1
DR.JAMAL AL-SAIDY
M.B.CH.B…F.I.C.M.S
FRACTURED SCAPHOID
Scaphoid fractures account for almost 75 per cent of all carpal fractures although
they are rare in the elderly and in children.
With unstable fractures there may also be disruption of the scapho-lunate
ligaments and dorsal rotation of the lunate.
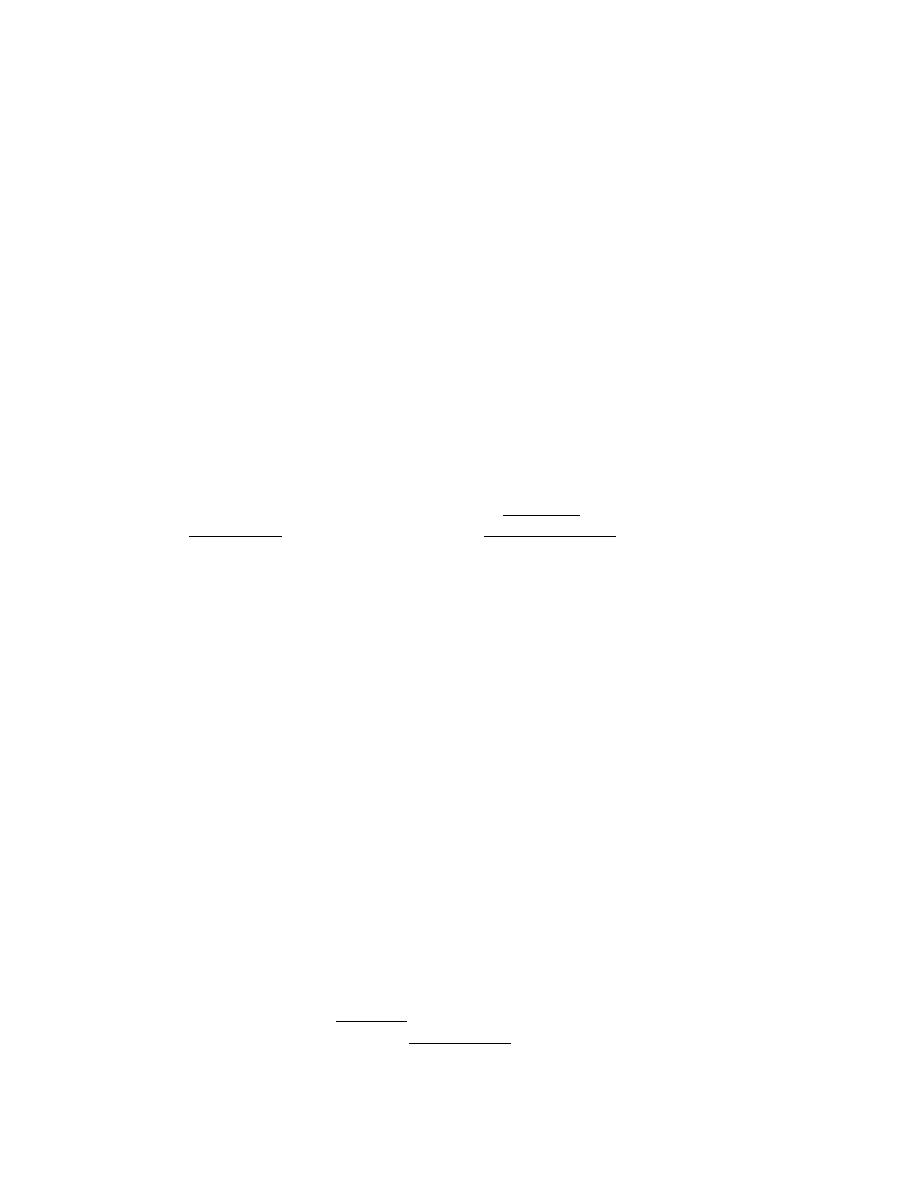
Mechanism of injury and pathological anatomy
The scaphoid lies obliquely across the two rows of carpal bones, and is also in the
line of loading between the thumb and forearm.
