Dr.Mushtaq Talib Hussein
F.I.B.M.S(ortho.) C.A.B.O(ortho.)
Elbow dislocation
Dislocation of the ulno-_humeral joint is fairly common more so in adults than in
children. Injuries are usually classified according to the direction of the displacement.
However, in 90% of cases the radio- ulnar complex is displaced posteriorly or
posterolaterally ,often together with fractures of the restraining bony processes.
Mechanism of injury
Elbow dislocations typically occur when a person falls onto an outstretched hand. When the
hand hits the ground, the force is sent to the elbow. Usually, there is a turning motion in this
force. This can drive and rotate the elbow out of its socket.
Elbow dislocations can also happen in a high energy trauma , a classic example is the so
called sideswipe injury in which a car_driver,s elbow, protruding through the window ,is
struck by another vehicle.
The result is forward dislocation with fractures of any or all of the bones around the elbow,
neurovascular injuries.
Clinical features
A complete elbow dislocation is extremely painful and very obvious. The arm will look
deformed and may have an odd twist at the elbow.
The doctor will examine the arm. He will check for tenderness, swelling, and deformity. He
will evaluate the skin and circulation to the arm. Pulses at the wrist will be checked.
It is also important to check the nerve supply to the hand. If nerves have been injured during
the dislocation, some or all of the hand may be numb and not able to move.
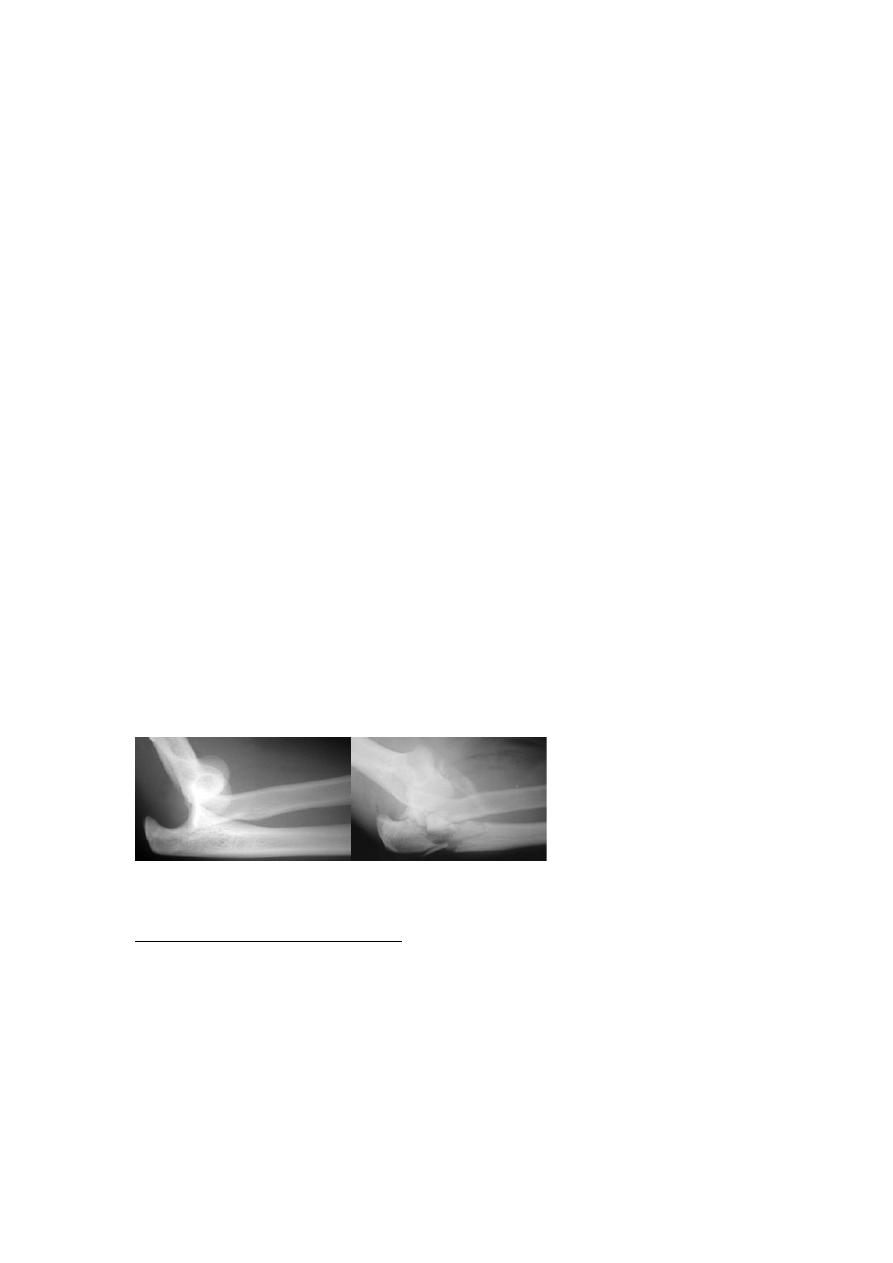
X_ray
An X-ray is necessary to determine if there is a bone injury. X-rays can also help show the
direction of the dislocation.
X-rays are the best way to confirm that the elbow is dislocated. If bone detail is difficult to
identify on an X-ray, a computed tomography (CT) scan may be done.
If it is important to evaluate the ligaments, a magnetic resonance image (MRI) can be
helpful.(complex dislocations) .
Simple complex dislocation
Treatment
Uncomplicated(simple )dislocation
An elbow dislocation should be considered an emergency injury. The goal of immediate
treatment of a dislocated elbow is to return the elbow to its normal alignment. The long-
term goal is to restore function to the arm.
