
Fasciola hepatica
Adult Egg
Fasciola hepatica Linnaeus, 1758 was the first trematode to be described (de brie,
1379). It is particularly prevalent in sheep- raising areas. In several countries
human infection is an increasing clinical and public health problem.

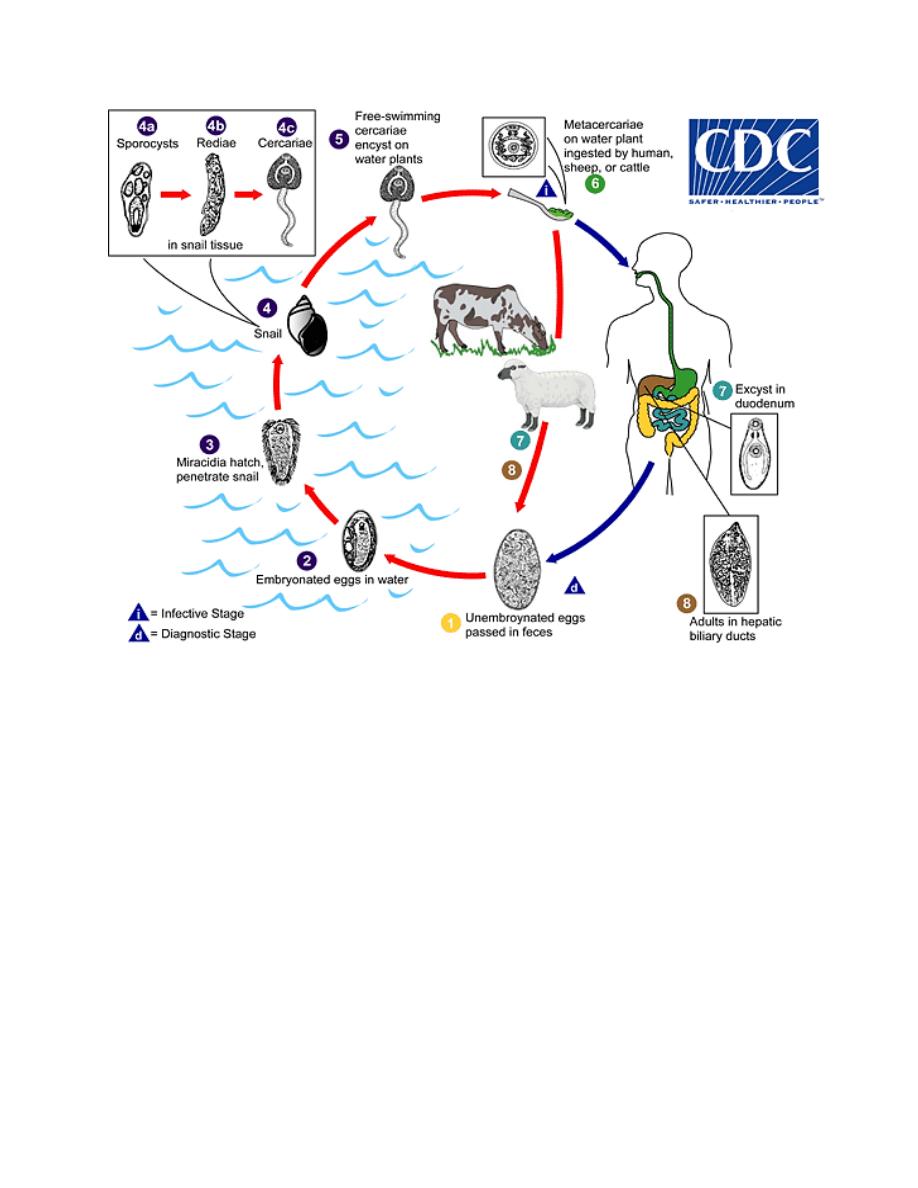
Morphology, Biology and life cycle.
The mature Fasciola hepatica is a relatively large worm, measuring up to 30 by 13
mm. It is more or less flattened and leaf-like along the margins, fleshy throughout
the middle. F. hepatica adults reside typically in bile passages and gall bladder.
Occasionally they fail to reach this location and are found ectopically in the
peritoneal cavity or other sites. The eggs are unembryonated when expelled. They
pass from the common bile duct into the duodenum and intestinal tract of the host,
to be evacuated in the stools. These eggs are large (130 to 150 microns by 63 to 90
microns), relatively thin-shelled, and have a small, flat operculum at one end. They
require 9 to 15 days to mature in fresh water at an optimum temperature of 22° to
25°C. Upon hatching, the miracidium invades a lymnaeid snail (Lymnaea
truncatula), enters the tissues and transforms into a sporocyst within 30 days,
second and third generation rediae and cercariae have been produced. Then the
cercariae swam out of the snail, and after crawling upon moist vegetation shed
their tail, round up and encyst as minute spherules (metacercariae). These cysts
survive for a considerable time in a moist atmosphere. When viable cysts ingested
by human, reach the duodenal or jejunal level of the intestine, they excyst and the
metacercariae actively burrow through the intestinal wall, migrate across the
peritoneal cavity to the liver, then eat their way as they burrow through the hepatic
parenchyma to the bile ducts, where they develop into adults in 3 to 4 months after
exposure. They feed on the tissues through which they pass, only incidentally
consuming extravasated blood.
Pathogenicity and symptomatology
The migration of young Fasciola hepatica en route through the parenchyma to the
bile ducts cause both traumatic damage and toxic irritation with necrosis of tissue
along their pathway. In the bile passages, they produce hyperplasia of the biliary
epithelium, with leukocyte infiltration and development of a fibrous capsule
around the ducts. Early symptoms in human infections consist of right upper
quadrant abdominal pain, fever and hepatomegaly; biliary colic with coughing and
vomiting; marked jaundice; diarrhea; irregular fever; significant eosinophilia. Later
there may be profound systemic toxemia.
False fascioliasis refers to the recovery of the eggs of Fasciola in the stool
following ingestion of infected livers of sheep, goats or cattle, raw or undercooked.

