1
Embryology & Anatomy of Genital Tract
It's necessary to understand the embryology of genital tract as both the
urinary and genital tract develop from the common mesodermal ridge running
along the posterior abdominal wall so sometimes the congenital anomalies of
the genital tract is associated with congenital anomalies of urinary tract .
Development of the genital organs:
During the 5
th
week of embryonic life the nephrogenic cord, develop from
mesoderm and form urogenital ridge and mesonephric duct, which form the
wolfian duct later on. While the paramesonephric duct will form later on the
mullerian system (uterus, cervix, fallopian tube).
The fate of this develop depend on the secretion of the gonads.
The mesonephric duct consist of large ovoid organ on each sides with the
developing gonads on the medial side of its lower portion.
Assuming that is female development, the two-paramesonephric duct extend
caudally into urogenital sinus and develop to form the female genital organ
while the wolfian duct degenerate.
The lower third of the mullerian duct come together in the midline, fuse and
develop into uterus and cervix. At first there is a septum and then disappear to
form a single cavity (the uterus).
the lower end of the fused mullarian duct proliferate to form a cord,, then
during the 9
th
week of embryonic life this cord make contact with sinovaginal
bulb and provide for the length to the vagina, while the solid sinovaginal bulb
start to canalize and form the lower part of the vagina, complete canalization
occur at 6
th
or 7
th
month of embryonic life.
Development of external genitalia:
There is overlap in timing of formation of external and internal genitalia but
there is common indifferent stage consist of
Two genital fold labia minor
Two genital swelling labia major
One midline anterior Genital tubercle clitoris
Male --- external genital development depend on the secretion of testosterone
from the gonads and any abnormality in this female development
د. سهى
وتوت
/ نسائية
2
Development of the ovary
The primitive gonad is 1
st
evident in embryonic life at 5
th
weeks
It form as bulb on the medial aspect of the mesonephric ridge, this bulb consist
of:
1- coelomic epithelium
2- underlying mesoderm
3- primitive germ cell
There is proliferation of cells in and beneath the coelomic epithelium
By 5th weeks these cell form the sex cord.
The development of ovary occur 2 weeks later than development of testes
The sex cord develop extensively and the epithelium cells in this area known
as pregranulosa
The next stage of development involve the primitive germ cell now known as
oocyte and surrounded by ring of pregranulosa cell .this germ cell pass into
Mitotic division & then cease & enter the first stage of meiosis & prophase
arrest.
the number of oocyte is greatest before birth and then after decline.
Approximately 7 million germ cell are present during 5
th
months But at birth,
they fallen to 2 million, half of which are atretic
Anatomy
Anatomy of vulva this include mons pubis, labia major, labia minor .vestibule,
clitoris , vestibular gland
The mons pubis consist of fibro fatty tissue, which cover the body of pubic
bone. In adult, the skin of mons bear hair (pubic hair)
Labia major are two fold of skin with underlying adipose Tissue. They contain
sebaceous and sweat gland.
Labia minor are two fold of skin lie below the labia major
Anteriorly, they divide into 2 to form prepuce and frenulum of clitoris
Posteriorly, they fuse to form a fold of skin called the fourchette. They contain
sebaceous gland but not adipose tissue.
3
The clitoris: is small erectile structure, the body of clitoris contain 2 crura and
its rich with nerve supply so it is so sensitive during sexual arousal, its length 1
cm
The vestibule the cleft between the labia minor the urethral opening the
bartholine duct and vaginal open in the vestibule
Bartholin gland: are small gland lie at the base of each vestibule bulb and
these are mucous secreting glands act as a lubricant during intercourse
The hymen: is e thin fold of mucous membrane across the entrance to the
vagina, there is usually opening in it to allow menses to escape
The vagina:
Is a fibro muscular canal lined with stratified squamous epithelium that lead
from the uterus to the vulva. it is longer in the posterior wall (9cm) than
anterior wall (7cm).