Under anaesthesia closed reduction (traction,flexion and olecranon process pushed forward
with thumbs).
Elbow should be in full range of movement ,then check the neurovascular function. Arm
held in elbow flexion above 90 degrees for 3 weeks ,then elbow movement are allowed
to return spontaneously and are never forced.
Complex dislocation(associated with fractures)
*Coronoid process fractures (which could be either avulsion pf the tip, single less than 50% ,
or comminuted more than 50% of the process) usually in such cases need close reduction of
elbow dislocation with open reduction and internal fixation of coronoid process especiallyif
it is more than 50% of the process.
*medial epicondyle with medial ligament disruption , it will need open reduction and
internal fixation.
*head of radius especially when associated with medial ligament disruption it will be
unstable elbow joint , so the treatment will be open reduction of radial head fracture with
medial collateral ligament repair.
*side_swipe injuries these usually associated with vascular and severe soft tissues injury,
priority should be to vascular repair with soft tissue coverage and skeletal stabilization.
Complications
Early
Vascular injury
Brachial artery injury is matter of emergency , absence of radial pulse with signs of
ischaemia necessitate urgent arteriogram and exploration with vascular repair.
Nerve injury the median or ulnar nerve is sometimes injured. Spontaneous recovery
usually occurs after 6_8 weeks.
Late
Stiffness loss 0f 20 to 30 degrees of extension is not uncommon after elbow dislocation.
So to treat elbow injuries u need to avoid passive stretching, and start early as possible
elbow movement and exercises.
Heterotopic ossification(myositis ossificans) may occur in the damaged soft tissue in
front of the joint . it is due to muscle bruising or haematoma formation.
NSAIDS may be helpful in early cases , otherwise surgery sometimes needed to excise
mature well formed bone mass.
Unreduced dislocation a dislocation may not have been diagnosed or there were just
elbow subluxation . up to 3 weeks there is possibility of closed reduction otherwise
surgery indicated to reduce the elbow joint.
Recurrent dislocation is rare unless there is larg coronoid fracture or radial head
fracture.