The combination of forced carpal movement and compression, as in a fall on the
dorsiflexed hand, exerts severe stress on the bone and it is liable to fracture.
Most scaphoid fractures are stable; with unstable fractures the fragments may
become displaced.
The distal fragment, unrestrained by the scapho-lunate ligament, flexes and the
proximal fragment tilts dorsally with the lunate (a DISI deformity.
The blood supply of the scaphoid diminishes proximally.
This accounts for the fact that 1 per cent of distal third fractures, 20 per cent of
middle third fractures and 40 per cent of proximal fractures result in non-union or
avascular necrosis of the proximal fragment.
Clinical features
The appearance may be deceptively normal, but the astute observer can usually
detect fullness in the anatomical snuffbox; precisely localized tenderness in the
same place is an important diagnostic sign; the scaphoid can of course also be
palpated from the front and back of the wrist and it may be tender there as well.
Proximal pressure along the axis of the thumb may be painful.
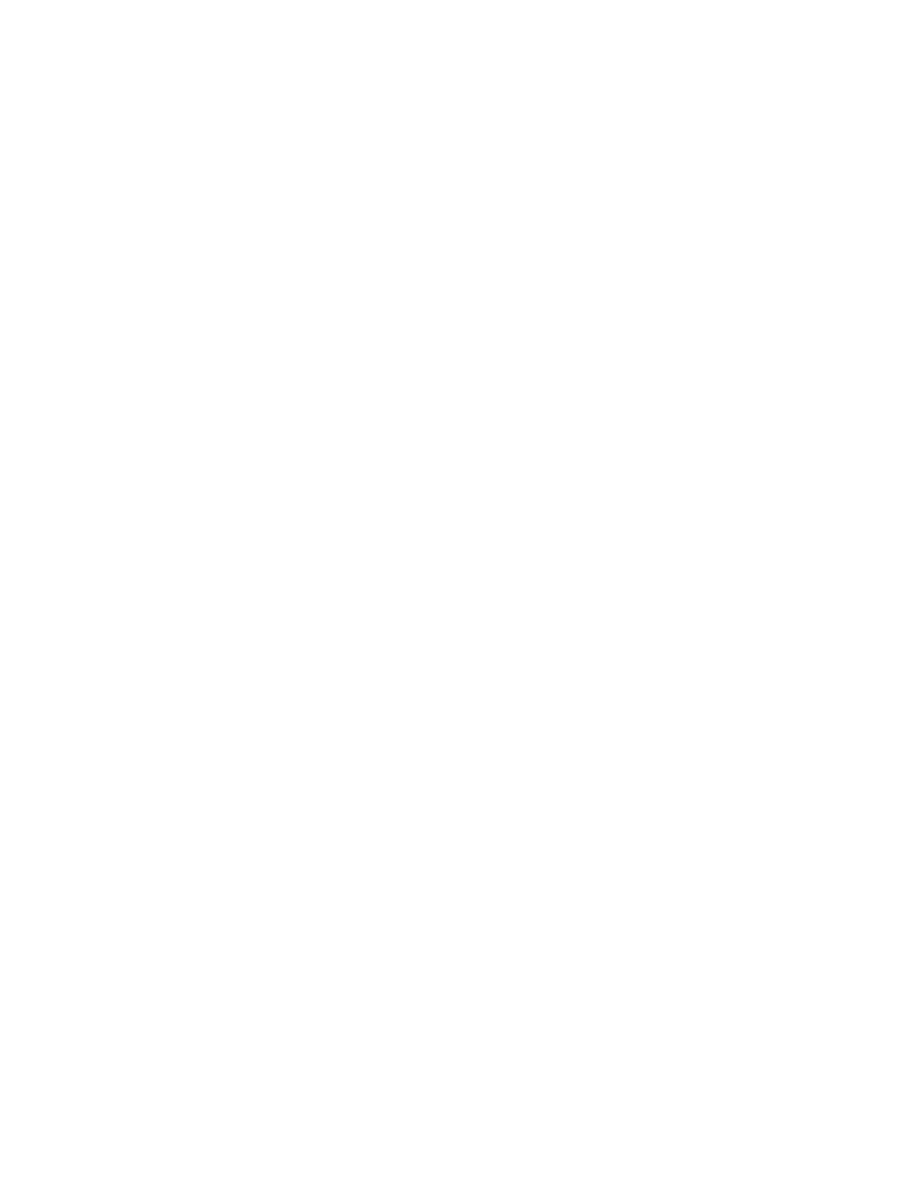
X-ray
Anteroposterior, lateral and oblique views are all essential; often a recent fracture
shows only in the oblique view.
