I
Extraction in Orthodontics
Most extractions are performed as part of a general plan of treatment
which also involves the use of appliances. The age of the patient and the nature
of the malocclusion may be important factors in deciding whether or not to
employ extractions. The duration of orthodontic treatment, an important
psychological factor, should always be as short as possible and may influence
the age at which extractions are performed. By careful timing of extractions it
is often possible to facilitate spontaneous migration of adjacent teeth as they
erupt.
It is fairly generally accepted in current orthodontic practice that if the
jaws are not large enough to accommodate the dentition, there is no satisfactory
alternative to extraction
.
Before extractions are considered, an exhaustive study of the case must
be made by a clinical and radiographic examination of the patient, paying
particular attention to caries or heavily filled or traumatized teeth which might
subsequently give rise to symptoms
.
Reasons for extracting teeth as part of orthodontic treatment
There are several factors which justify the extraction of teeth as part of
orthodontic treatment and these may serve as guiding principles:
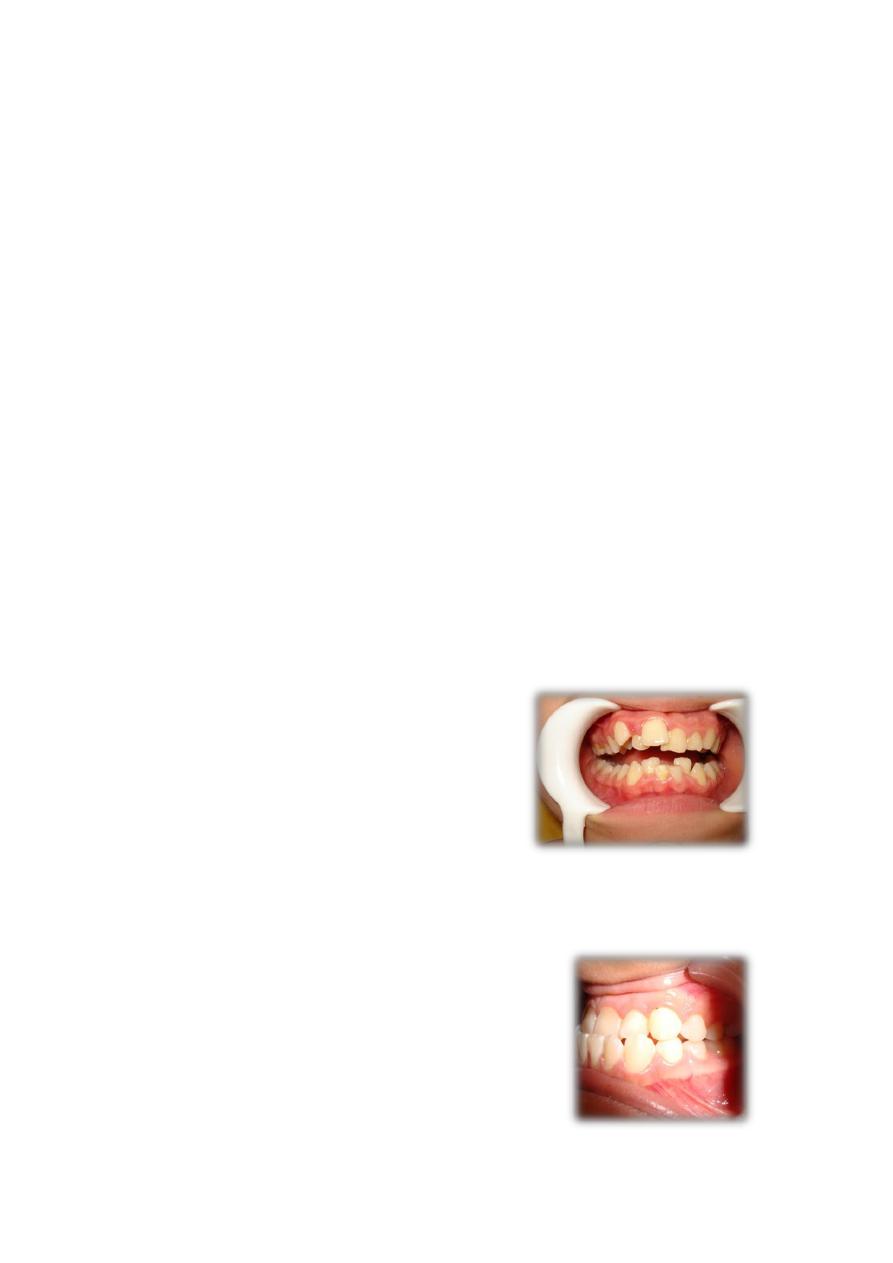
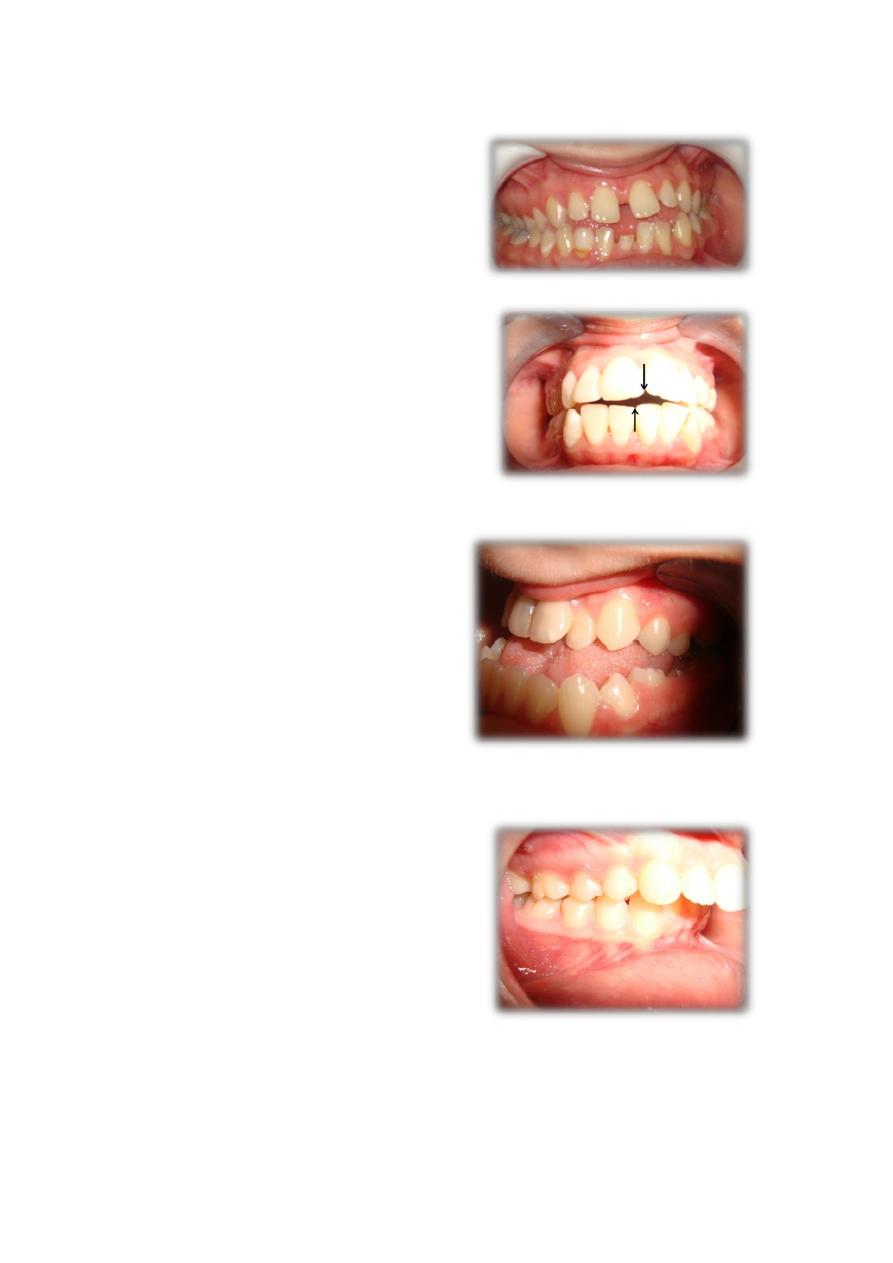
1. Disproportion between tooth and arch size. Disproportion in size between
the alveolar processes and the teeth may give rise to crowding.
2. Malrelation between arches. It is possible to select teeth for extraction in
such a way that the aesthetic appearance and functional efficiency may be
improved in some Angle Class II and Class III cases
II
3. Abnormal form and size of individual teeth.
4. Preservation of symmetry or correction of asymmetry.
5. Extreme jaw relations. In some cases teeth may require extraction as a part
of surgical correction of the jaws (orthognathic surgery).
6. Late treatment (adult patients).

III
Indications of individual tooth extraction
Incisors:
Maxillary Incisors
The incisors, especially the maxillary central incisors, are rarely extracted as a
part of orthodontic therapy.