Osteoarthritis is quite common after severe fracture_dislocations. In older patients,
total elbow replacement can be considered.
Olecranon Fracture
Olecranon fracture is a fracture involving the olecranon process of the ulna bone. This
process forms a part of the elbow joint that articulates with the trochlea of the humerus
bone. (intra_articular fracture)
Mechanism of injury
This fracture occurs in two ways
(1)fall on the tip of the elbow joint (comminuted fracture: displaced and undisplaced)
(2)sudden forceful contraction of the triceps muscle (the muscle pulls the bone
fragment apart)_ transverse fracture: displaced and undisplaced.
Clinical features
Symptoms include
•
history of trauma is present
•
pain and swelling in and around the elbow joint
•
inability to extend the elbow against gravity
•
tenderness is present at the fracture site
•
sometimes gap is felt when there is displaced transverse fracture
•
check the radial head, sometimes is dislocated(Montegia fracture_dislocation).
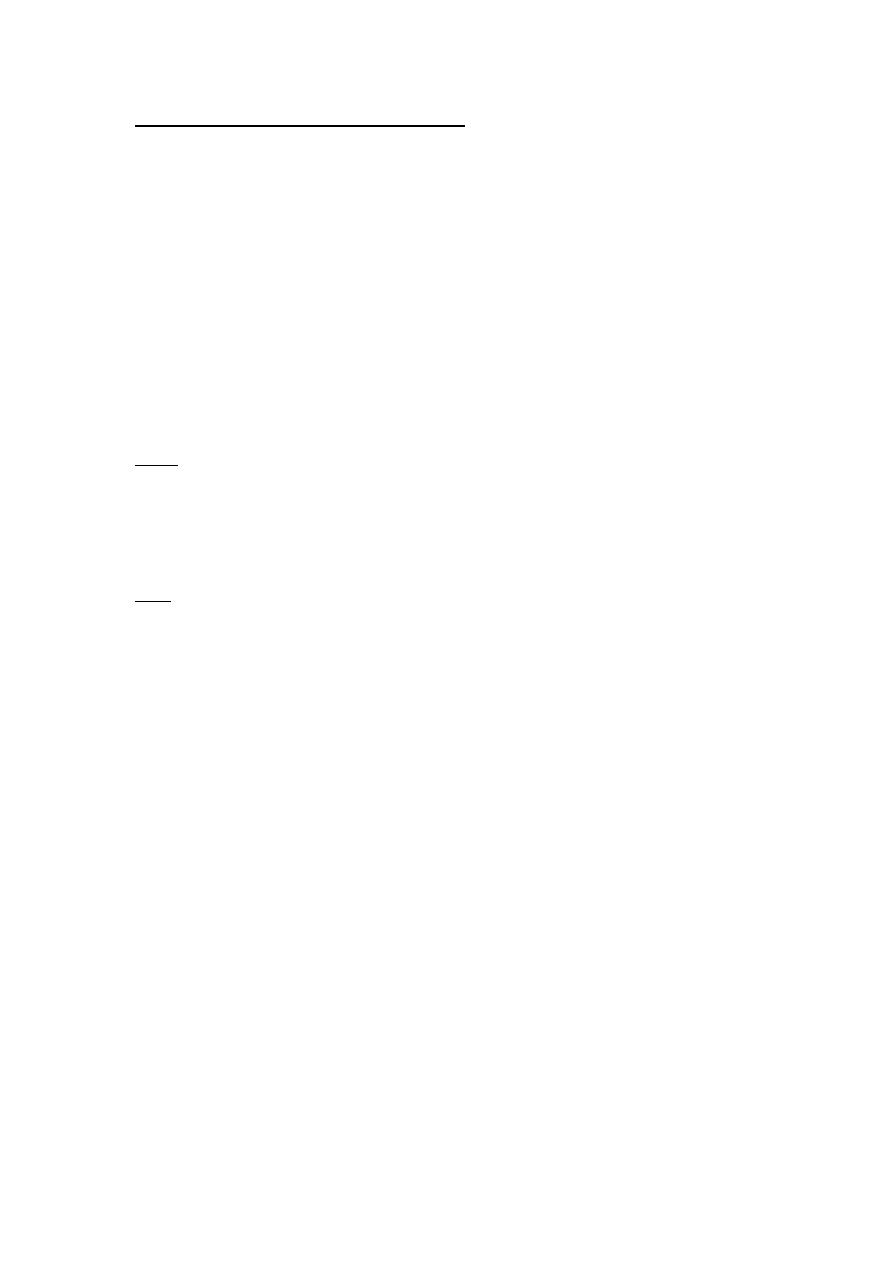
X_ray
Lateral view will reveal the fracture type and if displaced or not and radial head if
dislocated or not.