The vault of the vagina is divided into 4 fornices, posterior one that is the
largest one, anterior Fornix and 2 lateral.
It kept moist by the secretion of the uterus and cervical canal and transudation
of vaginal wall.
It has no glands.
Its wall is rich with glycogen epically during the postovulatory phase but it little
before puberty and after menopause.
Doderlein's bacilli is a normal flora of the vagina breaking glycogen to form
lactic acid & produce pH of 4.5, which is a protective mechanism, prevent
growth of pathogenic organism.
4
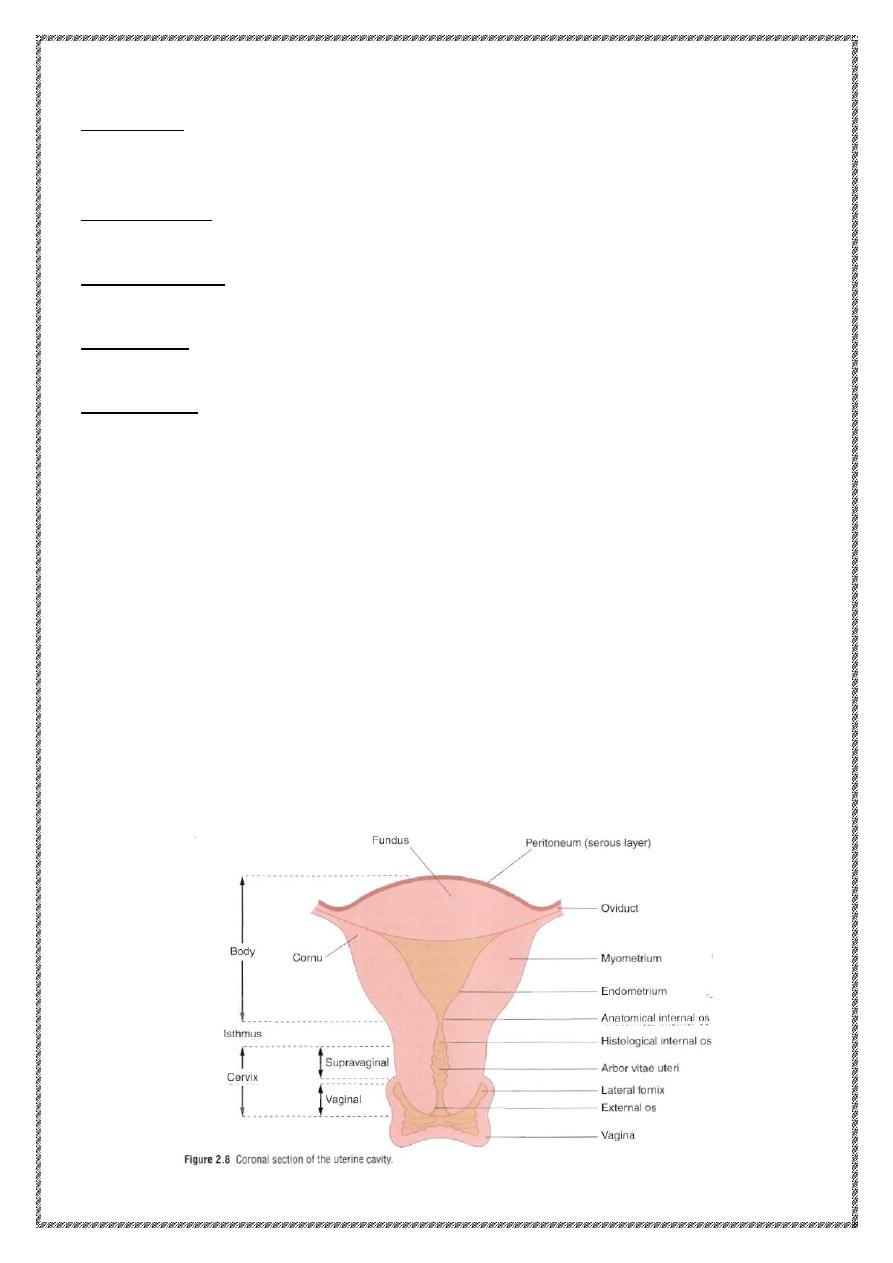
The uterus:
Its shape like an inverted pear & in non-pregnant lady, it completely lie within
the pelvis.
