
~ 1 ~
Vesicoureteral reflux
Represents the retrograde flow of the urine from the bladder to
the upper urinary tract.
normally there is a functional VUJ valve prevent VUR and thus
protect kidney from infection and high pressure (hydronephrosis )
The phenomenon of VUR represent balance of several factors
include:
• Functional integrity of the ureter
• Anatomic composition of the UVJ
• Bladder compliance
the ureter pass obliquely through bladder wall for 1-
2cm,normally ratio of intera mural ureteric length to ureteric
diameter is 5:1 for that reason if ureter insertion more lateral
more superior it have inadequate muscular support
A. Primary reflux
Is result from congenital abnormality of the UVJ usually involving
longitudinal muscle of intramural ureter
B –secondary reflux
either anatomic or functional
anatomic cause like:
• Posterior urethral valve
• Ectopic ureteral orifices
~ 2 ~
• Ureterocele
Functional. Like:
-neurogenic bladder &
-bladder instability or dysfunction.
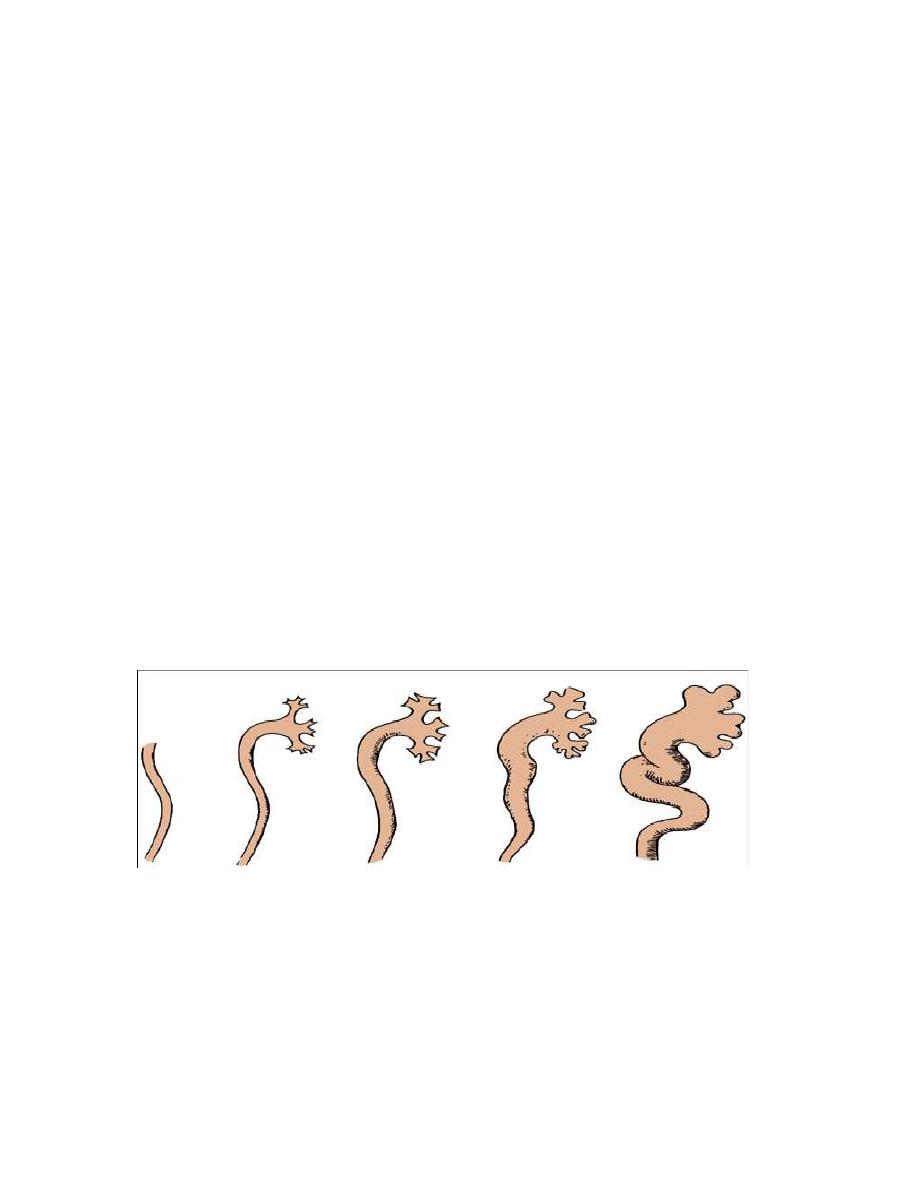
Grading of vesicoureteral reflux
Grade 1 reflux into the non dilated ureter.
Grade 2 into the pelvis & calyces without dilatation.
Grade 3 mild dilatation of the ureter renal pelvis &
calyces.
Grade 4 moderate dilatation of the ureter pelvis &
calyces.
Grade 5 gross dilatation of ureter, pelvis & calyces
.
Demography
• Prevalence:
It approximately 30%in children with UTI and 17% with out UTI.