Diagnosis
Most cases of true fascioliasis hepatica are first apprehended by of the eggs in the
patient’s stool. These require differentiation from eggs of Fasciolopsis buski,
which are almost identical in size and appearance. The difficulty may be avoided
by obtaining samples of uncontaminated bile for microscopic examination. In cases
of false fascioliasis, eggs of Fasciola will no longer appear in the feces a few days
after the patient has been placed on a liver-free diet.
Treatment
The recommended treatment options for fascioliasis (liver fluke infection with F.
hepatica or F. gigantica), include triclabendazole which is the drug of choice. The
drug is given by mouth, usually in two doses. Most people respond well to the
treatment. Praziquantel, previously used as an alternative drug is no longer
recommended due to poor efficacy against Fasciola species.
Epidemiology
Human infection is usually due to where eating freshwater cress to which the
metacercarial cysts are attached. Several hundred published human cases in Latin
America, Mediterranean countries, in which the infection is relatively frequent and
clinically important.
Control
Fundamental control requires the institution of measure to eradicate natural
infection in sheep and other herbivorous mammals. Since most human infections
results from use of water cress as salad greens, control of human fascioliasis
hepatica will usually be obtained if this delicacy is omitted from the diet in
endemic areas. Application of the molluscicide has proven effective against the
lymnaeid snail intermediate hosts in several European countries.

Fasciola gigantica
Fasciola gigantica cobbold, 1856, the giant liver fluke, differs from F. hepatica in
its greater length, and larger size of the eggs (160 to 190 microns by 70 to 90
microns). The life cycle parallels that of F .hepatica, including lymnaeid snails
(Radix auricularia) as intermediate hosts. Human infections have been reported
from West Africa, Vietnam,
Uzbekistan
, Iraq, and Hawaii. Clinical aspects of this
infection are essentially the same as in fascioliasis hepatica.