Its hallow structure and thick muscular wall. Its maximum external dimension
are 7.5 cm (length) \ 5 cm (width) \ 3 cm (thick) .in adult weight 70 gm.
The upper part of the uterus is term the body, the one of insertion of fallopian
tube is termed the cornu, the part above the cornu is term the fundus.
The uterus taper to a small constructed area is termed the isthmus below this
is the cervix which project into the vagina and divided into vaginal + supra
vaginal parts.
The area where the Corpus joint the cervix is termed the anatomical internal
os. Histologically where there is epithelial change or the mucous membrane
of the isthmus become that of the Cervix (histological internal os)
The uterus consist of three layers:
1- outer layer (serosa)---- peritoneum
2- middle layer ( muscular) ---myometrium which consist of interlacing
smooth muscle + blood vessels + nerves + lymphatic
3- inner layer (endometrium) covered by a single layer of columnar
epithelium and has gland that dip into myometrium
The endometrium undergo cyclical change during menstrual cycle vary
in thickness between 1-5 mm
The cervix:
Its narrow than the Uterus and about 2.5 cm in length, the ureter run about
one cm lateral to the cervix. The cervical epithelium has numerous deep
Glandular Follicles that secrete a clear alkaline mucous which is the main
compound of physiological vaginal discharge
Epithelial lining of the cervix is:
Ciliated epithelium --at the upper 2/3
Stratified squamous epithelium
— at the lower 1/3 (& area of external os)
The squamocolumor junction SCJ known as the transformation zone (TZ) this
area of rapid cellular division and about 90% of CA-cervix arise from this area
5
Position of uterus
The longitudinal axis of the uterus is at right angle to the vagina and tilted
forward so it's anteverted
The uterus is flex forward on itself at the isthmus so it is anteflexed
In about 20% of women, the Uterus is retroverted retroflex and this is not
pathological
Age changes
1- the vulva
Before puberty
—the skin devoid from the hair
After menopause-the skin atrophied and become thinner
2- the vagina
Before puberty and after menopause the estrogen level is low so there is
low glycogen, the vaginal wall epithelium is atrophy and has high PH.
After menopause the vaginal wall atrophied and shrinkage
3- the uterus
The disappearance of maternal osterogen
the Uterus decrease size
by around 1/3 and in weight by 1/2 and the cervix is then twice length of
the uterus
After menopause the uterus atrophies and the mucosa become very thin
the gland almost disappear and the wall less muscular.
The Fallopian Tube
Each fallopian tube extend from the uterus cornu to end near the ovary and
open into peritoneal cavity. It convey the ovum from the ovary toward the
uterus, which provide oxygenation and nutrition for sperm and ovum.
Each tube is about 10 cm length and consist of 4 parts start from the uterus
side are interstitial , isthmus , ampullary and fimbrial or infundibulum which
open into peritoneal cavity , the inner surface of the fimbria is covered by
ciliated epithelium , the tube consist of muscular layer (outer longitudinal &
inner circular muscle ) + epithelial lining
There is no submucosa or glands
6
The ovaries:
The size depend on the age and stage of menstrual cycle
In the child - its small size about 1.5 cm
In the adult -its almond in shape about 3 cm length
×1.5cm width×1 cm
thickness
The ovary increase size in the months precede puberty, this occur because of
proliferation of stromal cell + maturation of ovarian follicle
The ovary is the only intra-abdominal structure not covered by peritoneum.
