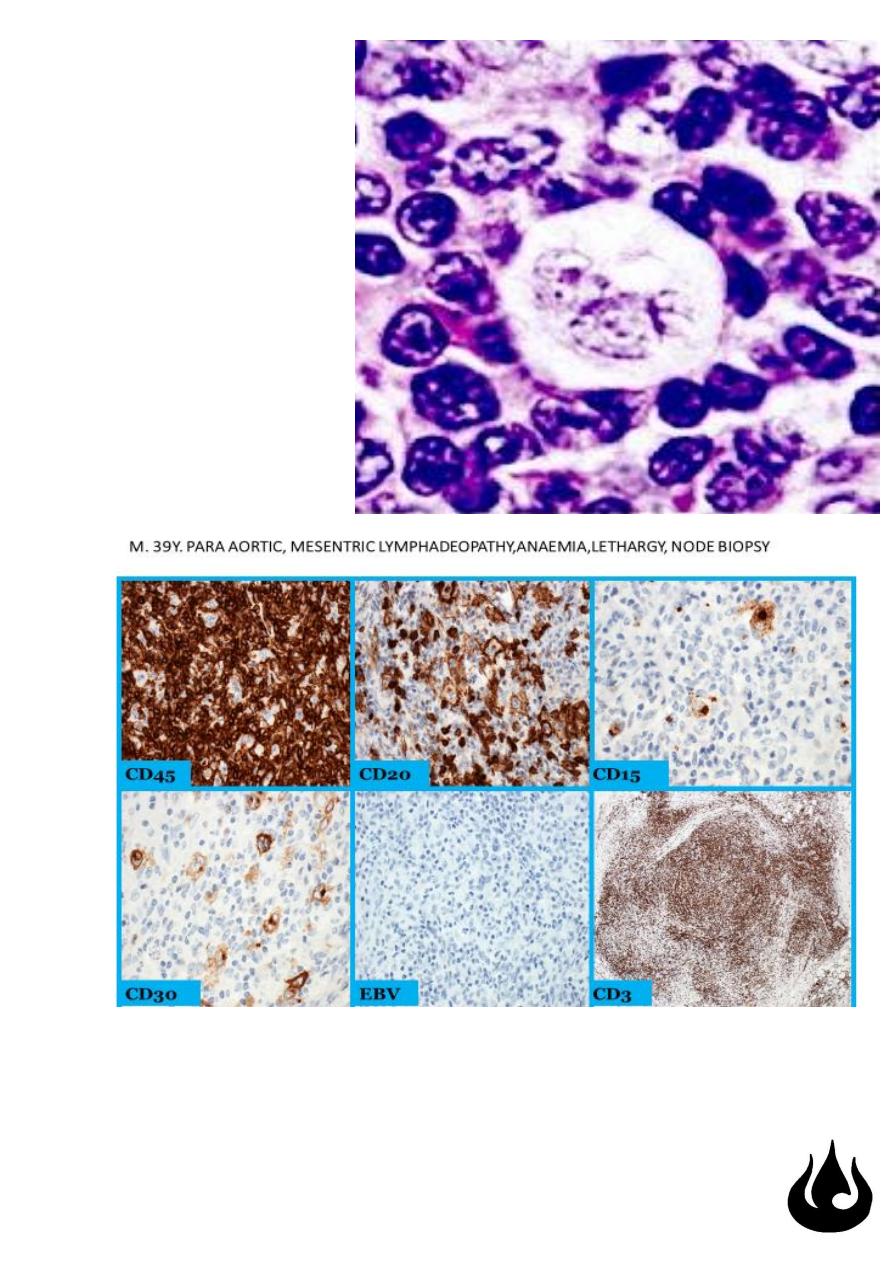
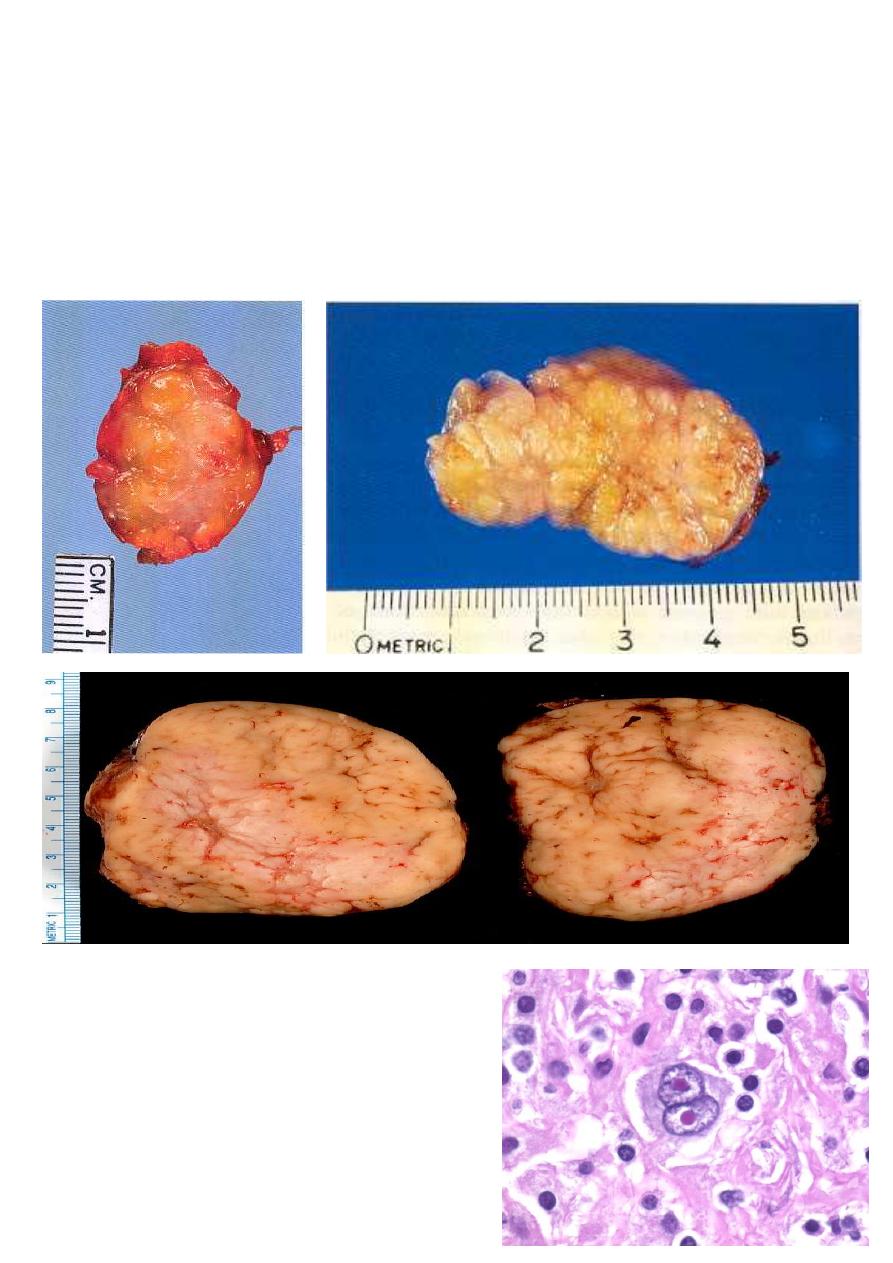
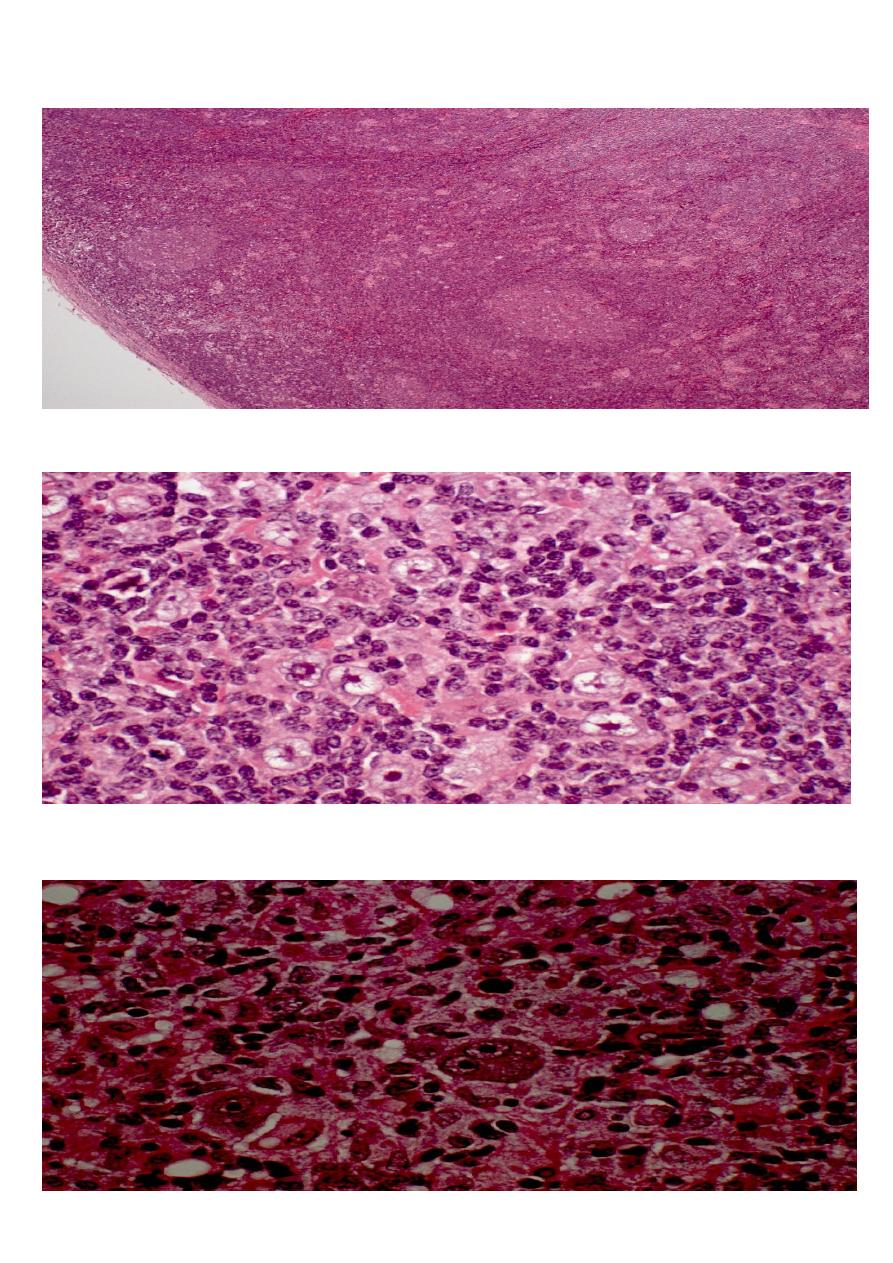
Hodgkin's disease, nodular
sclerosis type, lacunar cell HP mic
large cells with a surrounding
prominent clear space, an artefact
of formalin fixation. These are the
lacunar cells characteristic for the
nodular sclerosis type of Hodgkin's
disease .