Treatement
All undisplaced fractures are treated by immobilization in a plaster splint for 3 weeks. The
elbow should immobilized at 45 degrees of flexion. After 7 to 10 days of immobilization a x
ray is done to confirm the position of the fracture.
In elderly patients (beyond 60 years) the elbow is rested in a sling. A mild crepe bandage is
wrapped gently around the elbow and pain killer are given. Once pain has decreased, gentle
movements are encouraged in a brace.
All displaced fractures are treated operatively by fixation with wires, screws or plates. The
fixation should be strong enough for early active mobilization of the elbow joint. This
prevents the elbow from becoming stiff.
Complications
Include:
( 1) loss of some movement of the elbow( joint stiffness) , to be avoided need early
mobilization with rigid internal fixation.
(2 ) non union of the fracture can occur when undisplaced fracture becomes displaced and
goes unrecognised
(3) arthritis of the elbow joint especially if reduction is less than perfect.
Radial Head Fracture
Radial head fracture is a fracture of the upper end of the radius bone where it articulates
with the lower end of the humerus bone. It common in adults but are hardly ever seen in
children(probably because the proximal radius is mainly cartilaginous) whereas radial neck
fractures occur in children more frequently.
Mechanism of injury
(1) fall on the outstretched hand with elbow extended and the forearm pronated causes
impaction of the radial head against the capitulum.
) 2)along with dislocation of the elbow joint .
Clinical features :Symptoms include
history of trauma
pain in the outer aspect of the elbow joint
mild swelling may be present
movements of the elbow joint may be painful and limited ( especially pronation and
supination )
wrist pain may be present (indicates a Essex-Lopresti injury).
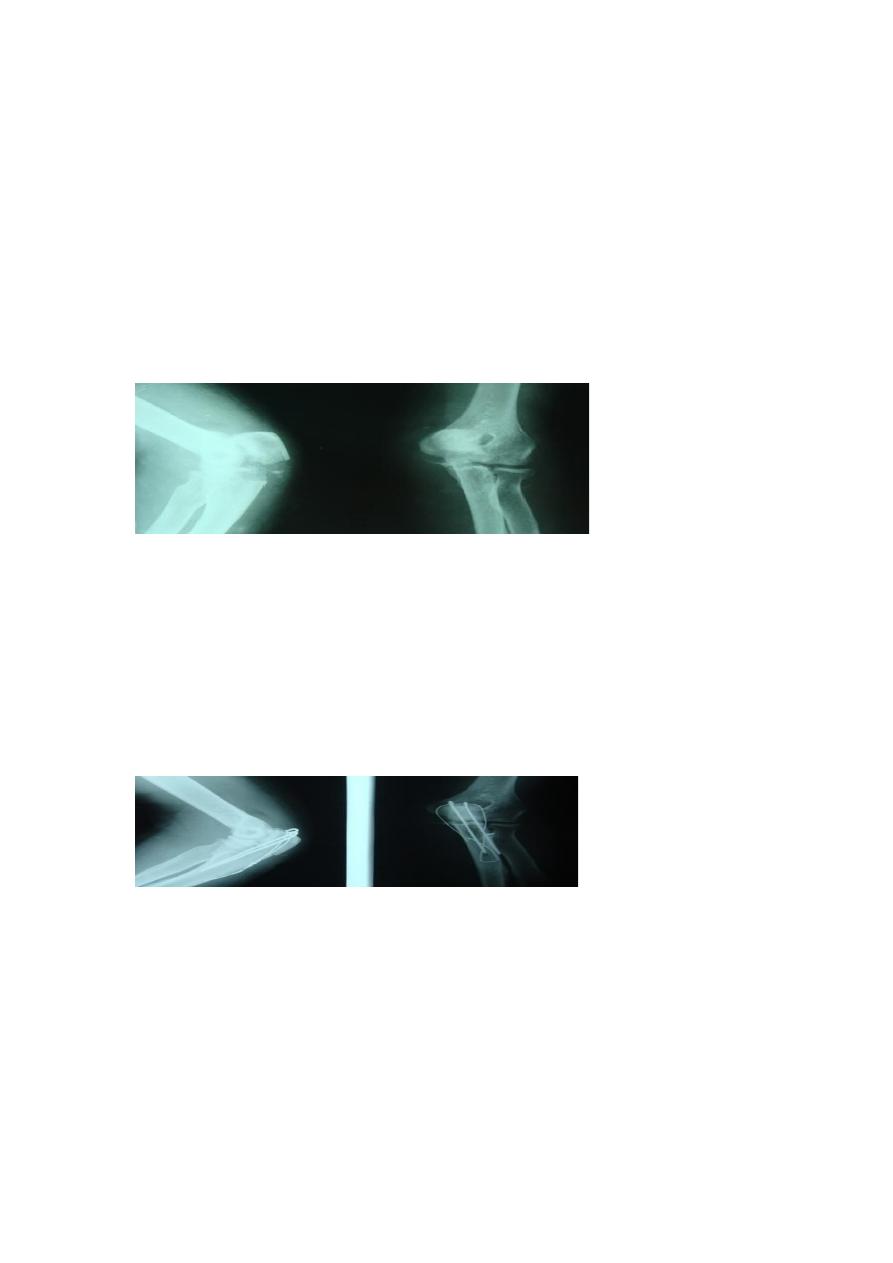
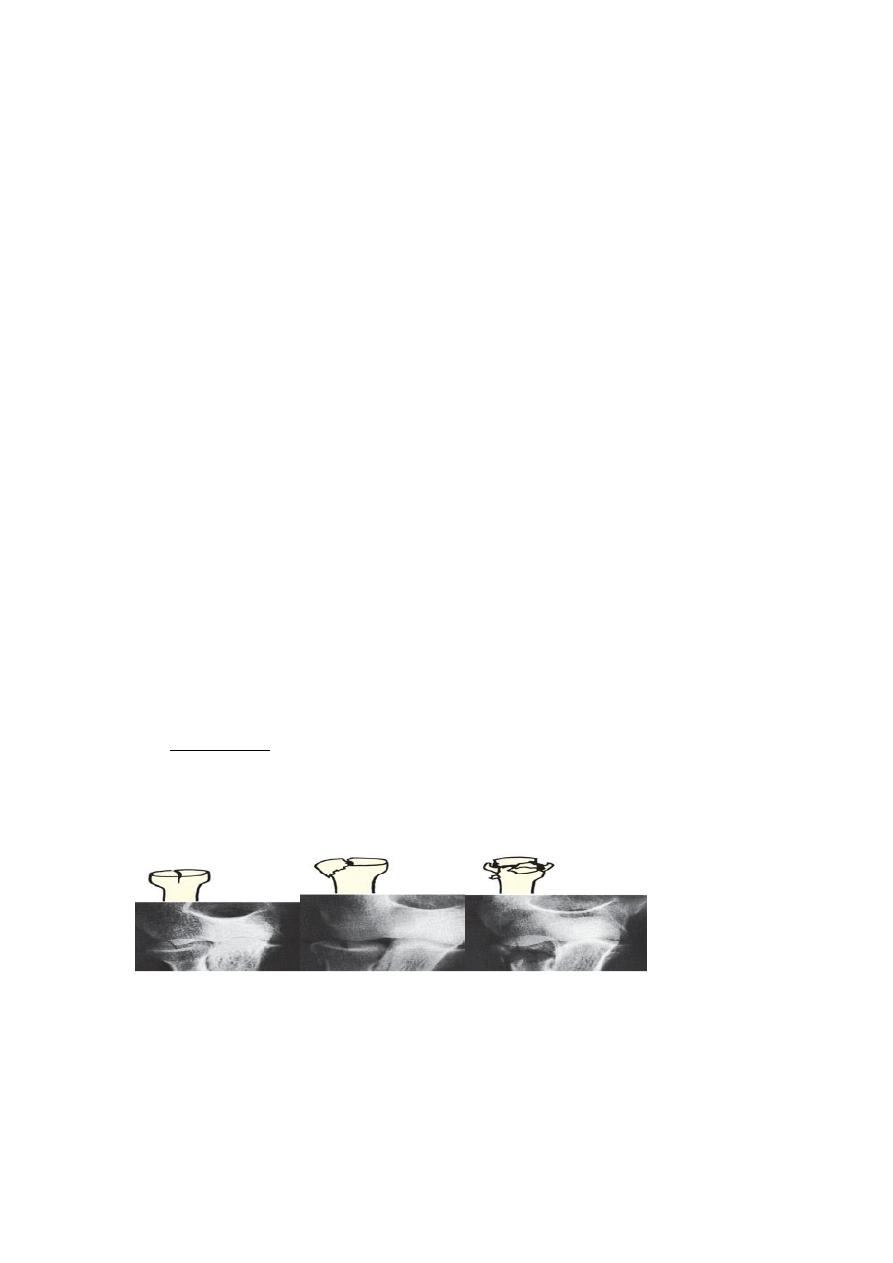
X-ray
Three types of fracture are identified and classified by Mason as:
Type I An undisplaced vertical split in the radial head
Type II A displaced single fragment of the head
Type III The head broken into several fragments (comminuted).
An additional Type IV has been proposed, for those fractures with an associated elbow
dislocation.
Lat.,Ap. Views, with x-ray_wrist joint to assess distal R_U joint .
Treatment
An undisplaced split (Type I) Worthwhile pain relief can be achieved by aspirating the
hematoma and injecting local anesthetic.
The arm is held in a collar and cuff for 3 weeks; active flexion, extension and rotation are
encouraged. The prognosis for this injury is very good.
A single large fragment (Type II) If the fragment is displaced, it should be reduced and held
with one or two small headless screws.
A comminuted fracture (Type III) This is a challenging injury. Always assess for an associated
soft tissue injury:
(1)Rupture of the medial collateral ligament;
(2)Rupture of the interosseous membrane (Essex Lopresti lesion);
(3)Combined fractures of the radial head and coronoid process plus dislocation of the elbow
– the‘terrible triad’.
If any of these is present, excision of the radial head is contra-indicated; this may lead to
intractable instability of the elbow or forearm.
The head must be meticulously reconstructed with small headless screws
or replaced with a metal spacer.
A medial collateral, should be repaired.
Complications
Joint stiffness is common and may involve both the elbow and the radioulnar joints.
Myositis ossificans is an occasional complication.
Recurrent instability of the elbow can occur if the medial collateral ligament was also
injured and the radial head excised.
FRACTURE OF THE RADIAL NECK
In adults, a displaced fracture of the radial neck may need open reduction; if so, a mini-
plate can be applied, making sure not to damage the articular surface.
An alternative is to use oblique headless screws.