Each ovary attach to the Uterus by ovarian ligament and to the broad ligament
by mesovarium which contain the supplying blood vessels and nerves.
Structure of the ovary
It consist of centrally located medulla which consist of loose connective tissue
+ outer cortex
Ovary covered by a single layer of cuboidal cell, the germinal epithelium.
At the birth, numerous primordial follicles are present usually in the cortex
With the puberty, some form each month, the Graafian follicle which after
ovulation leave what it is called the corpus luteum & the atretic follicle form
corpus albicans.
The ureter
As the ureter cross the brim of the pelvis it lie in front of the bifurcation of the
common iliac artery, it turn downward on the lateral wall of the pelvis to reach
the pelvic floor then it descend downward to pass below the uterine artery,
finally it run close to the lateral vaginal fornix to enter the trigon of the bladder
Blood supply is derived from branch of uterine, ovarian, vesical arteries
Pelvic diaphragm
Is form by levator ani muscle, which is broad flat muscle, arise from the lower
part of the body of the pubis and the pelvic surface ischial spine, so the
muscle describe into two parts: .puboCoccygeus & ilioCoccygeus.
7
It act as support for pelvic and abdominal viscera. Nerve supply from S3, S4
Urogenital diaphragm
Lie below the levator ani & consist of two layer of pelvic fascia
Perineal body
This is the Perineal mass of muscular tissue that lie between the anal canal
and lower third of the vagina
Pelvic peritoneum
The peritoneum is reflected from the lateral border of the Uterus to form , on
either side, a double fold of peritoneum, which is named the broad ligament, it
is not a ligament, but it is a fold of peritoneum that is not support the uterus
Ovarian ligament
Lie beneath the posterior layer of broad ligament & pass from the medial
border of the ovary to the uterus.
Round ligament:
It pass from the lateral side of the uterus beneath the anterior leaf of
peritoneum & descend to enter the inguinal canal ending into subcutaneous
tissue of labia major
Cardinal ligament: (named transvers cervical ligament)
Is the condensation or thinking of the fold of broad ligament at its lower portion
and connect the cervix to the lateral pelvic wall provide support to the uterus.
Blood supply:
The Ovary---supply by ovarian artery, which is a branch from the aorta just
below the renal artery.
Internal iliac artery (hypogastric Artery): it is about 4 cm in length & begin at
the bifurcation of common iliac artery in front of the sacroiliac joint
It divided to anterior & posterior division; the branches that supply the pelvis
are all from the anterior division.
The uterine artery provide the main blood supply to the uterus.
Pelvic vein drainage:
1- Of the Uterus, Vagina, Vesical plexus drain into
—internal iliac vein.
8
2- of the ovaries -
ovarian vein
left side
left renal vein
Right side
IVC
Lymphatic drainage
1- from the vulva +perineum---superficial inguinal lymph node + femoral
lymph node
2- vagina :
Lower 1/3....superficial inguinal L.N
Upper 2/3 ...internal +external iliac L.N
3- Cervix ---Obturator + internal & external iliac + common iliac L.N. & lower
paraAortic L.N.
4- uterus--- internal ,external iliac + common iliac L.N + paraAortic L.N
5- Ovary +fallopian tube --- paraAortic L.N.
6- Bladder +urethra ---iliac L.N.
Nerve Supply of the Pelvic
The main supply of the pelvis is the Pudendal N. arise from the 2
nd
, 3
rd
, 4th
sacral nerve
Nerve supply of the vulva & perineumPudendal nerve, which pass along the
outer wall of ischiorectal fossa, it devided to the perineal nerve and dorsal
nerve of clitoris.
The main nerve supply of levator ani is S3, S4
Nerve supply of the pelvic viscera:
The uterus & cervix nerve supply inferior hypogastric plexus
The ovary nerve supply ovarian plexus
The myometrium has both α & β- adrenergic receptor & cholinergic receptor.
So that a β- sympathomimetic drugs lead to myometrial relaxation.