Usually the fracture line is transverse, and through the narrowest part of the bone
(waist), but it may be more proximally situated (proximal pole fracture).
Sometimes only the tubercle of the scaphoid is fractured.
It is very important to look for subtle signs of displacement or instability:
e.g.:-
o obliquity of the fracture line,
o opening of the fracture line,
o angulation of the distal fragment and
o foreshortening of the scaphoid image.
A few weeks after the injury the fracture may be more obvious;
if union is delayed, cavitation appears on either side of the break.
Old, un-united fractures have ‘hard’ borders, making it seem as if there is an
extra carpal bone.

2
DR.JAMAL AL-SAIDY
M.B.CH.B…F.I.C.M.S
Relative sclerosis of the proximal fragment is pathognomonic of avascular
necrosis.
Treatment
Fracture of the scaphoid tubercle needs no splintage and should be treated as a
wrist sprain; a crepe bandage is applied and movement is encouraged.
Other scaphoid fractures are treated as follows:-
Undisplaced fractures :
need no reduction and are treated in plaster; 90 per cent of
waist fractures should heal.
The cast is applied from the upper forearm to just short of the
metacarpo-phalangeal joints of the fingers, but incorporating
the proximal phalanx of the thumb. The wrist is held
dorsiflexed and the thumb forwards in the ‘glass-holding’
position. The plaster must be carefully moulded into the hollow
of the hand, and is not split. It is retained (and if necessary
repaired or renewed) for 8 weeks.
After 8 weeks the plaster is removed and the wrist examined
clinically and radiologically.
If there is no tenderness and the x-ray shows signs of healing,
the wrist is left free; a CT scan is the most reliable means of
confirming union if in doubt.
If the scaphoid is tender, or the fracture still visible on x-ray,
the cast is reapplied for a further 4 weeks. At that stage, one of
two pictures may emerge:
(a) the wrist is painless and the fracture has healed – the
cast can be discarded;
(b) the x-ray shows signs of delayed healing (bone
resorption and cavitation around the fracture) – union
can be hastened by bone grafting and internal fixation.
Displaced fractures
can also be treated in plaster, but the outcome is less
predictable.
It is better to reduce the fracture openly and to fix it with a
compression screw. This should increase the likelihood of
union and reduce the time of immobilization.
Some patients may not want to endure a prolonged period in
plaster.
Early percutaneous fixation with a compression screw, though
technically demanding, can dramatically reduce the time away
from work and the difficulties associated with personal care.
Complications
Avascular necrosis The proximal fragment may die, especially with proximal pole
fractures, and then at 2– 3 months it appears dense on x-ray.
3
DR.JAMAL AL-SAIDY
M.B.CH.B…F.I.C.M.S
Non-union By 3 months it may be obvious that the fracture will not unite. Bone
grafting should be attempted, especially in the younger, more vigorous type of
patient, because this probably reduces the chance of later, symptomatic
osteoarthritis. In older patients, and those who are completely asymptomatic,
non-union may be left untreated.
Osteoarthritis Non-union or avascular necrosis may lead to secondary
osteoarthritis of the wrist.
THANK YOU
DR.JAMAL AL-SAIDY
M.B.CH.B..…… F.I.C.M.S