Indications for maxillary incisor extraction
a. Unfavorably impacted maxillary incisors.
b. Buccally or lingualy blocked out lateral incisor with good contact between
central incisor and canines.
c. Grossly carious incisor that cannot be restored.
d. Trauma/irreparable damage to incisors by fracture.
Mandibular Incisors
In a few well-defined cases, extraction of lower incisors may be
appropriate:
a. When one incisor is completely excluded from the arch and there are
satisfactory approximal contacts between other incisors .
b. Poor prognosis as in case of trauma, caries, bone loss, etc.
c. Severely malpositioned incisor.
d. In mild Class III incisor relation with an acceptable upper arch and lower
incisor crowding, a lower incisor may be extracted to achieve normal overjet,
overbite and to relieve crowding.
Canines:
Because of their position in the cornerstone of the dental arch,
canines are only considered for extraction if they are severely displaced
and/or crowded out of the arch.
a. Mandibular canine may be extracted when it is likely to be very difficult
to align, e.g. when it is excluded from the arch and the apex is severely
malpositioned or when it is unfavorably impacted.
b. Maxillary canines develop far away from their final location and have a
long path of eruption from their development site to their final position in
the oral cavity. Therefore, they are not uncommonly impacted or ectopic
and their alignment is difficult, even impossible. Extraction may be
required in such cases.
c. When maxillary canine is completely excluded from the arch and
approximal contact between lateral incisor and first premolar is good,
extraction of the canine may be considered
First premolars:
It is the tooth most commonly extracted as part of orthodontic therapy
especially for the relief of crowding because:
• It is positioned near the center of each quadrant of the arch and is therefore
near the site of crowding, i.e. the space gained by their extraction can be
utilized for correction both in the anterior and posterior region.
• First premolar extraction is the least likely to upset molar occlusion and is the
best alternative to maintain vertical dimension.

IV
• The contact between the canine and second premolar is satisfactory.
• First premolar extraction leaves behind a posterior segment that offers
adequate anchorage.
Indications:
1.
Tooth of choice for extraction to relieve moderate to severe anterior
crowding in both arches. In lower arch crowding, where canines are mesially
inclined, spontaneous improvement in incisor alignment will follow.
2. Correction of moderate to severe anterior proclination as in Class II div 1 or
Class I bimaxillary protrusion.
3. In high anchorage cases, first premolars take precedence over second
premolars as the teeth to be extracted.
4. As a part of serial extraction.
Second premolars:
The extraction of second premolars provides rather less space to the
incisor region since a greater proportion of that made available is lost to the
molars. This is 'of advantage' where only a small amount of space is required
anteriorly
.
Indications:
1. When second premolar is completely excluded from the arch following
forwards drift of first molar after early loss of deciduous second molar.
2. Second premolar extraction is preferred in mild anterior crowding cases as
space closure and vertical control is easier after anterior alignment. The
presence of first premolar anterior to extraction site strengthens the anterior
anchorage, thereby facilitating closure from behind.
3. Second premolar extraction is preferred when one wishes to maintain soft
tissue profile and esthetics.
4. Unfavorably impacted second premolars.
5. Grossly carious or periodontally compromised second premolar
6. In open bite cases second premolar is preferred for extraction as it
encourages deepening of the bite
First Permanent Molars:
As these teeth are particularly susceptible to caries, their early loss is
unfortunately common. This frequently complicates orthodontic treatment.
They may be extracted when beyond repair.
Indications:
1. Minimum space requirement for correction of anterior crowding or mild
proclination
2. Grossly decayed/periodontally compromised molar with poor prognosis.
3. Impacted molar(rarely seen).
Extraction of first molars is avoided because:
• It does not give adequate space to relieve anterior crowding.
• Deepening of bite

V
• Poor approximal contact between second premolar and second molar
• Second premolar and second molar may tip into extraction space
• Mastication is affected
Second permanent molars:
They are extracted if:
1. distal movement of the buccal segments is indicated.
2. when growth is insufficient for normal eruption of the 2nd and/or 3rd
molars.
Their extraction is contraindicated when;
1. upper 3rd molars are too high or show delayed eruption.
2. poor angulation of the 3rd molars.
3. 3rd molars of small size.
4. absence of the 3rd molars.
Third permanent molars:
Impacted 3
rd
molars that show evidence of interfering with treatment or
retention, or are the cause of reflex pain or infection, should be extracted.
Prophylactic extraction of the third molars in orthodontics is a matter of
continuous debate up till now.