~ 3 ~
• Gender:
During the 1
st
year most are boys with posterior urethral valves
after 1year the female: male ratio of infection with reflux is
approximately 3-4:1
• Rase:
10 time more in female children of African descent
• Inheritance : autosomal dominant
Diagnosis:
1. Clinical findings
Symptoms related to reflux
• Symptomatic pyelonephritis
• Symptom of cystitis
• Renal pain on voiding
• Uraemia
• Hypertension
Symptoms related to underlying disease
• Urinary tract obstruction
• Spinal cord disease
• 2- physical findings
• During attack of acute pyelonephritis renal tenderness

~ 4 ~
• Palpation and percussion of suprapubic area may reveal
distended bladder
• 3-Lab.finding
•
Infection,bacteriuria,pyuria,high serum creatinine
Therefore a urine culture should be included in the evaluation of
any infant or child who presents with fever & malaise
When reflux has gone undetected & renal scarring has occurred
children of any age can present with
• renal insufficiency,
• hypertension, &
• impaired somatic growth.
Complication of reflux
• Pyelonephritis
~ 5 ~
Hydroureteronephrosis
x-Ray finding
Plain film may reveal evidence of spina bifida or
meningomyelocele thus point to the neurologic deficit.
Excretory urograms may be
-normal, or -dilatation of whole or part of ureter or
-hydroureteronephrosis
Reflux is diagnosed by
voiding cystourethrography or
voiding cinefluoroscopy
Cystoscopy.
For
~ 6 ~
• Morphology (stadium or horseshoe or golf hole orifice)
• Position.
Treatment: medical
Maintaining urinary sterility by using single daily low dose
antimicrobial prophylaxis
Night time dosing allow to cover period of physiological retention
If child have infected urine then gave high dose antibiotic to
sterile the urine then continuo on low dose antibiotic
Antibiotic
Age less than 2 months we commonly use trimethoprin and
amoxicillin
After 2 months antibiotic of choice is trimethoprin-
sulfamethoxazole
Then follow up every 3 months by uls and urine cultures and some
time need yearly radionuleotide scanning
*In toilet trained children bladder emptying by timed voids,
double voiding, help to achieve the goals of medical management.
B-Surgery (ureteric Reimplantion)
Typical indication of antireflux surgery include:-

~ 7 ~
1- breakthrough UTI despite prophylactic antibiotic.
2- noncompliance with medical management.
3- sever reflux grade 4 or 5.
4- failure of renal growth, new scars, or deterioration of renal
function on follow up ultrasound.
5- reflux persist to puberty specially in girls.
6- reflux associated with congenital abnormalities such as bladder
diverticulum
MEGAURETER
It mean a dilated ureter ,normally ureteric diameter about 5mm if
it accede 7-8mm then it consider MGUs
Classification
a megaureter may be obstructed, refluxing, both refluxing and
obstructed, or unobstructed and not refluxing, either from a
primary (idiopathic cause intrinsic to the ureter or secondary to
specific pathophysiologic processes, such as outlet obstruction,
neurogenic dysfunction, polyuria, or infection).
Primary (at the UVJ; adynamic aprstalitic segment) or
secondary (e.g.,bladder malfunction) origins influence
management and must therefore be differentiated.

~ 8 ~
Indications for correction are often driven by serially
increasing pelvicalyceal dilation, increasing ureteral
diameter, or pyelonephritis and ureteral pyuria.
Antibiotic prophylaxis should be used to protect the dilated
ureter regardless of cause.
Many cases of antenatally diagnosed MGU will resolve
spontaneously.If there is improvement in degree of
hydroureteronephrosis, but not resolution, imaging at
puberty is advised.
Good lock